
Posterior sternoclavicular joint dislocations in skeletally immature patients may remodel over time, allowing safe conservative management in carefully selected cases.
Dr. Abdalla O. Abdalla, Department of Trauma and Orthopaedics, Cork University Hospital, Cork, Ireland. E-mail: abdalla_almansoury@hotmail.com
Abstract
Introduction: Posterior sternoclavicular joint (SCJ) dislocations are rare but potentially life-threatening injuries due to their proximity to vital mediastinal structures. Management traditionally favors urgent reduction with surgical stabilization indicated when persistent instability poses ongoing risk to mediastinal structures.
Case Report: We present a case of a 13-year-old male with a posterior SCJ dislocation who demonstrated significant spontaneous remodeling over 6 years following conservative management. This case highlights the remodeling potential of the skeletally immature SCJ and supports non-operative treatment in select patients without mediastinal compromise.
Conclusion: Awareness of this natural history may help guide management decisions and improve informed consent discussions.
Keywords: Sternoclavicular joint, posterior dislocation, physeal injury, remodeling, conservative management, clavicle.
Posterior sternoclavicular joint (SCJ) dislocations are rare injuries but carry significant clinical importance because of the joint’s close proximity to vital mediastinal structures, including the trachea, esophagus, and major vascular pathways [1,2]. Even minor posterior displacement can endanger these structures, making timely recognition and appropriate management essential. The SCJ is a saddle-type synovial articulation supported by a fibrocartilaginous disc and strong ligamentous complexes, which contribute to its inherent stability and influence the pattern of injury following trauma [3,4]. Diagnosis of posterior SCJ injuries can be challenging. Clinical signs may be subtle, and conventional radiographs often fail to provide adequate visualization due to overlapping anatomical structures [2,5]. Computed tomography (CT) is therefore considered the most reliable imaging modality for confirming posterior displacement and assessing mediastinal involvement [5]. However, CT has limitations in detecting physeal injuries, which are common in adolescents because the medial clavicular physis remains open until early adulthood [6]. As a result, many posterior SCJ injuries in younger patients represent physeal fracture-dislocations rather than true joint dislocations, a distinction that has important implications for management and prognosis [6,7]. Management strategies vary depending on the acuity and severity of presentation. Urgent reduction is recommended when there is evidence of neurovascular compromise, while surgical stabilisation may be required for unstable or irreducible injuries [8,9,10]. Despite this, emerging evidence suggests that conservative management may be appropriate in carefully selected cases, particularly in skeletally immature patients who possess substantial remodeling potential [7,11,12]. Adaptive changes in bone and soft tissues can restore functional stability over time, and long-term outcomes following non-operative treatment may be comparable to those achieved with surgical intervention in selected cohorts [8,13]. There remains limited literature describing the natural history of posterior SCJ injuries managed conservatively, especially regarding long-term remodeling in adolescents. Understanding this process is important for guiding treatment decisions, counseling families and determining appropriate follow-up. This case report describes a posterior SCJ dislocation in a skeletally immature patient with notable remodeling observed over several years, contributing to the growing evidence that non-operative management may be a safe and effective option in selected presentations.
A 13-year-old right-hand-dominant male presented to the Emergency Department in June 2014 with a right shoulder injury sustained while playing football. The injury had occurred 2 weeks earlier following a direct impact to the right clavicle during a collision. He reported immediate pain and swelling over the anterior chest and difficulty mobilizing the shoulder due to discomfort. He denied paraesthesia, weakness, dyspnea, dysphagia or dysphonia. On examination, there was localized swelling and tenderness over the right SCJ without bruising. Shoulder range of motion was preserved, and neurovascular assessment demonstrated intact axillary, median, radial and ulnar nerve function. A CT scan (Fig. 1) confirmed a posterior dislocation of the right SCJ with an associated anterior mediastinal hematoma.
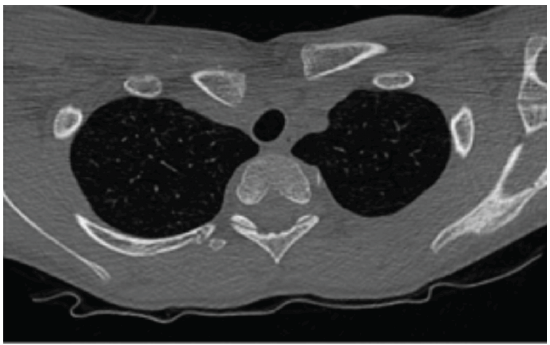
Figure 1: Computed tomography (CT) scan – Upper thorax with right sternoclavicular joint dislocation. Axial CT image showing posterior displacement of the right sternoclavicular joint. The medial end of the right clavicle is displaced posteriorly relative to the sternum, with potential compression of adjacent mediastinal structures.
