
Surgical fixation of unstable intertrochanteric femur fractures with a long proximal femoral nail results in significant improvements in pain, mobility, hip-related QoL, and a high level of patient satisfaction at mid-term follow-up.
Dr. R R Rajkumar, Department of Orthopaedics, Vinayaka Mission’s Kirupananda Variyar Medical College and Hospital, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: rrrajkumar66@gmail.com
Abstract
Introduction: As the world’s population ages, hip fractures become more common. The global incidence of hip fractures will rise to a million per year by 2040. Intertrochanteric femoral fractures are common fracture in older people, typically caused by low-energy falls. These fractures are also classified based on their stability, with unstable fracture patterns posing more challenges for surgical therapy and potentially resulting in worse functional recovery. Surgical fixation is the most effective treatment for these fractures since it restores motion while reducing complications. Intertrochanteric fractures occur between the lesser and greater trochanters of the femur. Unstable intertrochanteric fractures exhibit medial cortical comminution, fracture planes with reverse obliquity, and subtrochanteric extension. These characteristics contribute to the difficulty of achieving and maintaining reduction, as well as the likelihood of malunion, non-union, and eventual functional limitation.
Aims and Objectives: To evaluate the functional outcomes of patients with unstable intertrochanteric femur fractures who undergo surgical treatment using a long proximal femoral nail (PFN) and to assess complication rates, radiographic evaluation, return to daily activities, and patient satisfaction.
Materials and Methods: This prospective cross-sectional study was conducted in the Department of Orthopaedics, Vinayaka Mission’s Kirupananda Variyar Medical College, from November 2022 to September 2025. Thirty patients aged above 18 years presenting with unstable intertrochanteric femur fractures (Boyd and Griffin types I–IV) were included and treated surgically with a long PFN.
Results: The mean Harris Hip score (HHS) at the 3rd and 6th months after surgery was 75 ± 7.5 (72–77) and 87 ± 6.6 (84–89), respectively, with a statistically significant (P < 0.001) improvement. A significant (P < 0.05) increase in proportion from 3% in 3 months to 40% in 6 months in an excellent HHS. The mean hip disability and osteoarthritis outcome score (HOOS)-12 pain, function, quality of life (QoL), and summary of the study participants at the pre-operative stage were 29.2 ± 3.9, 34.6 ± 5.8, 26.3 ± 7, and 30 ± 5.4, respectively. In the 3rd and 6th months, there were significant improvements in all domains of the HOOS-12 score.
Conclusion: The HHS was significantly increased at 6 months compared to HHS at 3 months. All the domains (pain, function, QoL, and summary) of the HOOS-12 and Visual Analog Scale pain scores increased significantly at the 3rd and 6th months from pre-operative.
Keywords: Unstable intertrochanteric femur fracture, long proximal femoral nail, functional outcome, Harris Hip Score, hip disability and osteoarthritis outcome score-12, Visual Analog Scale pain score, surgical fixation, hip fracture.
As the world’s population ages, hip fractures become more common. The global incidence of hip fractures will rise to 6 million per year by 2040 [1]. Intertrochanteric femoral fracture is a common fracture in older people, typically caused by low-energy falls. These fractures are also classified based on their stability, with unstable fracture patterns posing more challenges for surgical therapy and potentially resulting in worse functional recovery [2]. Surgical fixation is the most effective treatment for these fractures since it restores motion while reducing complications. Intertrochanteric fractures occur between the lesser and greater trochanters of the femur [3]. Unstable intertrochanteric fractures exhibit medial cortical comminution, fracture planes with reverse obliquity, and subtrochanteric extension. These characteristics contribute to the difficulty of achieving and maintaining reduction, as well as the likelihood of malunion, non-union, and eventual functional limitation. Hip fractures are a major global health problem, with the intertrochanteric fracture accounting for more than half of all fractures. Hip fractures will increase to 4.5 million by 2050, driven primarily by an increasing older population worldwide and an increased prevalence of osteoporosis [4,5]. Intertrochanteric fractures will become more common over the next few decades, with an estimated 7 million occurring each year. The study’s findings show that around 30% of intertrochanteric fractures are unstable. Hip fractures are expected to impact more than 120/100,000 people over the age of 50 in India each year. In 2004, a survey indicated that there were 600,000 