
Early recognition of CRMO through a multidisciplinary approach is crucial to avoid diagnostic delay and prevent long-term deformity and functional loss.
Mehmet Kaymakoglu, Department of Orthopedics and Traumatology, Izmir University of Economics, Medicalpoint Hospital, Yeni Girne Bulvarı, 1825. Sk. No:12, 35575 Karşıyaka/İzmir, Turkey. E-mail: kaymakoglumehmet@gmail.com
Abstract
Introduction: Chronic Recurrent Multifocal Osteomyelitis (CRMO) represents a chronic inflammatory bone condition which does not result from infectious pathogens. The non-bacterial osteomyelitis spectrum includes this condition, which affects children and teenagers through recurrent multifocal bone lesions. Although the exact etiology of CRMO remains unclear, current evidence suggests that autoinflammatory mechanisms play a significant role in its pathogenesis.
Case Report: A 10-year-old female patient presented with right shoulder pain. The patient described the pain as 6/10 in intensity. The pain increased over the past 3 days. There was no significant trauma or systemic history. Physical examination showed a deformity and swelling in the right shoulder, tenderness in the acromioclavicular joint, and restricted shoulder movements due to pain. Ultrasound, direct radiography, computed tomography, whole body-magnetic resonance imaging, and surgical biopsy performed.
Conclusion: CRMO should be considered in the differential diagnosis of pediatric patients presenting with unexplained bone pain and swelling, particularly when common etiologies have been ruled out. A multidisciplinary approach is required for early diagnosis and correct treatment of CRMO, which is a multifactorial disease. Early diagnosis and treatment can prevent functional losses and deformities that patients may experience.
Keywords: Chronic recurrent multifocal osteomyelitis, Clavicle, Pediatric, Non-bacterial
Chronic recurrent multifocal osteomyelitis (CRMO) represents a chronic inflammatory bone condition which does not result from infectious pathogens. The non-bacterial osteomyelitis spectrum includes this condition, which affects children and teenagers through recurrent multifocal bone lesions. Although the exact cause of CRMO remains unclear, it is widely believed that autoinflammatory processes play a key role in its development. The inflammatory reaction in bone tissue occurs via excessive proinflammatory cytokines, including interleukin IL-1, IL-6, and tumor necrosis factor-alpha [1]. Ferguson and Sandu identified genetic mutations in LPIN2, PSTPIP2, and IL1RN, which cause autoinflammatory syndromes that show similar pathological features to CRMO [2].
The disease manifests across different severity levels from asymptomatic to severe functional impairment. The main symptom of CRMO is bone pain at the affected body region. The early radiological features of CRMO include osteolytic lesions, which may later develop into areas of sclerosis and cortical thickening [3]. The metaphyseal regions of long bones – particularly the tibia and femur, are the most commonly affected sites in CRMO. Other reported regions that affected by CRMO are the pelvis, vertebrae, and mandible [3]. There are very few case reports on CRMO involving the clavicle.
The main challenge of CRMO is making the initial diagnosis. There are several differential diagnoses, including infectious osteomyelitis, Ewing sarcoma, osteosarcoma, neuroblastoma, leukemia, lymphoma, and Langerhans cell histiocytosis [4,5]. Therefore, a biopsy is warranted to exclude these conditions in the differential diagnosis. There are no specific markers for CRMO, and the only laboratory finding in routine blood tests is elevated C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) [6]. Bacterial culture also plays a key role in differentiating infectious osteomyelitis from other conditions [4]. The radiograph may appear normal in early stages or may have the appearance of an osteolytic lesion. In more advanced stages, irregular cortical thickening and changes resembling periosteal reaction may be observed on radiographs. However, computed tomography (CT) is the most effective imaging modality for demonstrating these alterations [5,6]. Whole – body magnetic resonance imaging (WB-MRI) is important for characterizing the lesion, as it more clearly demonstrates bone marrow edema and can reveal any soft-tissue invasion or related findings [3]. The Jansson criteria are widely used to support the diagnosis of CRMO, especially in challenging cases (Table 1).
