
In patients with isolated medial compartment osteoarthritis, one-stage single-sitting bilateral unicompartmental knee arthroplasty (UKA) provides equivalent mid-term functional outcomes and implant safety compared to unilateral UKA, while enabling faster rehabilitation, earlier return to daily activities, and higher long-term patient satisfaction without increasing hospital stay or complication rates.
Dr. Amyn M Rajani, OAKS Clinic, Mumbai, Maharashtra, India. E-mail: dramrajani@gmail.com
Abstract
Introduction: Unicompartmental knee arthroplasty (UKA) is a joint-preserving surgical option for individuals with isolated medial compartment osteoarthritis (OA). Although performing UKA on both knees in a single sitting can offer logistical benefits, there is limited data comparing its safety and clinical outcomes with unilateral procedures. The objective of this study was to compare the mid-term functional outcomes, recovery parameters, and complication rates between one-stage single-sitting bilateral and unilateral UKA.
Materials and Methods: This observational study included 256 patients diagnosed with medial compartment OA who underwent either one-stage single-sitting bilateral UKA (n = 134) or unilateral UKA (n = 122). Functional outcomes were evaluated using the Oxford Knee Score (OKS), pain levels through the Visual Analog Scale (VAS), range of motion (ROM), post-operative satisfaction, and time to return to regular activities over a 5-year follow-up period.
Results: Significant improvements in OKS, ROM, and VAS scores were observed in both groups (P < 0.001). Patients undergoing one-stage single-sitting bilateral UKA required fewer physiotherapy sessions (17.6 vs. 21.4, P < 0.001) and returned to daily activities earlier (5.2 vs. 6.4 weeks, P < 0.001), without increased hospital stay or complications.
Conclusion: One-stage single-sitting bilateral UKA appears to be a safe and effective treatment strategy for carefully selected patients with medial compartment OA, offering comparable safety and enhanced functional recovery compared to unilateral procedures.
Keywords: Unicompartmental knee arthroplasty, one-stage single-sitting bilateral unicompartmental knee arthroplasty, medial compartment osteoarthritis, functional outcomes, patient satisfaction.
Knee osteoarthritis (OA) is a major global cause of pain and disability [1]. Approximately one in three patients with knee OA has involvement limited to a single compartment, typically the medial compartment. In such cases, unicompartmental knee arthroplasty (UKA) offers a minimally invasive, bone-sparing alternative to total knee arthroplasty (TKA), with consistent outcomes in terms of pain reduction and functional gains [2]. Compared to TKA, UKA has been associated with quicker postoperative recovery, reduced blood loss, fewer perioperative complications, shorter hospital stays, and greater postoperative range of motion (ROM) [3]. When carefully selected, patients undergoing UKA achieve excellent long-term outcomes, with reported 10- and 20-year implant survival rates between 85% and 95% [4]. Many patients with knee OA present with bilateral disease, raising important questions about surgical strategy. Options include a staged approach (operating on each knee separately with an interval between procedures) or performing both procedures during a single anesthetic session ( one-stage single-sitting bilateral UKA). A one-stage single sitting approach can reduce the need for multiple hospital admissions, shorten overall rehabilitation time, and potentially lower total healthcare costs [5]. However, concerns remain about increased intraoperative blood loss, longer operative times, and higher perioperative risks. In contrast, staging the procedures allows a recovery period between operations, possibly reducing physiological stress, but at the cost of prolonged total recovery time, higher cumulative healthcare utilization, and greater inconvenience for patients [6]. Although bilateral versus unilateral TKA has been well studied, there is relatively limited high-quality evidence specific to UKA in this context. Existing retrospective analyses have produced mixed conclusions, some indicating higher complication rates with one-stage single-sitting procedures, while others suggest comparable or even better functional results and safety. In addition, cost-effectiveness and patient-reported outcomes in this setting are not well characterised [7,8]. Given the growing use of UKA and the increasing number of patients with bilateral unicompartmental OA, it is critical to evaluate whether one-stage single-sitting bilateral UKA compromises safety or enhances clinical efficiency compared to a unilateral approach. This prospective study is designed to compare clinical outcomes, perioperative risks, and functional recovery between one-stage single-sitting bilateral and unilateral UKA. By systematically gathering and analyzing data, this study aims to support evidence-based decision-making and improve patient care in the management of unicompartmental knee OA. We hypothesised that one-stage single-sitting bilateral UKA would provide faster functional recovery and higher patient satisfaction without compromising safety compared with unilateral UKA.
.
This observational study was conducted at a high-volume tertiary orthopedic center between January 2015 and January 2019. All procedures were performed by a single senior surgeon using a standardised surgical technique and a consistent implant system (Oxford UKA). This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. As the study involved standard surgical care without deviation from routine clinical practice, formal Institutional Ethics Committee approval was not obtained. However, all patients provided written informed consent for participation and use of their anonymized clinical data for research purposes. Eligible patients included those diagnosed with isolated medial compartment OA of the knee, who were planned to undergo either one-stage single-sitting bilateral or unilateral UKA. Radiological and clinical evaluation confirmed the indication for UKA in all cases. Patients were excluded if they demonstrated lateral or tricompartmental disease on radiographs, required TKA for any reason, had a history of inflammatory arthritis, prior surgical procedures on the involved knees, or were unwilling to participate or were lost to follow-up. Group allocation into one-stage single-sitting bilateral or unilateral UKA was determined in a non-randomized, observational manner. The decision was made jointly by the patient, anesthesiologist, and surgeon, taking into account the patient’s medical status, anesthetic risk, functional expectations, and personal preference. Patients deemed to have high anesthetic risk (American Society of Anesthesiologists [ASA] classification ≥3) [9], significant comorbid conditions, or poor functional reserve were generally advised to undergo staged procedures. A sample size calculation was performed based on the Oxford Knee Score (OKS) [10], which served as the primary functional outcome measure. Assuming a minimal clinically important difference (MCID) of 4 points [11], a standard deviation of 10, a significance level (α) of 0.05, and a statistical power of 80%, the estimated required sample size was 63 patients per group. Ultimately, 256 patients were enrolled, exceeding the required sample size. Of these, 134 underwent one-stage single-sitting bilateral UKA, while 122 underwent unilateral UKA. A flow diagram depicting patient enrollment, group allocation, exclusions, and follow-up is provided in Fig. 1.
