
Os vesalianum can be a symptomatic cause of lateral foot pain, and in refractory cases, operative management can be successfully attempted.
Dr. Vignesh Chandrasekar, Department of Orthopaedics, All India Institute of Medical Sciences, Mangalagiri, Andhra Pradesh, India. E-mail: vigneshc024@gmail.com
Abstract
Introduction: Accessory bones, such as the Os vesalianum, are developmental skeletal variations in the ankle and foot. The prevalence of Os vesalianum is between 0.1% and 1.0% of the population. It lies proximal to the fifth metatarsal base and is found within the peroneus brevis tendon.
Case Report: We present a case of a 34-year-old female with persistent pain in the lateral border of her left foot. X-rays were suggestive of Os vesalianum. Computed tomography and magnetic resonance imaging confirmed a thin line of fluid between Os vesalianum and the fifth metatarsal base. After failed conservative measures, she was managed by surgical excision of the Os vesalianum and reattaching the peroneus brevis to the fifth metatarsal base with a suture anchor. The patient resumed routine activities 8 weeks later, with no residual pain. After 3 months of follow-up, the patient’s strength was normal, and she had no pain.
Conclusion: Os vesalianum, though rare, is mostly asymptomatic and is often detected incidentally. In symptomatic cases, it can cause chronic lateral foot pain. It is important to differentiate Os vesalianum from other causes of chronic lateral foot pain, such as a Jones fracture or avulsion fracture. Surgical excision with peroneus tendon repair is the standard treatment, giving favorable outcomes in symptomatic cases that do not respond to conservative measures.
Keywords: Os vesalianum pedis, accessory bone, peroneus brevis tendonitis, fifth metatarsal, lateral foot pain.
Accessory bones of the ankle and foot are developmental skeletal variations. O’Rahilly’s[1] definition of accessory bones states that they have to be “inconsistent, independent, well-defined bones in an otherwise normally developed foot.” They are rarely symptomatic. Coskun et al. reported the incidence of the most common accessory bones in adult feet. These were: accessory navicular (11.7%), Os peroneum (4.7%), Os trigonum (2.3%), Os supranaviculare (1.6%), Os vesalianum (0.4%), Os supratalare (0.2%), and Os intermetatarseum (0.2%) [2]. Bilateral accessory bones were seen in 7.6% of cases. The distribution of male and female patients was similar [3].
An accessory bone situated proximal to the fifth metatarsal bone is known as the Os vesalianum pedis (OVP), and it is extremely rare. It is named after Andreas Vesalius, anatomist and physician, who first described it in “de humani corporis fabrica” in 1543. Later on, this accessory ossicle was named “Os vesalianum pedis” by Pfitzner in memory of Andreas Vesalius [4]. Its prevalence has been reported to be between 0.1% and 1.0% of the population. A radiological study on prevalence by Pitchandi et al. showed only 15 cases of OVP among 1000 X-ray studies, all of which were unilateral [5]. Bilateral OVP is even rarer and reported in some familial cases. If present, it is found within the peroneus brevis tendon. It is located just proximal to the tip of a well-developed fifth metatarsal tuberosity.
OVP, like other accessory ossicles in the foot, is typically asymptomatic and is discovered by chance on regular radiography or following an acute foot or ankle injury. In some instances, the opposing surfaces at the accessory bone (synchondrosis) may be sclerotic due to chronic degenerative changes, suggesting a pseudoarthrosis, and become symptomatic. Of the few reported symptomatic cases, OVP is the cause of chronic lateral foot pain [6]. It is important to clinically examine and radiologically define and differentiate OVP from other causes of lateral foot pain, such as Jones fracture, avulsion fracture of the proximal fifth metatarsal/Iselin’s disease [7].
There have only been very few reports of symptomatic OVP so far, and some of them were managed conservatively. Very few cases managed by surgical resection or osteosynthesis have been reported so far. We also present here a case of chronic symptomatic OVP in a young female patient, which was managed by surgical excision of the OVP and repair of the peroneus brevis tendon with a suture anchor. We presented a review of all similar cases reported in the literature. We discuss the cause of pain in OVP and different methods of management in symptomatic cases. The exact etiopathogenesis of OVP remains unclear and is thought to be related to failure of apophyseal fusion or post-traumatic pseudoarthrosis.