osteoporotic hip fractures in India per year, with a dramatic increase expected by 2026. Indian research has revealed that roughly 30% of intertrochanteric fractures are unstable [6,7]. Long proximal femoral nails (PFNs) are one of the most often used implants for surgical stabilization of intertrochanteric fractures, particularly unstable forms, since they provide better distal fixation and rotational stability. The long PFN penetrates deeper into the femoral shaft, beyond the isthmus, and has more stability than shorter nails. This extra distal fixation is potentially favorable in unstable fracture patterns, particularly those with subtrochanteric extension, because it improves rotational stress control and prevents distal fragment displacement [8,9]. The longer nail also provides more surface area for bone-implant interaction, which promotes healing and reduces the likelihood of implant failure in complex fracture patterns. Longer PFNs provide more stability and aid in fracture reduction in unstable intertrochanteric fractures than shorter implants. This stability can lead to better healing and functional recovery. Applying a long PFN in unstable patterns reduces the likelihood of problems such as lag screw cut-out and distal fragment rotation compared to using shorter nails or a dynamic hip screw in specific forms of fracture [10]. Functional effects of extended PFN fixation are determined by the nature of the unstable intertrochanteric fracture. For example, fractures with significant comminution or subtrochanteric extension might cause problems and result in inferior outcomes even when a long nail is implanted [11]. More research in various populations will be required to determine that extended PFN is clearly superior to other methods of treatment in certain unstable intertrochanteric fractures. To optimize treatment methods, we will identify patient- and fracture-specific factors that potentially predict functional results after long-term PFN fixation. It has been demonstrated to provide stability and perhaps aid in the reduction of fractures, which could result in improved functional outcomes. However, a variety of factors determine the best implant choice, including fracture type, patient comorbidities, and surgeon expertise. The study’s goal is to offer definitive information about the functional results and relative efficiency of the long PFN in stabilizing unstable intertrochanteric femoral fractures.
Primary objective
The primary objective of this thesis is to evaluate the functional outcome of patients undergoing total hip arthroplasty. The functional outcome will be assessed using various measures such as mobility, pain level, and quality of life (QoL) indicators.
Secondary objective
To get the full functions of the hip.
Study design
Prospective cross-sectional study
Study period
Two years.
Study population
Patients diagnosed with unstable intertrochanteric femur fractures.
Study duration
November 2022–September 2025.
Place of study
Department of Orthopedics, Vinayaka Missions Kirupananda Variyar Medical College. The study received approval from the Institutional Ethics Committee of Vinayaka Mission’s Kirupananda Variyar Medical College and Hospitals, Salem, with IEC approval number VMKVMC&H/IEC/23/096 dated September 14, 2023, and the committee granted permission for the project to be conducted at the institution while advising adherence to ICMR biomedical research guidelines and Good Clinical Practice, timely reporting of any adverse events, and submission of the final report upon completion of the study.
Inclusion criteria
Patients >18 years of age presenting to our casualty with intertrochanteric femoral fractures with all Boyd and Griffin types (1–4), planned for surgical correction with long PFN, both displaced and undisplaced fractures, fractures <1 week duration, and without any other associated fractures were included in the study.
Exclusion criteria
Fractures with non-union changes, old malunited intertrochanteric fractures, and patients with arthritic changes in the hip joint, pathological fractures were excluded from the study.
Sample size
Maximum of 30 patients.
Mode of injury
Nearly two-thirds (19, 63%) of the study participants had a fall as the mode of injury for the fracture. AO type Nearly one-third (10, 33%) of the study participants had AO type 31A2.2, and 8 (27%) had 31A2.3.
Fracture reduction
The majority (28, 93%) of the study participants had closed reduction surgery for fracture correction.
Surgery time and complications
The average surgery time was 49 min, and the average blood loss was 216 mL. More than three-fourths (23, 76%) of the study participants had no intraoperative complications. Two-thirds (20, 67%) of the study participants had no post-operative complications.
Harris hip score (HHS)
The mean HHS of study participants increased after 3 months to 6 months of surgery (P <0.001) (Tables 1 and 2).