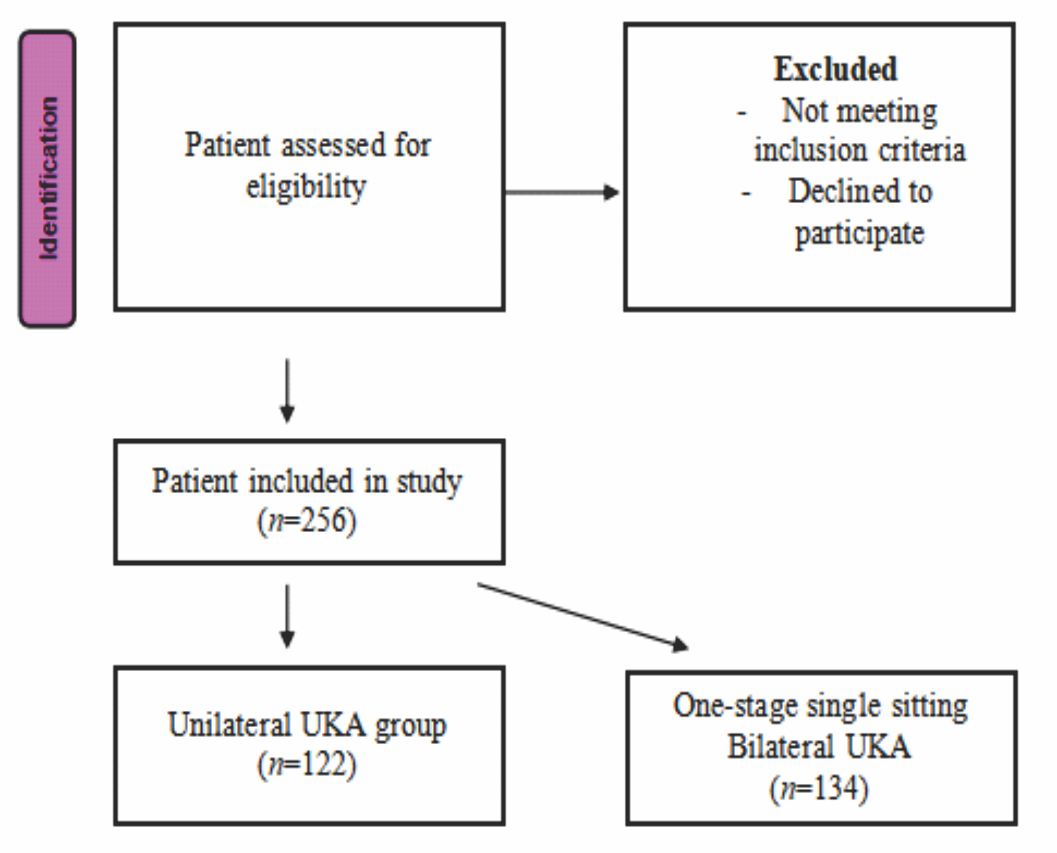
Figure 1: Patient selection flow diagram.
All included patients were radiologically confirmed to have bilateral medial compartment OA. In the unilateral UKA group, the contralateral knee was either asymptomatic or less symptomatic at baseline. These patients were managed conservatively and monitored at each follow-up visit. During the 5-year follow-up, 24 patients (19.7%) from the unilateral group subsequently underwent contralateral UKA due to progression of symptoms. These procedures were not included in the primary outcome analysis to preserve group integrity. Follow-up assessments were conducted at 2 weeks, 6 weeks, 3 months, 6 months, 1 year, and annually thereafter for up to 5 years. Outcome measures included the OKS, Visual Analog Scale (VAS) for pain [12], and annual radiographic evaluations. All clinical assessments were carried out by a trained evaluator who was blinded to the type of surgical intervention performed. Baseline data collection included pre-operative OKS and VAS scores, patient demographics, and comorbidities such as diabetes, hypertension, obesity, and cardiovascular or respiratory conditions. ASA grading was recorded preoperatively for all patients. All surgeries were performed under tourniquet control through a minimally invasive medial approach. The Oxford mobile-bearing unicompartmental knee system was used uniformly in all patients. Thromboprophylaxis included the administration of subcutaneous low-molecular-weight heparin in the immediate postoperative period, followed by oral rivaroxaban for extended prophylaxis. A standardized, structured rehabilitation protocol was implemented for all patients and supervised by a dedicated physiotherapy team. During the initial 2 weeks postoperatively, rehabilitation focused on isometric quadriceps exercises, ankle pumps, walker-assisted ambulation, and achieving knee ROM up to 90°. Between weeks 2 and 6, straight leg raises, progressive gait training, and knee flexion beyond 100° were introduced. From 6 to 12 weeks, patients began closed-chain exercises, stair climbing, and transitioned to unassisted walking. After 12 weeks, rehabilitation emphasized achieving full ROM, proprioceptive and balance training, and continuing home exercises. Importantly, there were no variations in the rehabilitation protocol between the two groups. Return to daily activities was defined as the patient’s ability to independently ambulate, perform basic household tasks, and resume low-impact activities of daily living without assistive devices. This was assessed via structured self-report at each follow-up visit.