With parental consent, the patient underwent closed reduction under cardiothoracic supervision. He was positioned supine with a sandbag between the scapulae. Longitudinal traction was applied to the right upper limb with counter-traction while the limb was held in abduction and slight extension. The medial clavicle was manually levered anteriorly using a pointed reduction clamp. A figure-of-eight bandage and sling were applied following reduction. A repeat CT scan (Fig. 2) the next day demonstrated minimal improvement compared with the initial imaging. As the patient remained asymptomatic and hemodynamically stable, a multidisciplinary team recommended conservative management. He commenced physiotherapy and was discharged shortly thereafter.
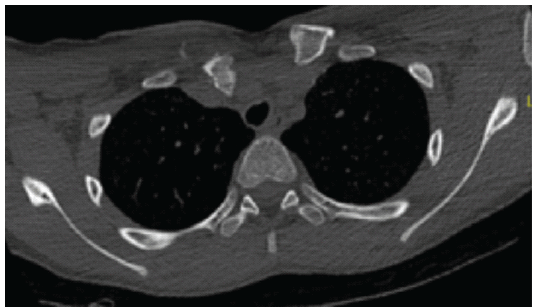
Figure 2: Computed tomography (CT) scan – Thoracic apex with sternoclavicular joint (SCJ) Pathology (post-closed attempted reduction). Axial CT slice demonstrating posterior dislocation of the right SCJ. The trachea appears slightly deviated, possibly due to mass effect from the displaced clavicle.
At 6-week follow-up, the patient had regained full shoulder range of motion with no pain or functional limitation. He was discharged from orthopedic care with ongoing physiotherapy and safety-netting advice.
Approximately 6 years later, in mid-2020, the patient re-presented to the Emergency Department after sustaining a new injury to the right SCJ while playing Gaelic football. The injury had occurred 2 weeks earlier. Examination revealed localized tenderness and a subtle prominence over the joint, with minimal swelling and no bruising. Shoulder motion remained full, and neurovascular status was intact. There were no signs of respiratory compromise or swallowing difficulty.
Initial radiographs (Fig. 3) were inconclusive, prompting further evaluation with CT (Fig. 4). Imaging demonstrated evidence of previous medial clavicle injury with remodeling and mild malalignment. No acute posterior dislocation was identified. A 2-mm discrepancy between the right and left SCJs was noted.
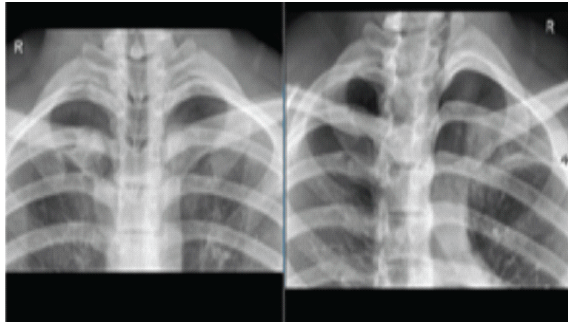
Figure 3: Chest X-rays – Right sternoclavicular joint dislocation from the most recent presentation to A&E. Comparative radiographs showing asymmetry of the sternoclavicular joints. The right clavicle appears displaced posteriorly, with altered alignment at the manubria junction. The “R” marker confirms laterality.
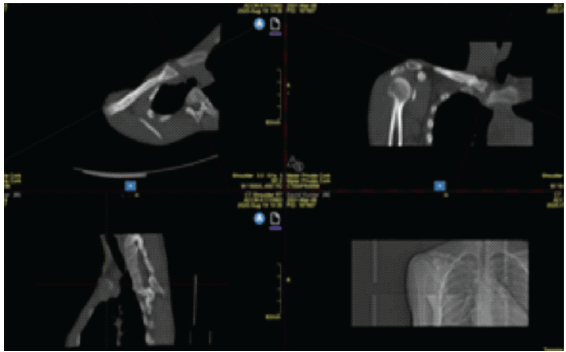
Figure 4: Multiplanar imaging – Right sternoclavicular joint remodeling. Composite imaging reveals structural changes consistent with remodeling of the right sternoclavicular joint. The sagittal and coronal views show altered bone contours and joint morphology, possibly following prior posterior dislocation. Evidence of cortical thickening, irregular joint surfaces, and adaptation of surrounding soft-tissues suggest chronic changes rather than acute trauma.