History
A 34-year-old female reported having pain in her left foot that was concentrated on the lateral side of the foot and worsened while climbing downstairs and during exertional foot activities. The symptoms had worsened over the course of the preceding year, and there was no history of trauma. The foot arches were well-maintained. Clinical tenderness was localized to the fifth metatarsal base, and pain increased when walking along the lateral border of the foot. Her Visual Analog Scale (VAS) score was 8/10. Non-steroidal anti-inflammatory medications, activity modification, and supervised physiotherapy with stretching exercises were given for 1 year, with persistent pain during walking and no significant improvement. Plantar flexion and resisted inversion also caused pain pointing to the fifth metatarsal base. Strength testing showed that eversion was associated with discomfort compared to the opposite foot.
Radiology
Radiographs revealed a smooth-edged, radiolucent line at the base of the fifth metatarsal (Fig. 1).
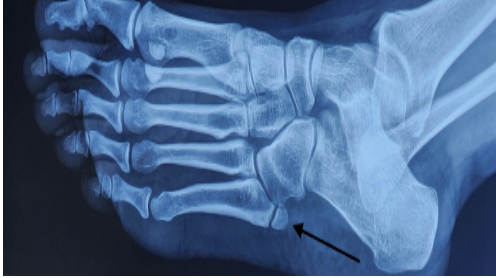
Figure 1: Pre-operative X-ray showing Os vesalianum at the base of the fifth metatarsal.
It did not appear likely that there had been a prior fracture in the absence of trauma. Opposite foot radiographs were unremarkable (Fig. 2).
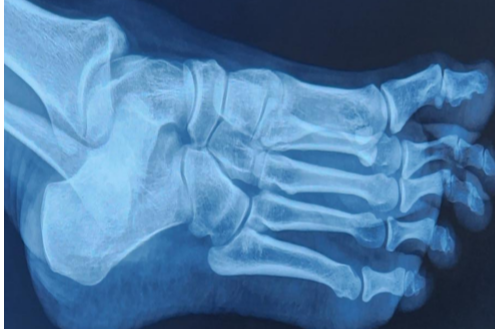
Figure 2: X-ray of the opposite foot without Os vesalianum.
Magnetic resonance imaging (MRI) and computed tomography (CT) were done to confirm the diagnosis and rule out other possibilities.
CT showed sclerotic ends at the junction of the OVP and fifth metatarsal (Fig. 3).

Figure 3: Shows a computed tomography image confirming Os vesalianum with smooth sclerotic ends between the accessory bone and the fifth metatarsal.
MRI confirmed pseudoarthrosis with a thin line of fluid between bone ends and showed no other injuries (Figs. 4 and 5).
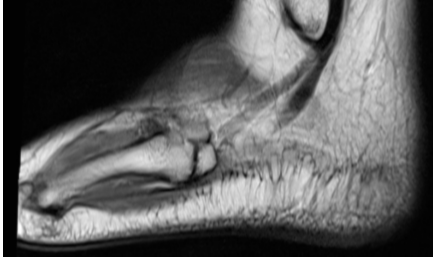
Figure 4: Magnetic resonance imaging T1 image showing Os vesalianum with smooth ends like synchondrosis and in continuity with the peroneus brevis tendon.

Figure 5: Magnetic resonance imaging T2 image showing fluid in the gap between Os vesalianum and the fifth metatarsal, suggestive of pseudoarthrosis or degenerative process.
Considering the severity of the pain and no response to conservative measures, operative treatment was offered.
Surgery
Centered over the base of the fifth metatarsal, a 4-cm longitudinal incision was made to expose the peroneus brevis tendon. The tendon’s superior two-thirds was separated from the fifth metatarsal tuberosity and split in line in accordance with its fibers (Fig. 6).

Figure 6: Intraoperative image showing accessory bone proximal to the fifth metatarsal (needle positioned for confirmation) and peroneus brevis tendon partly split and retracted.