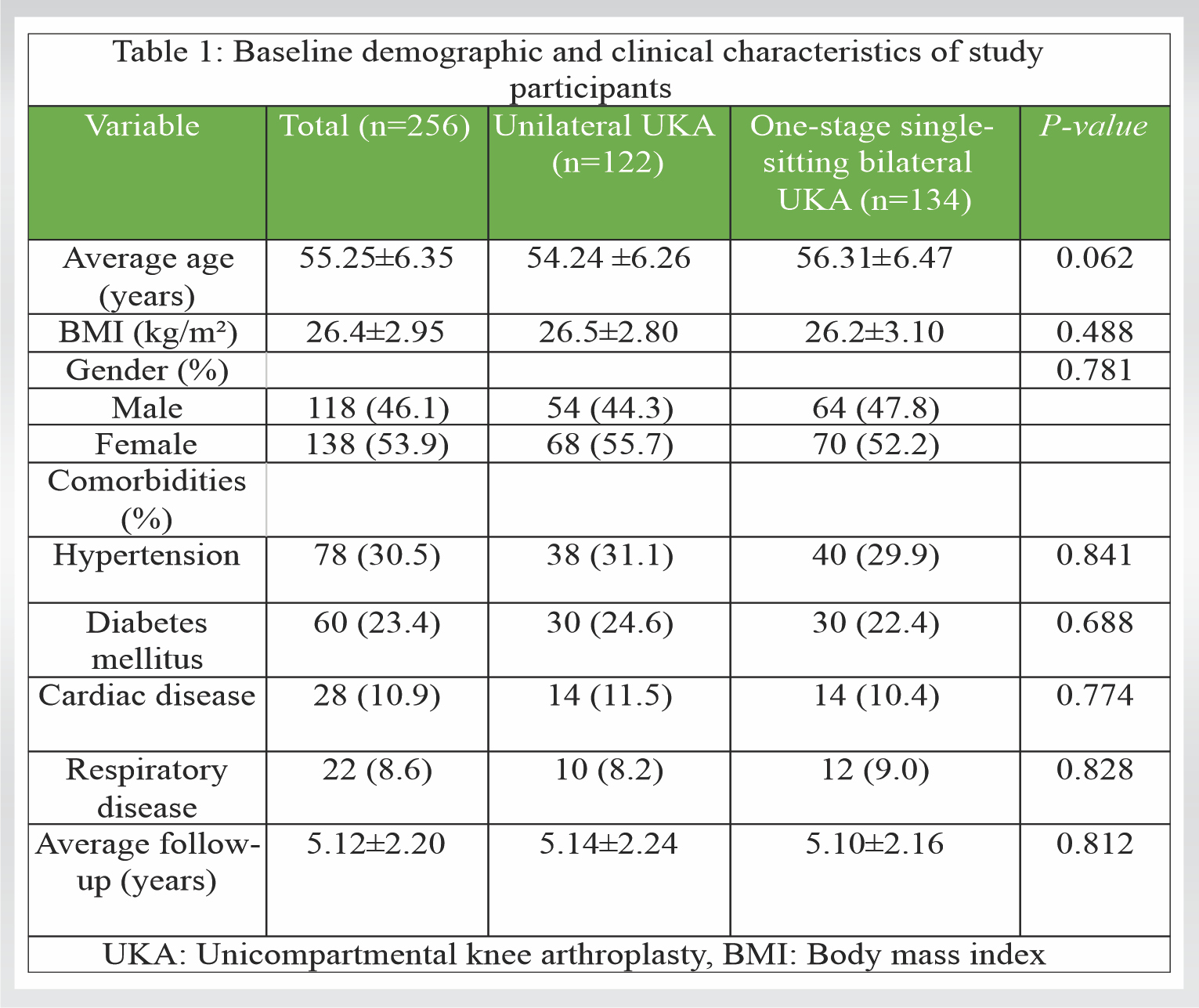
A total of 256 patients were enrolled in the study, with 122 individuals undergoing unilateral UKA and 134 receiving one-stage single-sitting bilateral UKA. Baseline characteristics such as age, gender, body mass index, and comorbidity profiles were well matched between the two cohorts (Table 1). The mean age was 54.24 ± 6.26 years in the unilateral group and 56.31 ± 6.47 years in the bilateral group, with no statistically significant difference (P = 0.062). Follow-up duration averaged 5.14 ± 2.24 years for the unilateral group and 5.10 ± 2.16 years for the bilateral group (P = 0.812) (Table 1).