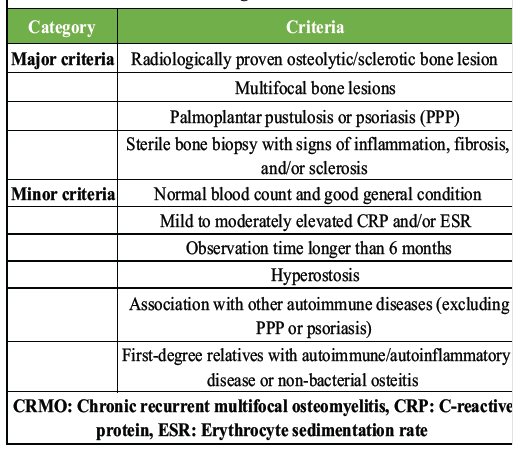
Table 1: Jansson diagnostic criteria for CRMO
According to these criteria, the diagnosis can be made when a patient meets either two major criteria or one major and three minor criteria. Major criteria include radiologically confirmed bone lesions, multifocal involvement, psoriasis or palmoplantar pustulosis, and a sterile bone biopsy showing inflammation or sclerosis. Minor criteria include normal blood tests and overall good health, mildly to moderately elevated CRP or ESR, symptoms lasting longer than 6 months, hyperostosis, association with other autoimmune diseases, or a family history of similar conditions. These criteria help clinicians differentiate CRMO from infections, malignancies, and other inflammatory bone diseases [7,8]. Bone biopsy is recommended to rule out malignancy and histopathologically shows non-specific inflammatory changes characterized by lymphocyte and histiocyte infiltration [5,6].
There is no consensus for treatment. However, the first choice treatment is non-steroidal anti-inflammatory drugs (NSAIDs) to control inflammation, decrease pain, and improve patient life quality [5,9]. The other treatment options are corticosteroids, methotrexate, or biologic therapies such as tumor necrosis factor-alpha inhibitors (TNFi) and bisphosphonates [5]. CRMO is characterized with frequent fluctuations. Therefore, long-term follow-up is essential to monitor disease progression and treatment response.
A 10-year-old female patient presented with a 2-year history of right shoulder pain. She had been evaluated by multiple physicians and received NSAIDs, which provided partial symptom relief. However, the pain recurred on discontinuation of the medication. The patient described the pain as mild to moderate in intensity. There was no history of trauma, fever, weight loss, or other systemic symptoms.
Her physical examination revealed that there was a deformity and swelling in the right shoulder, tenderness, and pain, especially in the sternoclavicular joint area, which limited shoulder movements, without any neurovascular deficit. Elevated ESR (80 mm/h) and CRP (0.8 mg/dL) were found in her blood tests with normal complete blood count, liver, and renal function.
No superficial soft-tissue mass was observed in the right clavicle on ultrasound. Shoulder X-ray revealed a bone expansion, cortical thickening, and sclerosis around an osteolytic lesion proximal – medial part of clavicle (Fig. 1).

Figure 1: Shoulder X-ray showing bone expansion, cortical thickening, and sclerosis surrounding an osteolytic lesion located in the proximal-medial part of the right clavicle.
CT examination showed an osteolytic lesion on the medial part of the clavicle, involving nearly 30% of the medial part of the clavicle and in close proximity to the sternoclavicular joint. The lesion was in the central and inferior part and had a 2.5 cm sharp transition zone (Fig. 2).
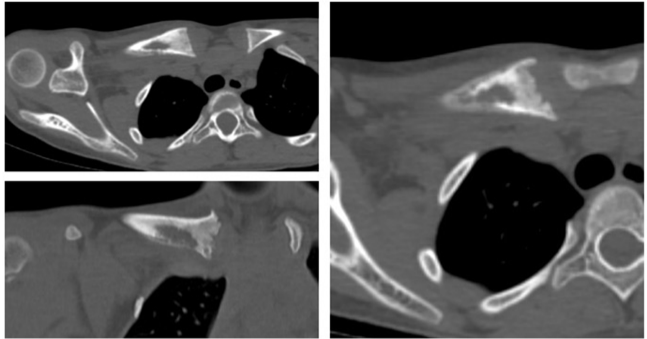
Figure 2: Computed tomography image demonstrating an osteolytic lesion involving approximately 30% of the medial clavicle, centrally and inferiorly located, with a sharp 2.5 cm transition zone and close proximity to the sternoclavicular joint. Joint space widening is observed, consistent with synovitis.
3D CT revealed hyperostosis of the right clavicle, consistent with a CRMO, while the left clavicle appeared normal (Fig. 3).

Figure 3: Right clavicle with hyperostosis and normal left clavicle on 3D computed tomography.
The sternoclavicular joint space was widened because of synovitis. WB-MRI showed T1-weighted hyperintense bone marrow edema that diffusely involving the medial 1/2 of the right clavicle, thickens the bone and causes remodeling, and contains a cystic area of 28 mm in diameter in the medial section. Diffuse heterogeneity is observed in adjacent fat tissue and muscle planes (Fig. 4). The periosteum appeared thinned in places. However, there is no aggressive lytic-destructive appearance.