The bony discontinuity was identified and confirmed radiologically. The accessory ossicle was excised from the metatarsal base. The released peroneus brevis tendon (Fig. 7) after excising the OVP in fragments (Fig. 8) was reattached to the base of the fifth metatarsal using a double-loaded suture anchor (Fig. 9).

Figure 7: After excision of Os vesalianum, the peroneus brevis was repaired to the fifth metatarsal base with a double-loaded suture anchor.

Figure 8: Excised accessory ossicle fragments.

Figure 9: Post-operative X-ray showing suture anchor placed into the fifth metatarsal after excision of the accessory bone, along with pseudoarthrosis.
A walking boot cast was given for 3 weeks, and full weight bearing was allowed as per tolerance and range-of-motion exercises were started outside the boot. The walking boot was removed 3 weeks after surgery, and the patient resumed routine activities 3 weeks later with no residual pain (VAS 0/10). When compared to the contralateral side, the patient’s strength was normal, and she was pain-free until the 9-month follow-up.
Diagnosis
The majority of reported OVP cases are asymptomatic and unilateral. They are usually discovered by chance on radiographs when taken for ankle sprains with no clinical tenderness on the fifth metatarsal [8,9,10]. When patients present with an ankle sprain, there is a chance of confusion with a fifth metatarsal base fracture [7]. The literature shows a few cases of incidentally identified OVP when presented due to other foot problems [11].
A few of the symptomatic cases reported were shown to have presented with an acute onset of lateral foot pain [10,12,13]. Some authors reported OVP causing chronic lateral border foot pain. Kim et al., [12] Dorrestijn and Brower, [14] and Aykanat et al., [15] have reported cases of lateral foot pain due to OVP, which was confirmed by scintigraphy showing active uptake [12]. OVP leading to chronic lateral foot pain has been reported by Husain et al., [16] though they responded to conservative measures.
This clearly defines the importance of clinical examination in identifying the source of pain and differentiating other causes of lateral foot pain, like avulsion fracture or non-union of the fifth metatarsal tuberosity, Iselin’s disease, Jones fracture, stress fracture, and Os peroneum. Characteristics that radiologically confirm OVP are the smooth opposing surfaces of bone ends [17], the presence of fluid between bone ends, such as pseudoarthrosis [18]. Hence, CT and MRI are valuable in evaluating a symptomatic patient with OVP identified in an X-ray. Scintigraphy may be used to confirm and exclude other causes if available.
Management
All asymptomatic cases may be reassured and closely followed up, explaining the chance of the development of pain. The treatment of symptomatic OVP with an acute onset of pain should start with conservative methods. Rest or activity modification, shoe inserts, stretching exercises, and non-steroidal anti-inflammatory medications are the most commonly used traditional treatment modalities. Only a single case of chronic lateral foot pain responding to conservative management has been reported [16]. All incidentally detected and symptomatic cases managed conservatively are summarized in Table 1.
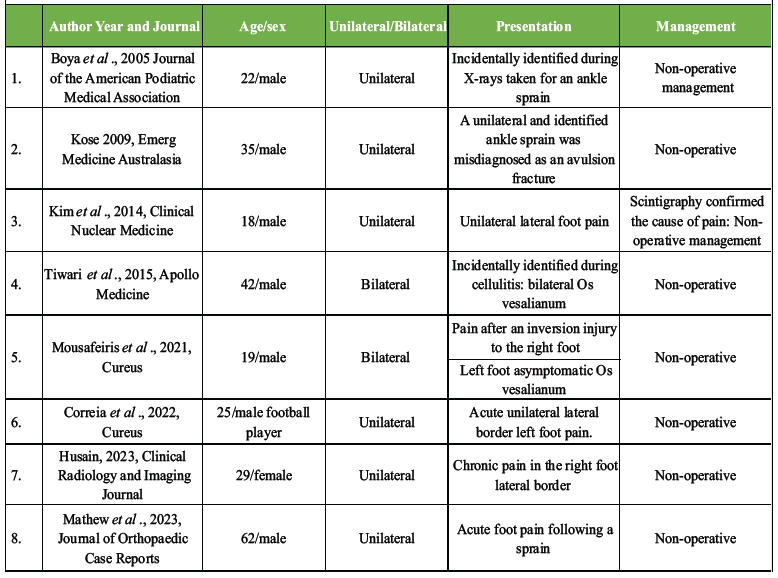
Table 1: The list of conservatively managed Os vesalianum cases (incidentally identified and symptomatic cases)
Most of the chronic and refractory symptomatic OVP cases were managed by surgery. Before any surgical intervention, it should be ensured that the actual cause of lateral foot pain is the OVP. In other words, other possible causes of lateral foot pain should be excluded to avoid overtreatment. Two different surgical techniques have been described in the reported cases. One of them is excision of the ossicle with repair of the peroneus brevis tendons, and the other is osteosynthesis with fixation of the ossicle to obtain fusion between the ossicle and the fifth metatarsal.