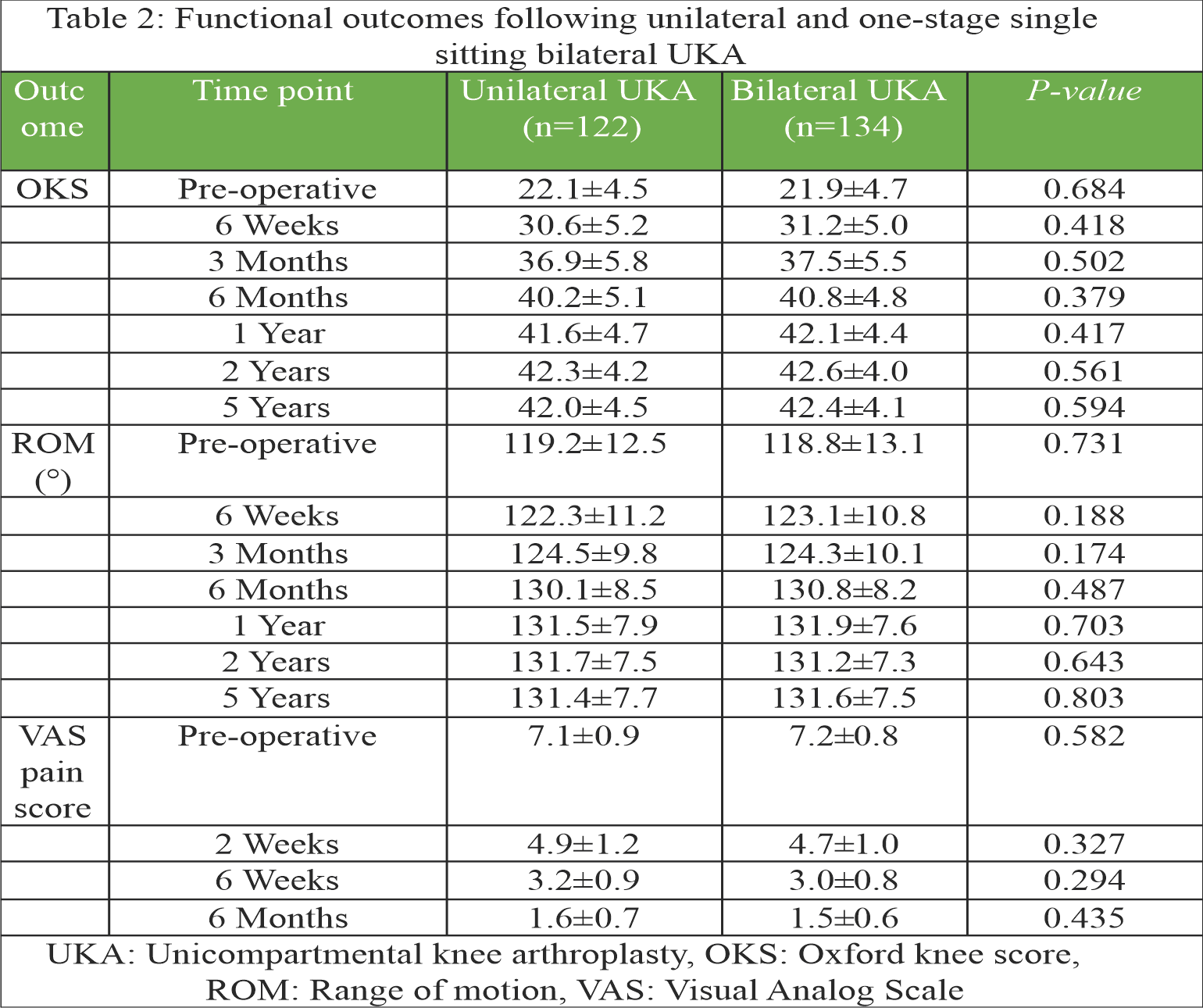
Functional outcomes, measured by the OKS and ROM, were recorded at 6 weeks, 3 months, 6 months, 1 year, 2 years, and 5 years postoperatively (Table 2).
 Both groups showed significant gains in OKS and ROM from their pre-operative values (P < 0.001), with improvements sustained throughout the follow-up period (Fig. 1 and 2). While early postoperative ROM (between 6 weeks and 3 months) showed slightly quicker gains in the bilateral group, these differences did not reach statistical significance. By 1-year, functional recovery was similar across both groups.
Both groups showed significant gains in OKS and ROM from their pre-operative values (P < 0.001), with improvements sustained throughout the follow-up period (Fig. 1 and 2). While early postoperative ROM (between 6 weeks and 3 months) showed slightly quicker gains in the bilateral group, these differences did not reach statistical significance. By 1-year, functional recovery was similar across both groups.
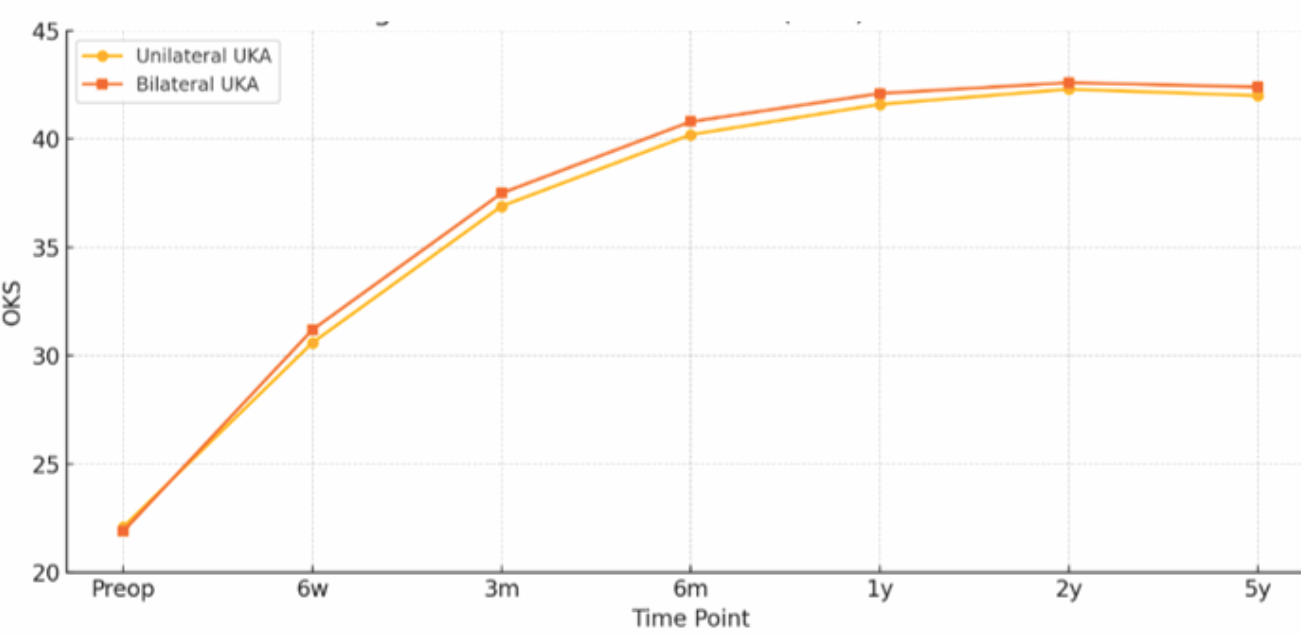
Figure 2: Line graph illustrating the mean Oxford knee scores over time for both groups.
