
While corticosteroid injections for various pathologies of the hand are largely well-tolerated, the risk of flexor tendon rupture after injection is not zero.
Dr. Timothy Baker, Orlando Health Jewett Orthopedic Institute, Orlando, Florida, USA. E-mail: P-tbaker@orlandohealth.com
Abstract
Introduction: Finger flexor tendon injuries commonly occur as a result of direct trauma. On rare occasions, spontaneous ruptures can occur. Many pathologic processes have been described in the literature contributing to spontaneous finger flexor tendon ruptures, with most leading to progressive weakening of the tendon until it ultimately fails. We present a unique case of a Zone III spontaneous combined flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) rupture of the small finger in a 66-year-old female, 3 weeks after a corticosteroid injection for trigger finger. To the best of our knowledge, this is the only report of a small finger combined FDS/FDP rupture after a single corticosteroid injection.
Case Report: A 66-year-old female presented with the inability to flex her right small finger for the past 4 days, after injuring it at the gym. She had previously received one corticosteroid injection into her small finger for the treatment of the trigger finger approximately 3 weeks prior. Magnetic resonance imaging revealed rupture of both finger flexors of the small finger at the level of the mid metacarpal shaft, with at least 1 cm of separation. Reconstruction of the small finger FDP was performed using the FDS as an intercalary graft without complication. At the 6-week follow-up visit, she was doing well, able to flex both her proximal and distal interphalangeal joints actively. She experienced some stiffness but had an almost complete range of motion. She was pleased with the results at that time.
Conclusion: This case demonstrates a unique complication of non-operative treatment of trigger finger. While it will ultimately not change our institution’s treatment of trigger finger, it will lead to our team becoming more aware of the impact of corticosteroid injections and the need to inform patients to ease back into physical activity following injection.
Keywords: Finger flexor rupture, finger flexor reconstruction, trigger finger injection complication.
The incidence of traumatic tendon injuries involving the hand and wrist is reported to be as high as 33.2 injuries/100,000 persons/years, with the incidence of spontaneous finger flexor tendons expected to be substantially lower [1,2]. Spontaneous flexor tendon rupture can be defined as a tear of the tendon substance without any contributing pathologic processes or direct trauma [2]. While most atraumatic flexor tendon ruptures are thought to be spontaneous upon initial presentation, an underlying pathology is often identified that directly contributed to the rupture. Several case reports have identified secondary causes that contributed to rupture, including non-union of a hamate fracture, ulnar head osteophyte, pisotriquetral arthritis, pisotriquetral instability, chronic radioulnar dissociation, rheumatoid arthritis, infection after a cat bite, Kienboch’s disease, and corticosteroid injections [3,4,5,6,7,8,9,10,11].
The limited reports of spontaneous flexor tendon ruptures suggest that the most common injury pattern is an isolated small finger flexor digitorum profundus (FDP) Zone III tear, with the combined flexor digitorum superficialis (FDS) and FDP small finger tendon rupture being a rare phenomenon [12,13]. We report a case of a Zone III spontaneous combined FDS and FDP tendon rupture of the small finger in a 66-year-old female, approximately 3 weeks after receiving a corticosteroid injection for trigger finger.
History of Present Illness
A 66-year-old female, in good health, presented to the office with complaints of inability to flex her right small finger for the past 4 days. The patient reported that she was at the gym performing deadlifts when she felt a pop in her right hand. She was immediately unable to flex her small finger. Of note, she was diagnosed with trigger finger of her small finger approximately 3 weeks prior, at which time she received a corticosteroid injection. Other relevant past medical history is a history of carpal tunnel of the bilateral wrists for which she had been receiving corticosteroid injections.
Physical examination revealed no tenderness to palpation over the small finger. There was an inability to actively flex the small finger metacarpophalangeal joint, proximal interphalangeal joint, or distal interphalangeal joint (Fig. 1).

Figure 1: Clinical photo of the right hand demonstrating the loss of both proximal interphalangeal joint and distal interphalangeal joint flexion when attempting to make a fist.
Full passive range of motion (ROM) and intact sensation over the small finger were apparent. She was able to flex and extend all other fingers with full strength and maintained small finger abduction and adduction. Carpal tunnel Tinel sign and Durkan compression test were positive. She had an intact palmaris longus.
Imaging
Three radiographic views of the right small finger were obtained, including posteroanterior, oblique, and lateral, demonstrating no acute fractures, dislocations, or joint space narrowing.
Magnetic resonance imaging revealed rupture of the small finger FDS and FDP tendons with at least 1 cm separation of the tendon fragments centered at the level of the mid metacarpal shaft, representing a Zone III injury.