Only one pediatric case (13-year-old child) was reported by Inoue et al. in 1999, managed by osteosynthesis with bone grafting, with a successful outcome [19]. This is the only pediatric case reported and managed by osteosynthesis.
Chan et al. [18] described two cases of OVP managed by percutaneous diagnostic injection. First was a 20-year-old male football player managed by targeted injection under fluoroscopy with contrast given between the OVP and 5th metatarsal, who was found to be communicating with the 3rd and 4th tarsometatarsal joints. The 2nd case was a 39-year-old female runner, managed by ultrasound-assisted injection for pain relief.
Baastrup in 1922, Smith et al. in 1984, and Miswan et al. in 2014 have reported better outcomes with excision of OVP alone [6,20,21]. Miswan et al. reported a case that was confused for a fracture and, though prepared for fixation, ended up excising the ossicle with no need for tendon repair, with an excellent outcome. All other cases, presented after skeletal maturity, were managed by excision of the OVP and repair of the peroneus brevis tendon. The list of previously reported cases managed by surgery is summarized in Table 2.
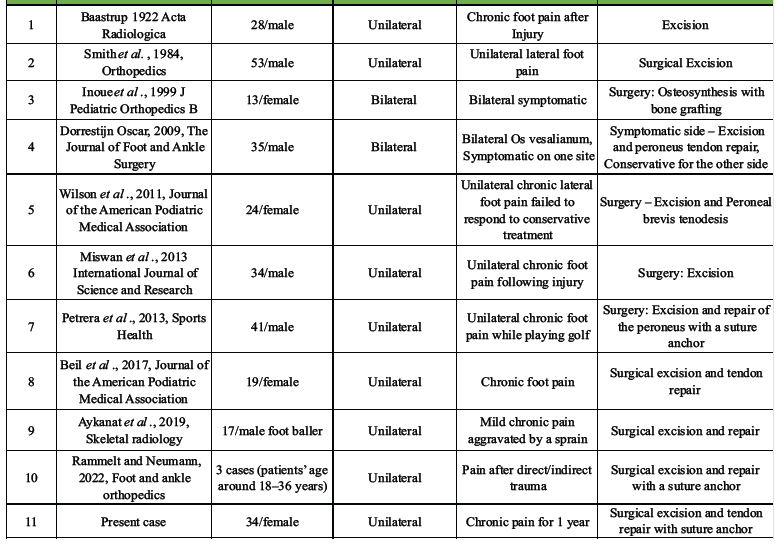
Table 2: The list of reported Os vesalianum symptomatic cases managed by various surgical procedures
Six authors have shown their cases, managed along with tendon repair, as in our case. Rammelt and Neumann [22] reported three cases in 2022, Dorrestijn and Brower [14], Wilson et al., [23], Petrera et al., [24] Beil et al., [25] and Aykanat et al. [15] have all reported cases managed by excision and tendon repair.
Good functional outcomes have been documented for both therapies. When the peroneus brevis is released from the ossicle, sometimes it becomes necessary to repair the tendon. In the present case, as per the literature, we chose to remove the accessory bone and repair the peroneus brevis with a suture anchor. This allows for strong fixation, quick recovery, and a quick return to normal without running the risk of non-union that comes with trying to create osteosynthesis and weak evertors if the Peroneus brevis is not repaired.