OKS evaluations were conducted through structured interviews by trained physiotherapists, using the patient’s native language. The unilateral group demonstrated an increase in OKS from a baseline of 22.1 ± 4.5 to 41.6 ± 4.7 at 1 year and 42.0 ± 4.5 at 5 years. The bilateral group exhibited similar improvements, with scores rising from 21.9 ± 4.7 to 42.1 ± 4.4 at 1 year and 42.4 ± 4.1 at 5 years. A sub-analysis of specific OKS domains showed that at 1 year, patients in the bilateral group reported better outcomes in aspects such as limping, kneeling, and functional tasks at home. However, by the 5-year mark, these domain scores were comparable between the two groups. Initial ROM was nearly identical between groups ( 119.2 ± 12.5° in the unilateral group vs. 118.8 ± 13.1° in the bilateral group). At 5 years, both groups reached similar final ROM ( 131.4 ± 7.7° vs. 131.6 ± 7.5°, P = 0.803), indicating no significant long-term difference in mobility. Pain levels, managed using a uniform multimodal analgesia protocol, showed a mild trend toward lower VAS scores in the bilateral group at early time points. At 2 weeks post-op, mean VAS scores were 4.9 ± 1.2 in the unilateral group and 4.7 ± 1.0 in the bilateral group (P = 0.327), and at 6 weeks, 3.2 ± 0.9 vs. 3.0 ± 0.8 (P = 0.294), respectively. By 6 months, both groups reported similar pain levels (1.6 ± 0.6 vs. 1.5 ± 0.6; P = 0.435) (Table 2). No instances of mechanical failure or implant loosening were detected in either cohort during the 5-year follow-up. Length of hospital stay was similar, averaging 2.8 ± 0.9 days for unilateral UKA and 2.7 ± 1.0 days for bilateral UKA (P = 0.412). Interestingly, the bilateral group achieved rehabilitation goals with fewer physiotherapy sessions (17.6 ± 2.9 vs. 21.4 ± 3.2; P < 0.001), indicating a more efficient recovery process (Table 3).
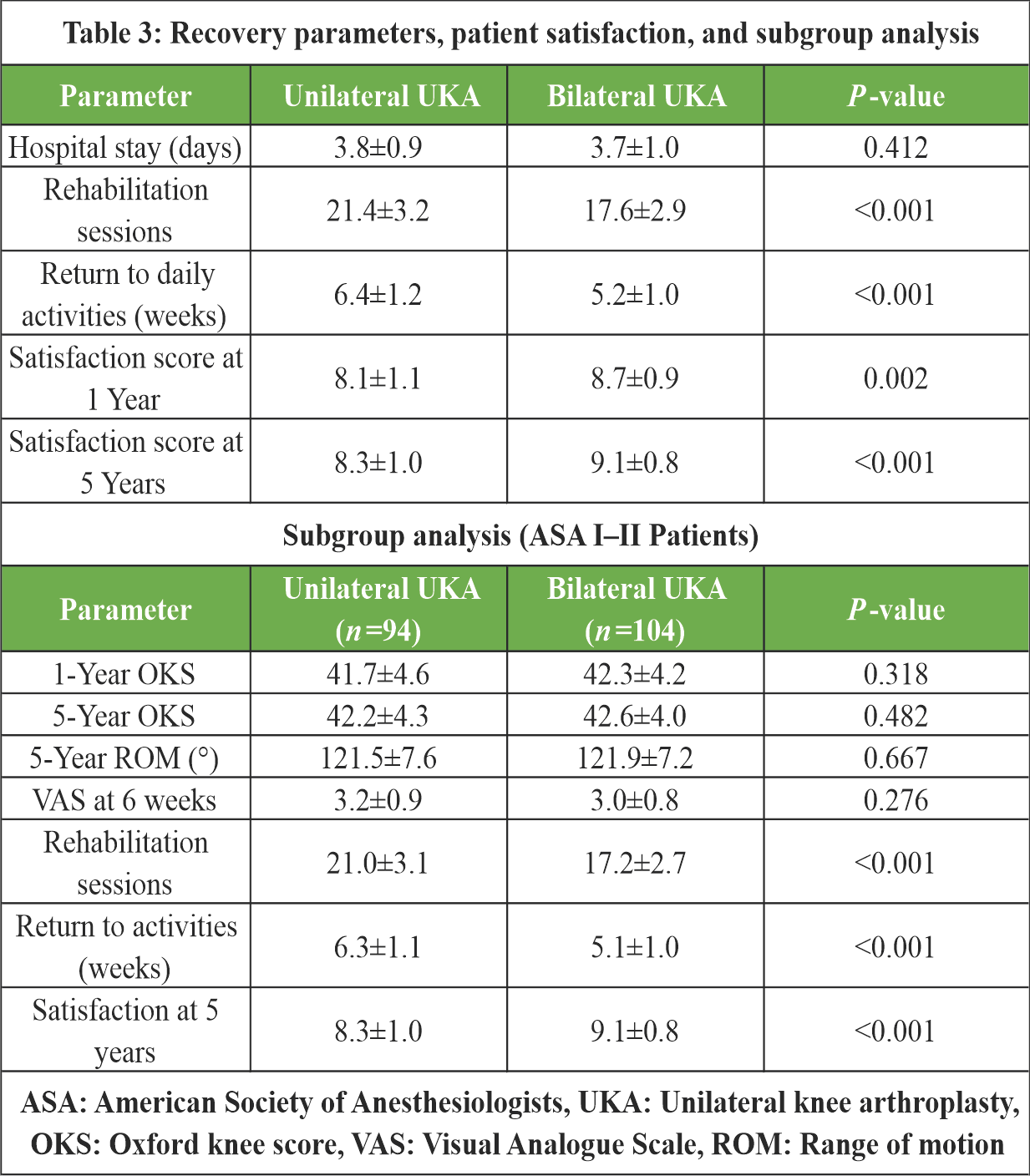 At 5 years, patient satisfaction scores were significantly higher in those who underwent bilateral procedures (9.1 ± 0.8) compared to the unilateral group (8.3 ± 1.0; P < 0.001). In addition, return to pre-operative activity levels occurred earlier in the bilateral group (5.2 ± 1.0 weeks vs. 6.4 ± 1.2 weeks; P < 0.001) (Table 3). A subgroup of 198 patients (104 in the bilateral group and 94 in the unilateral group) was classified as ASA Grade I or II. Within this lower-risk cohort, functional outcomes, pain scores, and satisfaction levels remained consistent with the overall trends observed. The bilateral group continued to demonstrate slightly earlier gains in ROM and return to daily activities and reported higher satisfaction at 5 years (P < 0.05). No significant differences in complication rates or hospital stay were observed (Table 3).