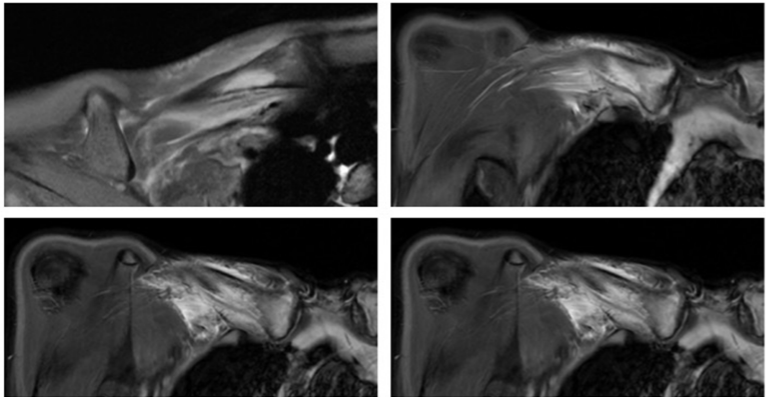
Figure 4: Whole-body magnetic resonance imaging showing T1-weighted hyperintense bone marrow edema diffusely involving the medial half of the right clavicle, associated with hyperostosis, bone remodeling, and a 28 mm cystic area in the medial portion.
The patient fulfilled the Jansson diagnostic criteria for CRMO, meeting two major criteria, radiologically proven bone lesion and sterile biopsy with inflammatory findings, and three minor criteria, including elevated inflammatory markers, normal blood counts with good general condition, and a symptom duration exceeding 6 months (Table A surgical biopsy was performed. While taking a biopsy, it was seen that the clavicle was completely covered with periosteal reaction, and the cortex continuity was disrupted in the anteroinferior portion.
Histopathological examination of the excised material, the largest measuring 1.5 × 0.8 × 0.03 cm with a volume of 5 cc, revealed chronic osteomyelitis with reactive osteoblastic activity and no evidence of neoplastic development; in line with later-stage disease, the tissue also showed monocytes, macrophages, lymphocytes, and plasma cells, along with multinucleated giant cells, osteolysis, and areas of bone necrosis accompanied by sclerosis and fibrosis.
Following a 2-month course of 10 mg daily naproxen, the patient experienced substantial pain relief and was able to engage more comfortably in daily activities with improved functional mobility.
CRMO is a rare autoinflammatory bone disease that poses considerable diagnostic challenges due to its insidious onset, non-specific symptoms, and the necessity to exclude other differential diagnoses such as infectious osteomyelitis or malignancies [10]. In our case, the patient had been symptomatic for 2 years and received only symptomatic treatment without a definitive diagnosis, underscoring the well-documented issue of diagnostic delay in CRMO. This delay has been consistently associated with worse clinical outcomes, including skeletal deformities, prolonged disease course, and unnecessary exposure to antibiotics or even suspicion of malignancy [11].
Although bone biopsy remains the gold standard for definitive diagnosis, particularly in unifocal or atypically located lesions such as the clavicle, the role of clinical suspicion and imaging particularly WB-MRI is increasingly emphasized. WB-MRI offers a non-invasive means to detect asymptomatic lesions, define the full extent of the disease, and assist in identifying characteristic patterns that may support the diagnosis in the absence of biopsy or in ambiguous cases [10]. Indeed, the patient described in this report presented with an isolated clavicular lesion, a rare location, and biopsy was necessary to exclude malignancy. However, if WB-MRI had been performed earlier, it might have expedited the diagnostic process and prevented unnecessary delay.
Recent literature has described four distinct radiological phenotypes in CRMO based on WB-MRI findings: tibio-appendicular multifocal pattern with tibial lesions, multifocal pattern without clavicular involvement, claviculospinal paucifocal pattern, and tibioclavicular crossover pattern [12]. Our patient’s presentation with an isolated clavicular lesion and absence of spinal or tibial involvement most closely fits the claviculospinal paucifocal pattern. This phenotype is typically characterized by a limited number of lesions localized to the clavicle and spine and is frequently mistaken for malignancy or bacterial osteomyelitis, leading to diagnostic delay. Recognizing these patterns may assist clinicians in differentiating CRMO from other bone pathologies and inform both prognosis and therapeutic planning.