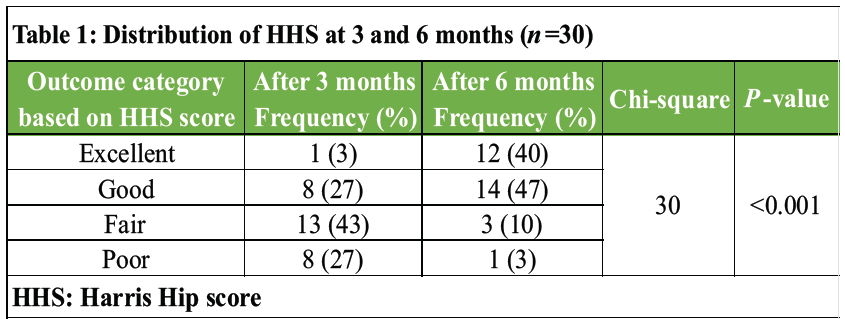
Table 1: Distribution of HHS at 3 and 6 months (n=30)
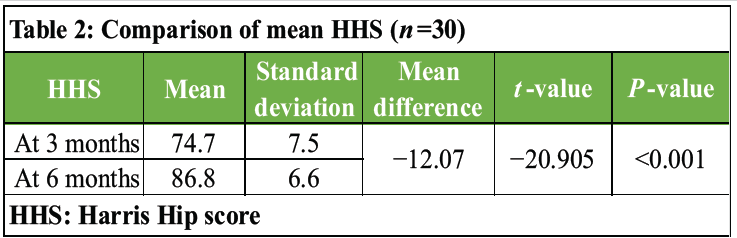
Table 2: Comparison of mean HHS (n=30)
The mean hip disability and osteoarthritis outcome score (HOOS)-12 score of the study participants in pain, function, and QoL increased significantly after surgery, 3 months, and 6 months, respectively (P <0.001) (Tables 3 and 4).
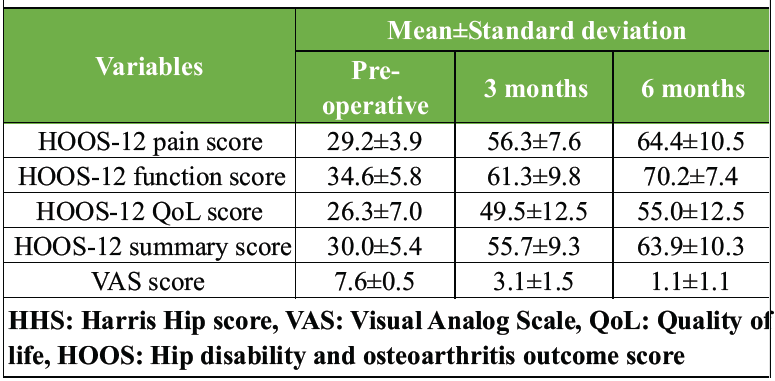
Table 3: Comparison of mean HOOS-12 and VAS scores pre-operative, 3 months, and 6 months (n=30)
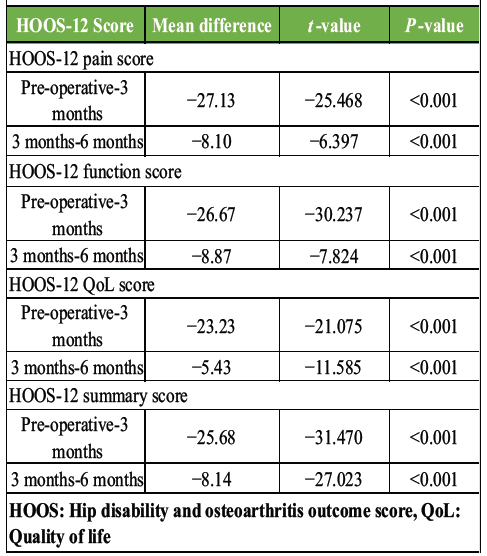
Table 4: Comparison of HOOS-12 scores by T-test
Visual Analog Scale (VAS) pain score
The mean VAS pain score of the study participants in pain, function, and QoL decreases significantly after surgery, 3 months, and 6 months, respectively (P < 0.001) (Table 5).