At 5 years, patient satisfaction scores were significantly higher in those who underwent bilateral procedures (9.1 ± 0.8) compared to the unilateral group (8.3 ± 1.0; P < 0.001). In addition, return to pre-operative activity levels occurred earlier in the bilateral group (5.2 ± 1.0 weeks vs. 6.4 ± 1.2 weeks; P < 0.001) (Table 3). A subgroup of 198 patients (104 in the bilateral group and 94 in the unilateral group) was classified as ASA Grade I or II. Within this lower-risk cohort, functional outcomes, pain scores, and satisfaction levels remained consistent with the overall trends observed. The bilateral group continued to demonstrate slightly earlier gains in ROM and return to daily activities and reported higher satisfaction at 5 years (P < 0.05). No significant differences in complication rates or hospital stay were observed (Table 3).
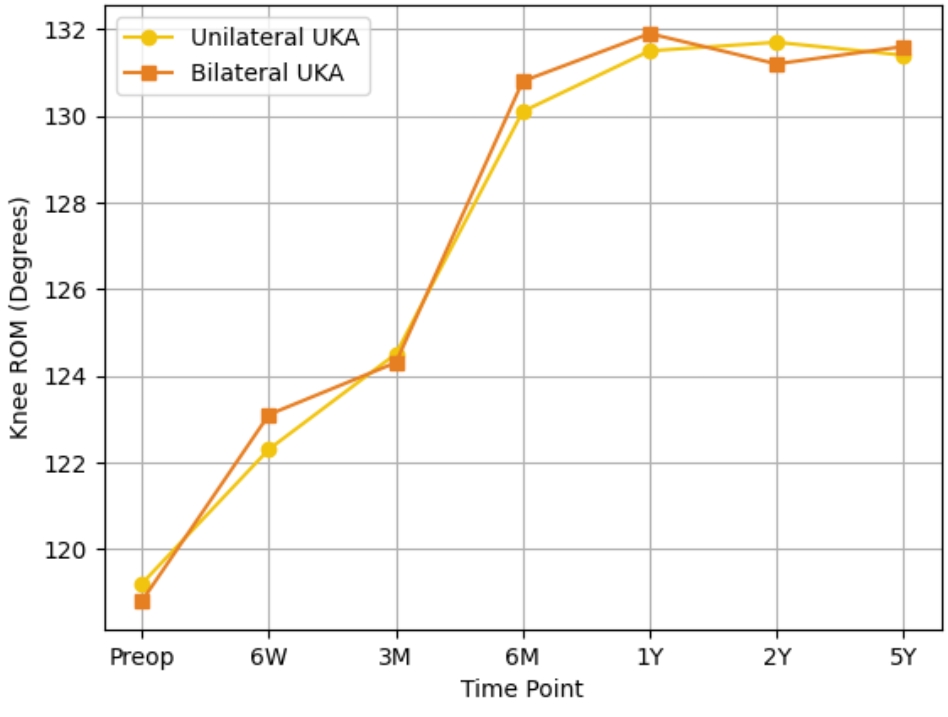
Figure 3: Line graph showing improvement in average knee range of motion over the follow-up period for both groups.