The patient was reviewed by an upper limb orthopedic surgeon and found to have satisfactory joint remodeling with preserved function. As he remained asymptomatic and had returned to full sporting and occupational activities, he was discharged from orthopedic follow‑up with advice to continue physiotherapy.
Posterior SCJ dislocations are rare but clinically important injuries due to the joint’s proximity to vital mediastinal structures, where even minor displacement can place the trachea, esophagus, or major vessels at risk [1,2]. The stability of the SCJ is maintained by strong ligamentous support, including the costoclavicular, interclavicular, and posterior SCJ ligaments, which resist excessive translational forces [3,4]. In adolescents, the medial clavicular physis remains open until early adulthood, making physeal fracture-dislocations more common than true SCJ dislocations [6]. This distinction is clinically relevant because physeal injuries possess greater remodeling potential, particularly in skeletally immature patients [6,7]. The remodeling capacity observed in this case aligns with previous reports demonstrating that adaptive changes in bone and soft tissues can restore functional stability over time without surgical intervention [7,11,12]. The patient’s long-term outcome, including full return to sport and work, supports the concept that conservative management may be effective in selected cases, especially when the injury involves the physis rather than the true joint articulation. Diagnosis of posterior SCJ injuries remains challenging. Conventional radiographs often fail to visualize the joint adequately due to overlapping anatomical structures [2,5]. CT is considered the most reliable modality for confirming posterior displacement and assessing mediastinal involvement [5]. However, CT is limited in detecting physeal injuries because cartilaginous structures are poorly visualized. In this case, the initial CT confirmed posterior displacement, while later imaging demonstrated remodeling with mild malalignment. The absence of symptoms and preserved function suggests that the remodeling process contributed to long-term stability. Although magnetic resonance imaging and ultrasound may improve detection of physeal injuries, their routine use in SCJ trauma is not yet established [6]. Management strategies depend on the acuity and severity of presentation. Acute posterior SCJ dislocations with neurovascular compromise require urgent reduction, and surgical stabilisation may be necessary when reduction is unsuccessful or instability persists [8,9,14]. However, surgery carries inherent risks due to the proximity of mediastinal structures, including potential vascular injury, implant failure, and post-operative stiffness [3,14]. Late presentations pose additional challenges, as callus formation around mediastinal structures increases the risk of morbidity and complicates attempts at anatomical reduction [8]. These considerations highlight the importance of balancing surgical risks against the remodeling potential in younger patients. Emerging evidence suggests that conservative management can yield favorable outcomes when patients do not exhibit persistent instability, recurrent dislocation, or mediastinal symptoms [8,13]. The functional recovery observed in this case mirrors outcomes reported in selected cohorts where non-operative treatment achieved results comparable to surgical stabilisation [8]. This reinforces the importance of careful patient selection, close monitoring, and multidisciplinary decision-making when considering conservative management. Further research is needed to clarify the indications for non-operative versus surgical management, particularly in skeletally immature patients. Improved imaging strategies may also help differentiate true dislocations from physeal injuries, supporting more accurate diagnosis, treatment planning, and patient counseling.
This case demonstrates that posterior SCJ dislocations in skeletally immature patients may achieve functional stability through a natural remodeling process, particularly when the injury involves the medial clavicular physis. Although surgical reduction and stabilisation can provide more predictable anatomical correction, these procedures carry inherent risks due to the proximity of vital mediastinal structures. Understanding the natural history and remodeling potential of these injuries is therefore essential when counseling patients and families about the relative benefits and risks of operative and non-operative approaches. This is especially relevant in late or sub-acute presentations, where the balance between surgical risk and the likelihood of spontaneous adaptation becomes a key factor in decision-making.
Posterior SCJ dislocations in adolescents may remodel over time, allowing safe conservative management when the patient is asymptomatic and mediastinal structures are not compromised.