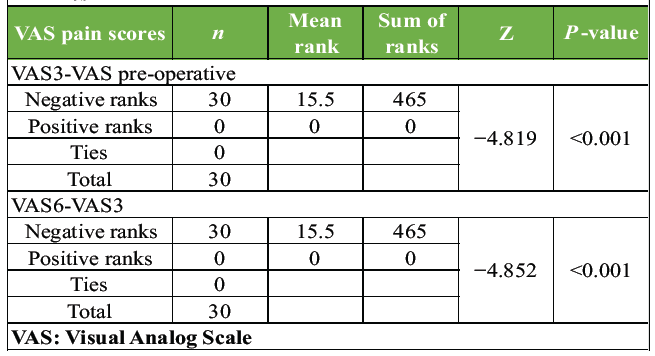
Table 5: Comparison of VAS pain scores by the Wilcoxon signed rank test
Comparison of outcome
The mean HHS, HOOS-12 pain, function, QoL, summary, and VAS pain scores among the satisfied study participants (26, 87%) at 6 months after surgery were 88.7 ± 4.5, 65.5 ± 10.8, 72 ± 5.8, 58.1 ± 10, 66.3 ± 8.8, and 0.8 ± 0.8, respectively; those of the not satisfied participants were 74.5 ± 4.2, 57.3 ± 3.6, 58 ± 4.3, 34.8 ± 6.3, 48.3 ± 3.2, and 3 ± 0.01, respectively (Table 6).
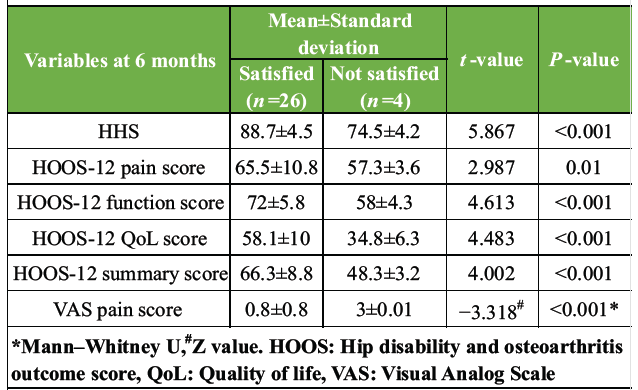
Table 6: Comparison of study outcome with patient satisfaction (n=30)
Follow-up and overall satisfaction
The mean follow-up duration was 10.5 ± 2.4 months, with a maximum of 15 months for 2 (7%). 26 (87% [69–98]) study participants had overall satisfaction at the end of follow-up after surgery. Thus, the mean outcome scores after 6 months of surgery were significantly (P <0.05) higher among satisfied study participants than among not satisfied participants.
This prospective cross-sectional study in the Department of Orthopaedic at Vinayaka Missions Kirupananda Variyar Medical College was done to evaluate the functional outcome and patient satisfaction among 30 willing patients with unstable intertrochanteric femur fractures who underwent surgical treatment using a long PFN. The functional outcome, such as mobility, pain levels, and QoL indicators, was assessed using the HHS, HOOS-12 score, and VAS pain score. The results of the study were discussed below:
Basic details
The mean ± standard deviation age of the study participants was 67 ± 12 years (63–71). 73% (54–88) were females. 63% (19) had falls, and 37% (11) had a road traffic accident as the mode of injury, causing unstable intertrochanteric femur fracture. The sides (right/left) were equally distributed (50% each) among the study participants. 33% (10) had a fracture of 31A2.2, and 27% (8) had 31A2.3 as per the AO classification.
Details of surgery
28 (93%) had closed, and 2 (7%) had open surgical reduction for fracture treatment. The mean time duration of surgery was 49 ± 7 min. The mean blood loss during surgery was 216 ± 39 mL. Intraoperative complications were fracture displacement (10%), reduction failure (7%), and varus angulation (7%). 23 (77%) had no intraoperative complications.
Post-operative follow-up
The post-operative complications were infection (13%), varus collapse (10%), implant failure (3%), Z effect (3%), and malunion/deformity (3%). 20 (67%) had no post-operative complications. The complications were appropriately treated. All the study participants had fractures united radiologically. The average time taken for fracture union was 14 ± 1.3 weeks. The mean duration of follow-up was 10.5 ± 2.4 months.