This prospective cohort study evaluated the clinical outcomes, pain relief, functional recovery, and patient satisfaction associated with one-stage single-sitting bilateral versus unilateral UKA in patients with medial compartment OA. Our findings indicate that both approaches result in significant improvements in knee function, pain reduction, and ROM. However, one-stage single-sitting bilateral UKA conferred specific advantages, including faster rehabilitation, earlier return to daily activities, and greater patient satisfaction at both short- and long-term follow-up. For working-age patients and those with bilateral symptoms, avoiding a second hospitalisation and rehabilitation cycle has substantial socioeconomic implications, particularly in low- and middle-income settings. The presence of contralateral disease in the unilateral group was acknowledged. Approximately 20% of these patients later underwent second-side UKA, reflecting the progressive nature of bilateral OA. The relatively young mean age ( 54.8 years) of our cohort may be attributed to the regional referral pattern, wherein younger patients with early-onset degenerative medial OA are actively considered for joint-preserving surgery such as UKA. Furthermore, high levels of physical activity and earlier onset of OA in the Indian population may contribute to a younger surgical demographic, as previously observed in regional arthroplasty registries [13]. The near-equal gender distribution observed (male: female ratio ≈1.2:1) differs from the typically female-predominant patterns in Western OA literature. This may reflect differing occupational and lifestyle factors in our population, where males with high-impact manual labor roles develop earlier medial compartment degeneration. However, since both groups were well matched, this does not impact intergroup comparisons. Functional outcomes, as measured by the OKS, improved markedly in both groups compared to pre-operative baselines, with no statistically significant differences observed between cohorts at any follow-up interval. These results are consistent with existing literature affirming the efficacy of UKA in preserving joint kinematics and restoring function in patients with isolated Unicompartmental disease [14,15]. Similarly, recovery of ROM was comparable between groups, with both achieving flexion beyond 120° by 6 months, underscoring the benefits of the minimally invasive approach inherent to UKA. A key finding was that patients undergoing one-stage single-sitting bilateral UKA required significantly fewer physiotherapy sessions to achieve functional milestones. This likely reflects the efficiency of a single recovery phase, which not only reduces rehabilitation demands but may also enhance overall cost-effectiveness. In addition, return to daily activities occurred significantly earlier in the bilateral group, both at 1 and 5 years, which is particularly valuable in active or working-age populations seeking to minimize downtime. Pain control, assessed using the VAS, improved significantly in both groups. Although patients in the bilateral group reported slightly lower VAS scores throughout follow-up, these differences were not statistically significant. Nonetheless, the consistent reduction in pain across both groups affirms the analgesic benefit of UKA when performed under a standardized multimodal pain management protocol. Contrary to expectations based on TKA literature [3,4,5], early post-operative VAS scores were slightly lower in the bilateral UKA group. We hypothesize that this may reflect a psychological benefit of having both symptomatic joints addressed in a single procedure, avoiding the discomfort of an untreated contralateral knee. In addition, the uniform use of minimally invasive techniques and multimodal analgesia may have blunted typical early pain differences. Several early differences between groups in VAS and ROM did not reach statistical significance but may still be clinically relevant. For instance, the MCID for VAS in knee arthroplasty patients is approximately 1.0 point, and for knee ROM, a 5° to 10° change is often considered functionally meaningful [16,17]. In our study, trends in these domains favoring the bilateral group approached or exceeded these thresholds at early follow-up intervals, suggesting potential real-world benefits. Interestingly, the length of hospital stay did not differ significantly between the two groups, challenging the assumption that one-stage single-sitting bilateral procedures necessitate prolonged inpatient care. This supports the safety and feasibility of one-stage single-sitting bilateral UKA when performed in appropriately selected patients and under enhanced recovery protocols. Patient satisfaction was notably higher in the bilateral group at both 1 and 5 years. This may reflect the psychological and functional advantage of resolving bilateral symptoms in a single surgical episode, as well as the avoidance of a second procedure. These findings are in line with prior reports suggesting superior patient-reported outcomes and quality of life following one-stage single-sitting bilateral interventions [18,19,20]. Although the greatest divergence in outcomes was seen during the early post-operative period, a 5-year follow-up was intentionally included to assess the durability of functional recovery, patient satisfaction, and implant survival. It also allowed tracking secondary interventions and contralateral procedures in the unilateral group, providing a comprehensive view of disease progression and treatment sustainability. This study has several notable strengths, including its prospective design, sufficient sample size, consistent surgical approach, and a standardized postoperative rehabilitation protocol. High follow-up rates and the use of independent, blinded assessors for outcome evaluation further enhance the study’s validity by minimizing the risk of observer bias. However, all procedures were performed by a single high-volume surgeon in a tertiary referral center, which may limit the generalizability of our results to lower-volume or community-based settings. Nonetheless, certain limitations must be acknowledged. The lack of randomization in assigning patients to treatment groups may have introduced selection bias, as individuals with higher perioperative risk were more likely to undergo unilateral UKA. To address the potential selection bias introduced by non-random group allocation, a subgroup analysis was performed among ASA I–II patients. Results remained consistent with the overall cohort, lending support to the internal validity of our conclusions. We acknowledge that potential confounders such as socioeconomic status, occupational demands, and baseline physical activity were not formally captured. However, our study population was relatively homogeneous in terms of urban setting, access to care, and functional expectations, which may have minimized the variability introduced by these factors. Another limitation of our outcome assessment is the use of the OKS, which is a patient-reported outcome measure reflecting bilateral knee function. While validated and widely used, it lacks knee-specific resolution. However, to ensure consistency and facilitate comparison with existing literature, we selected OKS. Future studies could incorporate joint-specific tools such as the KOOS or WOMAC with side-specific scoring in bilateral procedures. Future randomized controlled studies are warranted to confirm and expand on these results.
One-stage single-sitting bilateral UKA is a safe and effective surgical option for patients with medial compartment OA. In this prospective study, both one-stage single-sitting bilateral and unilateral UKA demonstrated significant improvements in pain relief, ROM, and functional outcomes. However, patients undergoing one-stage single-sitting bilateral UKA experienced earlier return to daily activities, required fewer rehabilitation sessions, and reported higher satisfaction at both short- and long-term follow-up. Importantly, these benefits were achieved without increasing hospital stay or perioperative complications. When performed in carefully selected patients, one-stage single-sitting bilateral UKA offers meaningful functional and logistical advantages without compromising safety.
For carefully selected patients (particularly ASA I–II) with bilateral medial compartment disease, one-stage single-sitting bilateral UKA is a safe and efficient surgical option that can reduce overall rehabilitation burden and accelerate functional recovery without compromising outcomes at 5 years.