References
- 1. Wirth MA. Sternoclavicular joint injuries. J Am Acad Orthop Surg 2002;10:277-85. [Google Scholar] [PubMed]
- 2. Ponce BA, Kundukulam JA, Pflugner R, Robichaux JM, Momaya AM. Sternoclavicular joint injuries and mediastinal involvement: Diagnostic and management strategies. J Am Acad Orthop Surg 2013;21:467–75. [Google Scholar] [PubMed]
- 3. Rockwood CA Jr., Wirth MA. Disorders of the sternoclavicular joint. In: Rockwood CA Jr., Matsen FA 3rd, editors. The Shoulder. Philadelphia, PA: Saunders; 2004. p. 527-63. [Google Scholar] [PubMed]
- 4. Spencer EE Jr., Kuhn JE. Biomechanical analysis of reconstructions for sternoclavicular joint instability. J Bone Joint Surg Am 2004;86:98-105. [Google Scholar] [PubMed]
- 5. Lee JT, Nasreddine AY, Black EM, Day CS, Kramer JF, Higgins LD. Computed tomography evaluation of sternoclavicular joint injuries. J Bone Joint Surg Am 2014;96:e26. [Google Scholar] [PubMed]
- 6. Bae DS, Waters PM. The paediatric sternoclavicular joint: Diagnosis and management of injuries and instability in children and adolescents. J Pediatr Orthop 2006;26:692-8. [Google Scholar] [PubMed]
- 7. Hesse E, Buckup J, Smolen D, Smolen D, Smolen D, Smolen D, et al. Posterior sternoclavicular joint dislocation: Diagnosis, management, and outcomes. J Orthop Trauma 2023;37:1–8. [Google Scholar] [PubMed]
- 8. Groh GI, Wirth MA, Rockwood CA Jr. Treatment of traumatic posterior sternoclavicular dislocations. J Shoulder Elbow Surg 2011;20:107-13. [Google Scholar] [PubMed]
- 9. Tepolt FA, Carry PM, Heyn PC, Miller NH. Posterior sternoclavicular joint injuries in the adolescent population: Outcomes of surgical management in a rare cohort. J Pediatr Orthop 2014;34:369-75. [Google Scholar] [PubMed]
- 10. Laffosse JM. Sternoclavicular joint dislocation and its management. Orthop Traumatol Surg Res 2016;102:S61-9. [Google Scholar] [PubMed]
- 11. Nettles JL, Linscheid RL. Sternoclavicular dislocations: A follow-up study of twenty-seven patients. J Bone Joint Surg Am 1968;50:1077-83. [Google Scholar] [PubMed]
- 12. Kuzak N, Ishkanian A, Abu-Laban RB. Posterior sternoclavicular joint dislocation: Case report and discussion. Can J Emerg Med 2006;8:355-7. [Google Scholar] [PubMed]
- 13. Morell DJ, Thyagarajan DS. Sternoclavicular joint dislocation and its management: A review of the literature. World J Orthop 2016;7:244-50. [Google Scholar] [PubMed]
- 14. Bak K. Traumatic posterior dislocation of the sternoclavicular joint: Report of three cases and review of literature on acute management and late reconstruction techniques. Scand J Med Sci Sports 1999;9:52-6. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Prospective Evaluation of Clavicle Fracture Osteosynthesis: Patient Satisfaction, Clinical, and Radiological Outcomes with Clavipectoral Fascial Plane Block
June 1, 2026 Prospective Evaluation of Clavicle Fracture Osteosynthesis: Patient Satisfaction, Clinical, and Radiological Outcomes with Clavipectoral Fascial Plane Block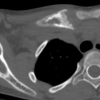 May 1, 2026 A Rare Occurrence of Chronic Recurrent Multifocal Osteomyelitis in Clavicle: Case Report
May 1, 2026 A Rare Occurrence of Chronic Recurrent Multifocal Osteomyelitis in Clavicle: Case Report February 1, 2026 Addressing Bilateral Post-traumatic Distal Radius Growth Arrest with Positive Ulnar Variance with Acute Ulnar Shortening Osteotomy and Distal Radioulnar Joint Fixation in a 13-Year-Old Child: A Case Report
February 1, 2026 Addressing Bilateral Post-traumatic Distal Radius Growth Arrest with Positive Ulnar Variance with Acute Ulnar Shortening Osteotomy and Distal Radioulnar Joint Fixation in a 13-Year-Old Child: A Case Report February 1, 2026 Atraumatic Subtrochanteric Stress Fracture in a 45-Year-Old Housewife: Diagnostic Challenge and Management Strategy
February 1, 2026 Atraumatic Subtrochanteric Stress Fracture in a 45-Year-Old Housewife: Diagnostic Challenge and Management Strategy