Operation and follow-up
The patient was scheduled for small finger flexor tendon repair versus reconstruction with carpal tunnel release. Intraoperatively, we began by releasing the carpal tunnel. We then inspected the anatomy of the carpal tunnel, looking for any potential causes of this rupture. There were no prominent osteophytes or rough edges that could have contributed to the tendon rupture. Moving on to the finger flexors, the tears were visualized at the proximal aspect of the A1 pulley (Fig. 2).
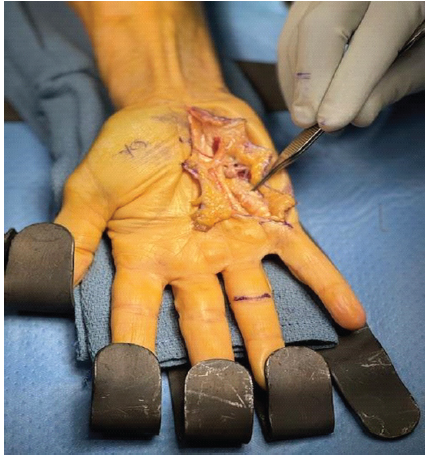
Figure 2: Intraoperative photo of the right hand demonstrating the distal stump of both finger flexors at the level of the proximal aspect of the A1 pulley.
The proximal stump of the FDP to the small finger was visualized at the level of the carpal tunnel with its shared muscle belly to the remaining digits (Fig. 3).
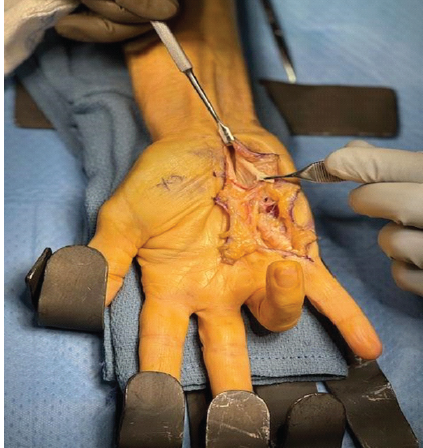
Figure 3: Intraoperative photo of the right hand demonstrating the proximal stump of both finger flexors just distal to the carpal tunnel.
The proximal stump of the FDS to the small finger had retracted proximal to the carpal tunnel. It was determined that a primary repair would not be feasible, and the decision was made to move forward with reconstruction of the FDP using a portion of the FDS as an intercalary graft. The FDS tendon was excised as high up as possible, which provided a 3-cm graft (Fig. 4).
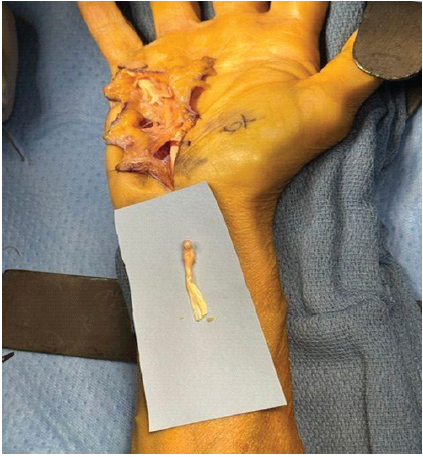
Figure 4: Intraoperative photo of the right hand demonstrating the approximately 3-cm flexor digitorum superficialis graft.
The attritional ruptured section of the FDS was excised, and a side-to-side weave of the distal stump of the FDP to the FDS graft was performed, using 3-0 Supramid in a running locking fashion. Then, a Pulvertaft and side-to-side weaves were performed to complete a coaptation and repair proximally. Careful attention was paid to the tension of the reconstructed tendon in order to avoid over-tensioning with the resulting quadrigia effect. Afterward, the repair was cycled multiple times and was found to be stable (Fig. 5).

Figure 5: Intraoperative photo of the right hand demonstrating the in situ reconstructed finger flexors with the small finger in extension.
Local anesthetic was injected, and sterile soft dressings were applied, as well as a dorsal blocking short-arm splint. At the 2-week follow-up, she was doing well with some stiffness. She was able to make a 50% composite fist, and the resting cascade to her small finger had been restored. She had an intact sensation of light touch on the small finger. At the 6-week follow-up, she was doing well with some residual stiffness. Her active finger flexion distance from her She had full passive ROM of the small finger and was able to pull through both the proximal and distal interphalangeal joints (Fig. 6).

Figure 6: Clinical photo of the right hand at 6-week post-operative visit showing the ability to make a fist, with assistance of the ring finger.
At that time, she had been completing occupational therapy and at-home exercises with improvement. She was compliant with her post-operative restrictions throughout the course. At 12 weeks her flexion contracture resolved and she had near full flexion.