Study outcome
The functional outcomes of the study were assessed by the HHS, HOOS-12 score, and VAS pain score. The mean HHS at the 3rd month and 6th month after surgery were 75 ± 7.5 (72–77) and 87 ± 6.6 (84–89), respectively, with a statistically significant (P < 0.001) improvement. Nishanthan V et al. [12]. The study showed a mean difference of −5.43 (−18.06) in the HHS for 3 and 6 months, which is similar to our study with an HHS mean difference of −12.04 for 3 and 6 months after surgery. The study by Nishanthan et al. [12] showed significant improvement in the proportion of patients undergoing long PFN by an excellent HHS functional outcome score from 3 months (8%) to 6 months (42%). This is similar to our study findings of a significant (P < 0.05) increase in proportion from 3% in 3 months to 40% in 6 months in an excellent HSS. The study by Rahman et al. [13] showed a final follow-up mean HHS in patients with long PFN for unstable intertrochanteric fracture of 81 ± 11.6, a mean fracture union time of 15.7 ± 2.7 weeks, which is similar to our study result of a mean HHS of 87 ± 6.6 at 6 months of follow-up and a mean fracture union time of 14 ± 1.3 weeks. The mean HOOS-12 pain, function, QoL, and summary of the study participants at the pre-operative stage were 29.2 ± 3.9, 34.6 ± 5.8, 26.3 ± 7, and 30 ± 5.4, respectively. In the 3rd and 6th months, there were significant improvements in all domains of the HOOS-12 score. The mean VAS pain scores at pre-operative, 3 months, and 6 months after surgery were 7.6 ± 0.5 (7.4–7.8), 3.1 ± 1.5 (2.5–3.7), and 1.1 ± 1.1 (0.7–1.5), respectively, with a statistically significant decrease in the mean VAS pain score (P < 0.05). Thus, pain decreases after surgery with long PFN. The mean HHS, HOOS-12 pain, function, QoL, summary, and VAS pain score 6 months after surgery were 88.7 ± 4.5, 65.5 ± 10.8, 72 ± 5.8, 58.1 ± 10, 66.3 ± 8.8, and 0.8 ± 0.8, respectively; in participants who were not satisfied, they were 74.5 ± 4.2, 57.3 ± 3.6, 58 ± 4.3, 34.8 ± 6.3, 48.3 ± 3.2, and 3 ± 0.01, respectively. The HHS, HOOS-12, and VAS pain scores were better in satisfied participants than in not satisfied ones, with a statistically significant difference (P < 0.05). The study by Chen et al. [14] showed that surgical correction by long PFN was better for unstable intertrochanteric fractures. Kim et al. [15] study showed that surgical correction for unstable intertrochanteric fracture with long PFN had a good functional outcome, which is similar to our study result.
The study was done to evaluate functional outcomes such as pain, mobility, and QoL among 30 patients with unstable intertrochanteric fractures undergoing surgical treatment with long PFN. The functional outcomes were evaluated at pre-operative, 3 months, and 6 months after surgery with HOOS-12 scores, VAS pain analog scores, and HHS. The HHS was significantly increased at 6 months compared to HHS at 3 months. All the domains (pain, function, QoL, and summary) of the HOOS-12 and VAS pain scores increased significantly at the 3rd and 6th months from pre-operative. All the study participants had radiological union and returned to daily activities at the end of their follow-up period. 87% (26) of the study participants had overall perceived satisfaction at the end of follow-up of the surgery with long PFN for their unstable intertrochanteric fracture, which was evident in their functional outcome assessment. Thus, functional outcomes such as pain levels, mobility, and hip-related QoL improved after surgery with long PFN. The radiological union, return to daily activity, and patient satisfaction were also better after surgery.
Study limitations
A multicentric study with a larger sample size could shed more insight into outcomes. Research with a control group may also be useful for comparing benefits.
Long proximal femoral nailing provides stable fixation for unstable intertrochanteric femur fractures, facilitating early mobilization, reliable fracture union, significant improvement in functional outcomes, and high patient satisfaction when combined with meticulous surgical technique and structured post-operative rehabilitation.