An image-guided diagnostic block is an option to consider for pain relief, which is the least reported in the literature for OVP [18]. Percutaneous radiofrequency ablation is also one option that may be considered in the future as a measure to give pain relief while avoiding surgery. However, pain relief and a return to pain-free activity must be considered in any modality of treatment.
OVP must be considered in patients presenting with chronic lateral foot pain. A thorough clinical examination and radiology will confirm the diagnosis. In symptomatic patients with failed conservative management, surgical excision of the OVP and suture anchor repair of the peroneus brevis is recommended for better patient recovery and quick resumption of sports activities.
Thorough clinical knowledge and familiarity with accessory ossicles in the foot are required to reassure normal cases and avoid confusion and mismanagement. A careful clinical examination is essential to accurately identify the source of pain or disability and to guide the appropriate method of treatment. In symptomatic cases like OVP, appropriate treatment can prevent chronic pain or disability, and an early return to sports or active life can be ensured.
References
- 1. O’Rahilly R. A survey of carpal and tarsal anomalies. J Bone Joint Surg Am 1953;35-A:626-42. [Google Scholar] [PubMed]
- 2. Candan B, Torun E, Dikici R. The prevalence of accessory ossicles, sesamoid bones, and biphalangism of the foot and ankle: A radiographic study. Foot Ankle Orthop. 2022;7(1):24730114211068792. [Google Scholar] [PubMed]
- 3. Coskun N, Yuksel M, Cevener M, Arican RY, Ozdemir H, Bircan O, et al. Incidence of accessory ossicles and sesamoid bones in the feet: A radiographic study of the Turkish subjects. Surg Radiol Anat 2008;31:19-24. [Google Scholar] [PubMed]
- 4. Vesalius A. De Pedis Ossibvs. De Humani Corporis Fabrica, 142, 1543. [Google Scholar] [PubMed]
- 5. Pitchandi M, Adibatti M, Bhuvaneswari V. Radiological study on the incidence and clinical importance of os vesalianum of 5th metatarsal bone. Inter J Anat Radiol Surg 2019;8:AO09-11. [Google Scholar] [PubMed]
- 6. Smith AD, Carter JR, Marcus RE. The os vesalianum: An unusual cause of lateral foot pain a case report and review of the literature. Orthopedics 1984;7:86-9. [Google Scholar] [PubMed]
- 7. Kose O. Os vesalianum pedis misdiagnosed as fifth metatarsal avulsion fracture. Emerg Med Aust 2009;21:426. [Google Scholar] [PubMed]
- 8. Boya H, Özcan Ö, Tandoğan R, Günal İ, Araç Ş. Os vesalianum pedis. J Am Podiatr Med Assoc 2005;95:583-5. [Google Scholar] [PubMed]
- 9. Mousafeiris VK, Papaioannou I, Kalyva N, Arachoviti C, Repantis T. Os vesalianum pedis in a young adult: A case report and literature review. Cureus 2021;13:e14896. [Google Scholar] [PubMed]
- 10. Mathew AJ, Hugh C, Nath S, Pillai MG. Red herring in orthopedics: A case report on painful os vesalianum pedis masquerading as an avulsion fracture of 5th metatarsal and review of literature. J Orthop Case Rep 2023;13:74-8. [Google Scholar] [PubMed]
- 11. Tiwari M, Khanna V, Kodide U, Vaishya R. Os vesalianum – A confounding diagnosis. Apollo Med 2015;12:285-6. [Google Scholar] [PubMed]
- 12. Kim MH, Kim WH, Kim CG, Kim DW. Os vesalianum pedis detected with bone SPECT/CT. Clin Nucl Med 2014;39:e190-2. [Google Scholar] [PubMed]
- 13. Correia MC, Lopes TR. Knowing your accessory foot ossicles and avoiding misdiagnoses: A case report of painful os vesalianum pedis. Cureus 2022;14:e27380. [Google Scholar] [PubMed]