To our knowledge, this is the only case report of small finger combined FDS/FDP tendon rupture occurring after a single corticosteroid injection for trigger finger. Given that intraoperatively there were no bony abnormalities that were contributing to the tendon tear, we believe the tear is directly related to the trigger finger injection. Of note, the patient is an avid weightlifter and injured her small finger while performing deadlifts. We hypothesize that the finger flexors could have already been weakened from repetitive microtrauma resulting from chronic loading of the finger flexors. The trigger finger injection could have weakened this tendon complex further until the ultimate tendon rupture occurred while performing deadlifts. The patient had also received multiple corticosteroid injections for carpal tunnel, which, although rare, has been reported in the literature to be associated with finger flexor rupture [14,15]. We believe that all three factors: singular trigger finger corticosteroid injection, multiple carpal tunnel injections, and chronic loading of the finger flexors with weightlifting, all contributed to her finger flexor rupture. Her finger flexors may have been weakened by the multiple corticosteroid injections combined with weightlifting; however, she did not fail until after the single trigger finger injection.
Stenosing flexor tenosynovitis, colloquially referred to as trigger finger, is a common pathology encountered in orthopedic hand surgery. It is commonly treated non-operatively with corticosteroid injections, with a cure rate seen between 60 and 90% [16,17,18]. While this common non-operative treatment has relatively high success rates, corticosteroids have been documented to lead to inhibition of tendon healing, increased tendon degeneration, and tendon rupture [19]. Golas et al. followed 401 patients over 22 years who had received corticosteroid injections for trigger finger and reported zero cases of flexor tendon rupture, demonstrating the rarity of this complication [20].
Fitzgerald et al. [10] discussed a case of a 77-year-old male who experienced a combined rupture of the middle finger FDS and FDP at the level of the A1 pulley after undergoing two corticosteroid injections for the trigger finger. Given that it had been around 11 months since the injury, treatment was a two-stage reconstruction. However, he was pleased with his results at his first follow-up and chose to forgo the second stage of reconstruction. This case differs in that the finger was injured and he received multiple corticosteroid injections. They also sent histologic specimens with examination revealing collagen necrosis consistent with intratendinous infiltration of steroids.
Oh et al. [21] discussed a similar case in a 57-year-old male with small finger FDP rupture after a single corticosteroid injection for trigger finger. They proposed that the injection, as well as repetitive microtrauma from playing golf, contributed to the injury. He underwent reconstruction using the palmaris longus autograft and was doing well with full ROM and strength at 5-month follow-up. This case differs in the fact that it was only an FDP injury, and the FDS was intact, as well as a palmaris longus autograft being used for reconstruction.
This case demonstrates a unique complication of non-operative treatment of trigger finger. While it will ultimately not change our institution’s treatment of trigger finger, it will lead to our team becoming more aware of the impact of corticosteroid injections and the need to inform patients to ease back into physical activity following injection.
While this report is unlikely to change treatment practices for trigger finger and carpal tunnel syndrome, it does shed light on a rare complication of corticosteroid injections to the hand. While it is often necessary to treat the combined conditions with corticosteroid injections, it is also necessary to be aware of the possible complications and to counsel patients accordingly.
References
- 1. De Jong JP, Nguyen JT, Sonnema AJ, Nguyen EC, Amadio PC, Moran SL. The incidence of acute traumatic tendon injuries in the hand and wrist: A 10-year population-based study. Clin Orthop Surg 2014;6:196-202. [Google Scholar] [PubMed]
- 2. Boyes JH, Wilson JN, Smith JW. Flexor tendon ruptures in the forearm and hand. J Bone Joint Surg 1960;42A:637-46. [Google Scholar] [PubMed]
- 3. Pajares-López M, Hernández-Cortés P, Robles-Molina MJ. Rupture of small finger flexor tendons secondary to asymptomatic nonunion of the hamate hook. Orthopedics 2011;34:142. [Google Scholar] [PubMed]