References
- 1. Veronese N, Kolk H, Maggi S. Epidemiology of Fragility Fractures and Social Impact. In: Falaschi P, Marsh D, editors. Orthogeriatrics: The Management of Older Patients with Fragility Fractures. 2nd ed. Cham, CH: Springer; 2021. Available from: http://www.ncbi.nlm.nih.gov/books/nbk565577 [Last accessed on 2025 Mar 16]. [Google Scholar] [PubMed]
- 2. Attum B, Pilson H. Intertrochanteric Femur Fracture. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2025. Available from: http://www.ncbi.nlm.nih.gov/books/nbk493161 [Last accessed on 2025 Mar 16]. [Google Scholar] [PubMed]
- 3. Fracture of Greater Trochanter – an Overview. ScienceDirect Topics. Available from: https://www.sciencedirect.com/topics/medicine-and-dentistry/fracture-of-greater-trochanter [Last accessed on 2025 Mar 16]. [Google Scholar] [PubMed]
- 4. Yıldırım C, Muratoğlu OG, Turan K, Ergün T, Mısır A, Aydın M. The intra- and interobserver reliability of five commonly used intertrochanteric femur fracture classification systems. Jt Dis Relat Surg 2022;33:187-92. [Google Scholar] [PubMed]
- 5. Fragility Fractures. Available from: https://www.who.int/news-room/fact-sheets/detail/fragility-fractures [Last accessed on 2025 Mar 16]. [Google Scholar] [PubMed]
- 6. George J, Sharma V, Farooque K, Trikha V, Mittal S, Malhotra R. Excess mortality in elderly hip fracture patients: An Indian experience. Chin J Traumatol 2023;26:363-8. [Google Scholar] [PubMed]
- 7. Shetty V, Agashe V, Shekhar S, Mishra S, Jorule KM, Landge S. Unstable inter-trochanteric femur fracture fixation with PFNA2: Does not require lateral wall fixation – a study of 278 patients. J Orthop Rep 2025;4:100367. [Google Scholar] [PubMed]
- 8. Simmermacher RK, Bosch AM, Van Der Werken C. The AO/ASIF-proximal femoral nail (PFN): A new device for the treatment of unstable proximal femoral fractures. Injury 1999;30:327-32. [Google Scholar] [PubMed]
- 9. Vaughn J, Cohen E, Vopat BG, Kane P, Abbood E, Born C. Complications of short versus long cephalomedullary nail for intertrochanteric femur fractures, minimum 1 year follow-up. Eur J Orthop Surg Traumatol 2015;25:665-70. [Google Scholar] [PubMed]
- 10. Haentjens P, Casteleyn PP, De Boeck H, Handelberg F, Opdecam P. Treatment of unstable intertrochanteric and subtrochanteric fractures in elderly patients. Primary bipolar arthroplasty compared with internal fixation. J Bone Joint Surg Am 1989;71:1214-25. [Google Scholar] [PubMed]
- 11. Palm H. Hip Fracture: The Choice of Surgery. In: Falaschi P, Marsh D, editors. Orthogeriatrics: The Management of Older Patients with Fragility Fractures. 2nd ed. Cham, CH: Springer; 2021. Available from: http://www.ncbi.nlm.nih.gov/books/nbk565572 [Last accessed on 2025 Mar 16]. [Google Scholar] [PubMed]
- 12. Nishanthan V, Siddarth R, Vijayaraghavan R. Functional outcome of unstable intertrochanteric fracture treated with long PFN with or without augmentation. Int J Orthop Sci 2023;9:200-6. [Google Scholar] [PubMed]
- 13. Rahman MA, Siddiqui YS, Julfiqar M, Khan AQ, Sabir AB, Abbas M. Short versus long proximal femoral nail in the management of intertrochanteric fractures – a comparative study. Int J Burns Trauma 2023;13:99-109. [Google Scholar] [PubMed]
- 14. Chen WH, Guo WX, Gao SH, Wei QS, Li ZQ, He W. Arthroplasty vs proximal femoral nails for unstable intertrochanteric femoral fractures in elderly patients: A systematic review and meta-analysis. World J Clin Cases 2021;9:9878-88. [Google Scholar] [PubMed]
- 15. Kim SY, Kim YG, Hwang JK. Cementless calcar-replacement hemiarthroplasty compared with intramedullary fixation of unstable intertrochanteric fractures. A prospective, randomized study. J Bone Joint Surg Am 2005;87:2186-92. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Comparison of Radial Head Prosthesis versus Excision in Comminuted Radial Head Fractures: A Retrospective Comparative Study
June 1, 2026 Comparison of Radial Head Prosthesis versus Excision in Comminuted Radial Head Fractures: A Retrospective Comparative Study June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study
June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study June 1, 2026 Column Involvement as a Predictor of Early Functional Outcome and Complications in Proximal Tibia Fractures: A Prospective Study
June 1, 2026 Column Involvement as a Predictor of Early Functional Outcome and Complications in Proximal Tibia Fractures: A Prospective Study May 1, 2026 Functional Outcomes and Surgical Utility of the Modified Schatzker Four-column Concept in Proximal Tibial Plateau Fractures: A Prospective Observational Study
May 1, 2026 Functional Outcomes and Surgical Utility of the Modified Schatzker Four-column Concept in Proximal Tibial Plateau Fractures: A Prospective Observational Study