- 14. Dorrestijn O, Brouwer RW. Bilateral symptomatic os vesalianum pedis: A case report. J Foot Ankle Surg 2011;50:473-5. [Google Scholar] [PubMed]
- 15. Aykanat F, Vincenten C, Cankus MC, Kose O, Sindel M. Lateral foot pain due to os vesalianum pedis in a young football player; a case report and review of the current literature. Skeletal Radiol 2019;48:1821-8. [Google Scholar] [PubMed]
- 16. Husain ZS. Symptomatic os vesalianum pedis in young adult: A case report. Clin Radiol Imaging J 2023;7:000198. [Google Scholar] [PubMed]
- 17. Keles-Celik N, Kose O, Sekerci R, Aytac G, Turan A, Güler F. Accessory ossicles of the foot and ankle: Disorders and a review of the literature. Cureus 2017;9:e1881. [Google Scholar] [PubMed]
- 18. Chan BY, Markhardt BK, Williams KL, Kanarek AA, Ross AB. Os conundrum: Identifying symptomatic sesamoids and accessory ossicles of the foot. AJR Am J Roentgenol 2019;213:417-26. [Google Scholar] [PubMed]
- 19. Inoue T, Yoshimura I, Ogata K, Emoto G. Os vesalianum as a cause of lateral foot pain: A familial case and its treatment. J Pediatr Orthop B 1999;8:56-8. [Google Scholar] [PubMed]
- 20. Baastrup CI. Os vesalianum tarsi and fracture of tuberositas ossis metatarsi v. Acta Radiol 1922;1:334-48. [Google Scholar] [PubMed]
- 21. Miswan MF, Hussin AR, Thangaraju S. Misdiagnosed os vesalianum as fifth metatarsal avulsion fracture: A case report. Int J Sci Res 2013;4:1874-5. [Google Scholar] [PubMed]
- 22. Rammelt S, Neumann AP. Resection of a symptomatic os vesalianum with peroneus brevis reattachment: A report of 3 cases and literature review of 100 years. Foot Ankle Orthop. 2022;7(4):2473011421S00892. [Google Scholar] [PubMed]
- 23. Wilson TC, Wilson RC, Ouzounov KG. The symptomatic os vesalianum as an uncommon cause of lateral foot pain: A case report. J Am Podiatr Med Assoc 2011;101:356-9. [Google Scholar] [PubMed]
- 24. Petrera M, Dwyer T, Ogilvie-Harris DJ. A rare cause of foot pain with golf swing: Symptomatic os vesalianum pedis-a case report. Sports Health 2013;5:357-9. [Google Scholar] [PubMed]
- 25. Beil FT, Burghardt RD, Strahl A, Ruether W, Niemeier A. Symptomatic os vesalianum: A case report and review of the literature. J Am Podiatr Med Assoc 2017;107:162-5. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 A Rare Pediatric Cause of Lateral Foot Pain: Symptomatic Os Vesalianum Pedis Requiring Excision and Peroneus Brevis Repair
June 1, 2026 A Rare Pediatric Cause of Lateral Foot Pain: Symptomatic Os Vesalianum Pedis Requiring Excision and Peroneus Brevis Repair June 10, 2023 Red Herring in Orthopedics: A Case Report on Painful Os Vesalianum Pedis Masquerading as an Avulsion Fracture of 5th Metatarsal and Review of Literature
June 10, 2023 Red Herring in Orthopedics: A Case Report on Painful Os Vesalianum Pedis Masquerading as an Avulsion Fracture of 5th Metatarsal and Review of Literature June 20, 2021 Eosinophilic Granulomatosis with Polyangiitis that was Difficult to Distinguish from Peroneal Nerve Palsy and Lumbar Disc Herniation: A Case Report
June 20, 2021 Eosinophilic Granulomatosis with Polyangiitis that was Difficult to Distinguish from Peroneal Nerve Palsy and Lumbar Disc Herniation: A Case Report January 1, 2026 Letter Re: “Faculty Development and Support in Orthopedic Education: A Narrative Review”
January 1, 2026 Letter Re: “Faculty Development and Support in Orthopedic Education: A Narrative Review”