Treatment of CRMO remains largely empirical due to the absence of standardized, evidence-based guidelines. NSAIDs are the recommended first-line therapy and are reported to be effective in controlling symptoms in up to 60% of patients [13]. In our case, treatment with naproxen resulted in pain relief and partial improvement in clavicular deformity, demonstrating the efficacy of NSAIDs in patients without systemic or spinal involvement. However, studies suggest that over half of patients eventually experience disease flares or require treatment escalation due to inadequate response or recurrence.
For patients who do not respond adequately to NSAIDs, particularly those with vertebral involvement or extensive multifocal disease, escalation to disease-modifying antirheumatic drugs (DMARDs), bisphosphonates, or TNFi is considered. DMARDs such as methotrexate and sulfasalazine have been used, although their effectiveness appears limited in retrospective analyses [7]. Bisphosphonates, particularly pamidronate, have shown significant efficacy in improving pain, reducing inflammation, and facilitating radiological resolution of bone lesions [7,14]. Their utility is especially notable in patients with vertebral involvement, where rapid control of osteolytic activity is essential to prevent collapse and long-term sequelae [10].
TNFi, including agents such as adalimumab and infliximab, have demonstrated benefit in refractory cases and are particularly useful in patients with systemic features or extraosseous involvement such as skin or gastrointestinal manifestations. However, their use is associated with potential side effects, including paradoxical psoriasis, and may not be universally accessible. Comparative data suggest that bisphosphonates may lead to faster radiological resolution, whereas TNFi may provide better control against disease flares over time [15].
Given the variability in clinical presentation, lesion distribution, and treatment response, a comprehensive and individualized approach is essential for the optimal management of CRMO. Early consideration of the diagnosis based on clinical suspicion, laboratory markers, and especially WB-MRI findings is crucial to prevent unnecessary investigations and prolonged morbidity. The identification of radiological phenotypes may further guide treatment selection, allowing more targeted and timely therapeutic interventions. The diagnosis and treatment of CRMO can be organized as a simple and practical clinical approach, as shown in Table 2.
In our case, the patient responded well to NSAID therapy, and she has remained symptom-free for the past 6 months without recurrence.
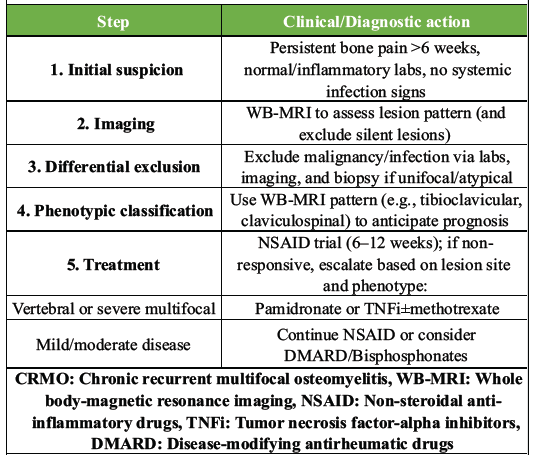
Table 2: Proposed clinical approach for suspected CRMO
CRMO remains a challenging condition to diagnose and manage due to its heterogeneity, non-specific presentation, and lack of definitive biomarkers. However, it should be considered in the differential diagnosis of pediatric patients presenting with unexplained bone pain and swelling, particularly when more common etiologies have been ruled out. Increasing awareness of its clinical and imaging features, especially the value of whole-body MRI and the utility of a phenotype-based approach, can significantly improve diagnostic accuracy and therapeutic outcomes. Recent studies have shown that CRMO is associated with autoinflammatory mechanisms, and research on targeted treatments is ongoing. A multidisciplinary approach involving pediatricians, radiologists, pathologists, and orthopedic specialists is essential for early diagnosis and appropriate management of this multifactorial disease. Early initiation of NSAID therapy remains the cornerstone of treatment, while escalation to immunomodulatory agents should be considered in cases with inadequate response or severe involvement. As demonstrated in this case, even rare presentations such as isolated clavicular lesions can achieve favorable outcomes when managed through a structured, evidence-guided diagnostic and therapeutic strategy.
Early recognition of CRMO is essential to avoid misdiagnosis and unnecessary invasive procedures. Whole-body MRI and a multidisciplinary approach play a key role in timely diagnosis and effective management, even in rare presentations such as isolated clavicular involvement.