- 4. Hattori Y, Doi K, Hoshino S, Sakamoto S, Yukata K. Attritional rupture of the flexor tendons to the small finger caused by osteophyte of the ulnar head: Case report. J Hand Surg Am 2010;35:24-6. [Google Scholar] [PubMed]
- 5. Corten EM, Van Den Broecke DG, Kon M, Schuurman AH. Pisotriquetral instability causing an unusual flexor tendon rupture. J Hand Surg Am 2004;29:236-9. [Google Scholar] [PubMed]
- 6. Moritomo H, Masatomi T, Tada K. Attritional rupture of flexor tendons by the head of the ulna associated with a chronic longitudinal radioulnar dissociation. J Hand Surg Br 1998;23:126-9. [Google Scholar] [PubMed]
- 7. Ertel AN. Flexor tendon ruptures in rheumatoid arthritis. Hand Clin 1989;5:177-90. [Google Scholar] [PubMed]
- 8. Lewellyn B, Young M, Blanco P. Flexor tendon rupture after a cat bite – a case report of an uncommon sequela. J Orthop Case Rep 2024;14:83-8. [Google Scholar] [PubMed]
- 9. Turner K, Sheppard NN, Norton SE. Flexor tendon rupture due to previously undiagnosed Kienböck disease: A case report. Hand (N Y) 2017;12:NP37-8. [Google Scholar] [PubMed]
- 10. Fitzgerald BT, Hofmeister EP, Fan RA, Thompson MA. Delayed flexor digitorum superficialis and profundus ruptures in a trigger finger after a steroid injection: A case report. J Hand Surg Am 2005;30:479-82. [Google Scholar] [PubMed]
- 11. Tanaka T, Ogawa T, Yanai T, Okano E, Kohyama S, Ochiai N. Disruption of flexor tendon after intrasheath triamcinolone acetonide injection for trigger digits: Two case reports. J Hand Surg Asian Pac Vol 2017;22:380-3. [Google Scholar] [PubMed]
- 12. Bois AJ, Johnston G, Classen D. Spontaneous flexor tendon ruptures of the hand: Case series and review of the literature. J Hand Surg Am 2007;32:1061-71. [Google Scholar] [PubMed]
- 13. Naam NH. Intratendinous rupture of the flexor digitorum profundus tendon in zones II and III. J Hand Surg Am 1995;20A:478-83. [Google Scholar] [PubMed]
- 14. Hardie KA, Bergeson AJ, Anderson MC, Erie AC, Van Demark RE Jr. Flexor tendon rupture following repeated corticosteroid injections for carpal tunnel syndrome: A case report. Int J Surg Case Rep 2024;123:110277. [Google Scholar] [PubMed]
- 15. Gottlieb NL, Riskin WG. Complications of local corticosteroid injections. JAMA 1980;243:1547-8. [Google Scholar] [PubMed]
- 16. Hansen RL, Søndergaard M, Lange J. Open surgery versus ultrasound-guided corticosteroid injection for trigger finger: A randomized controlled trial with 1-year follow-up. J Hand Surg Am 2017;42:359-66. [Google Scholar] [PubMed]
- 17. Shultz KJ, Kittinger JL, Czerwinski WL, Weber RA. Outcomes of corticosteroid treatment for trigger finger by stage. Plast Reconstr Surg 2018;142:983-90. [Google Scholar] [PubMed]
- 18. Kosiyatrakul A, Loketkrawee W, Luenam S. Different dosages of triamcinolone acetonide injection for the treatment of trigger finger and thumb: A randomized controlled trial. J Hand Surg Asian Pac Vol 2018;23:163-9. [Google Scholar] [PubMed]
- 19. Lu H, Yang H, Shen H, Ye G, Lin XJ. The clinical effect of tendon repair for tendon spontaneous rupture after corticosteroid injection in hands: A retrospective observational study. Medicine (Baltimore) 2016;95:e5145. [Google Scholar] [PubMed]
- 20. Golas AR, Marcus LR, Reiffel RS. Management of stenosing flexor tenosynovitis: Maximizing nonoperative success without increasing morbidity. Plast Reconstr Surg 2016;137:557-62. [Google Scholar] [PubMed]
- 21. Oh J, Jo L, Lee JI. Do not rush to return to sports after trigger finger injection. Am J Phys Med Rehabil 2015;94:e26-30. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 April 10, 2016 Bilateral Spontaneous Midsubstance Patellar Tendon Rupture after Bilateral Total Knee Arthroplasty
April 10, 2016 Bilateral Spontaneous Midsubstance Patellar Tendon Rupture after Bilateral Total Knee Arthroplasty February 1, 2025 Atlantoaxial Instability in Neurofibromatosis Type 1: A Case Report
February 1, 2025 Atlantoaxial Instability in Neurofibromatosis Type 1: A Case Report October 10, 2021 Monteggia Variant with Salter-Harris Fracture of the Radial Head: Case Report and Litergature Review
October 10, 2021 Monteggia Variant with Salter-Harris Fracture of the Radial Head: Case Report and Litergature Review February 1, 2026 Knee Arthroscopy in Morbidly Obese Patients: Perioperative Challenges and Technical Considerations to Optimize Outcomes
February 1, 2026 Knee Arthroscopy in Morbidly Obese Patients: Perioperative Challenges and Technical Considerations to Optimize Outcomes