References
- 1. Rajani AM, Mittal AR, Shah UA, Kulkarni VU, Dubey R. Midterm functional outcomes and survivorship of Oxford cemented medial unicompartmental knee arthroplasty: A comprehensive analysis of the Indian scenario. J Clin Orthop Trauma 2025;68:103115. [Google Scholar] [PubMed]
- 2. Mittal A, Meshram P, Kim WH, Kim TK. Unicompartmental knee arthroplasty, an enigma, and the ten enigmas of medial UKA. J Orthop Traumatol 2020;21:15. [Google Scholar] [PubMed]
- 3. Tille E, Beyer F, Auerbach K, Tinius M, Lützner J. Better short-term function after unicompartmental compared to total knee arthroplasty. BMC Musculoskelet Disord 2021;22:326. [Google Scholar] [PubMed]
- 4. Paul RW, Osman A, Clements A, Tjoumakaris FP, Lonner JH, Freedman KB. What are the all-cause survivorship rates and functional outcomes in patients younger than 55 years undergoing primary knee arthroplasty? A systematic review. Clin Orthop Relat Res 2022;480:507-22. [Google Scholar] [PubMed]
- 5. Crawford DA, Berend KR, Thienpont E. Unicompartmental knee arthroplasty: US and global perspectives. Orthop Clin North Am 2020;51:147-59. [Google Scholar] [PubMed]
- 6. Desouza C, Shetty V. Recovery after total knee arthroplasty: Does one or two knees matter? J Clin Orthop Trauma 2025;68:103076. [Google Scholar] [PubMed]
- 7. Holzer LA, Holzer G. The most influential papers in unicompartmental knee arthroplasty. Knee Surg Relat Res 2020;32:54. [Google Scholar] [PubMed]
- 8. Liddle AD, Pandit H, Judge A, Murray DW. Optimal usage of unicompartmental knee arthroplasty: A study of 41,986 cases from the national joint registry for England and Wales. Bone Joint J 2015;97-B:1506-11. [Google Scholar] [PubMed]
- 9. Daabiss M. American Society of Anaesthesiologists physical status classification. Indian J Anaesth 2011;55:111-5. [Google Scholar] [PubMed]
- 10. Clement ND, Afzal I, Liu P, Phoon KM, Asopa V, Sochart DH, et al. The Oxford knee score is a reliable predictor of patients in a health state worse than death and awaiting total knee arthroplasty. Arthroplasty 2022;4:33. [Google Scholar] [PubMed]
- 11. Clement ND, Haddad FS. Are the current minimal clinically important differences fit for purpose? Bone Joint J 2024;106-B:1033-5. [Google Scholar] [PubMed]
- 12. Langley GB, Sheppeard H. The visual analogue scale: Its use in pain measurement. Rheumatol Int 1985;5145-8. [Google Scholar] [PubMed]
- 13. Travers HI, Nin DZ, Kuznetsov M, Chang DC, Talmo CT, Smith EL. National trends in total and unicompartmental knee arthroplasty: 2020 to 2022. J Clin Orthop Trauma 2025;67:103064. [Google Scholar] [PubMed]
- 14. Casper DS, Fleischman AN, Papas PV, Grossman J, Scuderi GR, Lonner JH. Unicompartmental knee arthroplasty provides significantly greater improvement in function than total knee arthroplasty despite equivalent satisfaction for isolated medial compartment osteoarthritis. J Arthroplasty 2019;34:1611-6. [Google Scholar] [PubMed]
- 15. Campi S, Tibrewal S, Cuthbert R, Tibrewal SB. Unicompartmental knee replacement – current perspectives. J Clin Orthop Trauma 2018;9:17-23. [Google Scholar] [PubMed]
- 16. Clement ND, MacDonald D, Simpson AH. The minimal clinically important difference in the Oxford knee score and short Form 12 score after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 2014;22:1933-9. Erratum in: Knee Surg Sports Traumatol Arthrosc 2016;24:3696. [Google Scholar] [PubMed]
- 17. Tubach F, Ravaud P, Beaton D, Boers M, Bombardier C, Felson DT, et al. Minimal clinically important improvement and patient acceptable symptom state for subjective outcome measures in rheumatic disorders. J Rheumatol 2007;34:1188-93. [Google Scholar] [PubMed]
- 18. Ahn JH, Kang DM, Choi KJ. Bilateral simultaneous unicompartmental knee arthroplasty versus unilateral total knee arthroplasty: A comparison of the amount of blood loss and transfusion, perioperative complications, hospital stay, and functional recovery. Orthop Traumatol Surg Res 2017;103:1041-5. [Google Scholar] [PubMed]
- 19. Desouza C, Shetty V. Beyond one step: Unveiling optimal approach for bilateral knee arthroplasty – a comprehensive meta-analysis. Arch Orthop Trauma Surg 2024;144:3631-9. [Google Scholar] [PubMed]
- 20. Nagata N, Hiranaka T, Okamoto K, Fujishiro T, Tanaka T, Kensuke A, et al. Is simultaneous bilateral unicompartmental knee arthroplasty and total knee arthroplasty better than simultaneous bilateral total knee arthroplasty? Knee Surg Relat Res 2023;35:12. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes
July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes June 1, 2026 Prospective Evaluation of Clavicle Fracture Osteosynthesis: Patient Satisfaction, Clinical, and Radiological Outcomes with Clavipectoral Fascial Plane Block
June 1, 2026 Prospective Evaluation of Clavicle Fracture Osteosynthesis: Patient Satisfaction, Clinical, and Radiological Outcomes with Clavipectoral Fascial Plane Block June 1, 2026 Survivorship and Functional Outcomes after Surgery for Metastatic Spinal Disease Including Cord Compression: Single-Surgeon Cohort Series from UK Tertiary Center
June 1, 2026 Survivorship and Functional Outcomes after Surgery for Metastatic Spinal Disease Including Cord Compression: Single-Surgeon Cohort Series from UK Tertiary Center June 1, 2026 Comparative Analysis of Functional Outcomes in Robotic-assisted versus Conventional Total Knee Arthroplasty
June 1, 2026 Comparative Analysis of Functional Outcomes in Robotic-assisted versus Conventional Total Knee Arthroplasty