References
- 1. Hassan M, Assi H, Hassan M, Bies JJ, Prakash S, Hassan A, et al. Chronic recurrent multifocal osteomyelitis: A comprehensive literature review. Cureus 2023;15:e43118. [Google Scholar] [PubMed]
- 2. Ferguson PJ, Sandu M. Current understanding of the pathogenesis and management of chronic recurrent multifocal osteomyelitis. Curr Rheumatol Rep 2012;14:130-41. [Google Scholar] [PubMed]
- 3. Khanna G, Sato TS, Ferguson P. Imaging of chronic recurrent multifocal osteomyelitis. Radiographics 2009;29:1159-77. [Google Scholar] [PubMed]
- 4. Sergi CM, Miller E, Demellawy DE, Shen F, Zhang M. Chronic recurrent multifocal osteomyelitis. A narrative and pictorial review. Front Immunol 2022;13:959575. [Google Scholar] [PubMed]
- 5. Wipff J, Adamsbaum C, Kahan A, Job-Deslandre C. Chronic recurrent multifocal osteomyelitis. Joint Bone Spine 2011;78:555-60. [Google Scholar] [PubMed]
- 6. Taddio A, Zennaro F, Pastore S, Cimaz R. An update on the pathogenesis and treatment of chronic recurrent multifocal osteomyelitis in children. Paediatr Drugs 2017;19:165-72. [Google Scholar] [PubMed]
- 7. Andreasen CM, Jurik AG, Glerup MB, Host C, Mahler BT, Hauge EM, et al. Response to early-onset pamidronate treatment in chronic nonbacterial osteomyelitis: A retrospective single-center study. J Rheumatol 2019;46:1515-23. [Google Scholar] [PubMed]
- 8. Bhat CS, Anderson C, Harbinson A, McCann LJ, Roderick M, Finn A, et al. Chronic non bacterial osteitis- a multicentre study. Pediatr Rheumatol Online J 2018;16:74. [Google Scholar] [PubMed]
- 9. Hofmann SR, Kapplusch F, Girschick HJ, Morbach H, Pablik J, Ferguson PJ, et al. Chronic recurrent multifocal osteomyelitis (CRMO): Presentation, pathogenesis, and treatment. Curr Osteoporos Rep 2017;15:542-54. [Google Scholar] [PubMed]
- 10. Moreno-Mateo F, Perea SH, Onel KB. Chronic recurrent multifocal osteomyelitis: Diagnosis and treatment. Curr Opin Pediatr 2021;33:90-6. [Google Scholar] [PubMed]
- 11. Schnabel A, Range U, Hahn G, Berner R, Hedrich CM. Treatment response and longterm outcomes in children with chronic nonbacterial osteomyelitis. J Rheumatol 2017;44:1058-65. [Google Scholar] [PubMed]
- 12. Andronikou S, Mendes Da Costa T, Hussien M, Ramanan AV. Radiological diagnosis of chronic recurrent multifocal osteomyelitis using whole-body MRI-based lesion distribution patterns. Clin Radiol 2019;74:737.e3-15. [Google Scholar] [PubMed]
- 13. Zhao DY, McCann L, Hahn G, Hedrich CM. Chronic nonbacterial osteomyelitis (CNO) and chronic recurrent multifocal osteomyelitis (CRMO). J Transl Autoimmun 2021;4:100095. [Google Scholar] [PubMed]
- 14. Li C, Zhao Y, Zuo Y, Zhou Y, Zhang F, Liu S, et al. Efficacy of bisphosphonates in patients with synovitis, acne, pustulosis, hyperostosis, and osteitis syndrome: A prospective open study. Clin Exp Rheumatol 2019;37:663-9. [Google Scholar] [PubMed]
- 15. Schnabel A, Nashawi M, Anderson C, Felsenstein S, Lamoudi M, Poole-Cowley J, et al. TNF-inhibitors or bisphosphonates in chronic nonbacterial osteomyelitis? – Results of an international retrospective multicenter study. Clin Immunol 2022;238:109018. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2025 Chronic Recurrent Multifocal Osteomyelitis – A Case Report
August 1, 2025 Chronic Recurrent Multifocal Osteomyelitis – A Case Report July 1, 2026 Concurrent Occurrence of Dysplasia Epiphysealis Hemimelica involving Lateral Malleolus and Sinus Tarsi: Rare Case with Review of Literature
July 1, 2026 Concurrent Occurrence of Dysplasia Epiphysealis Hemimelica involving Lateral Malleolus and Sinus Tarsi: Rare Case with Review of Literature July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor June 1, 2026 Prospective Evaluation of Clavicle Fracture Osteosynthesis: Patient Satisfaction, Clinical, and Radiological Outcomes with Clavipectoral Fascial Plane Block
June 1, 2026 Prospective Evaluation of Clavicle Fracture Osteosynthesis: Patient Satisfaction, Clinical, and Radiological Outcomes with Clavipectoral Fascial Plane Block