
Navigation facilitates safe and precise removal of Hartshill rectangle and sublaminar wires in complex revision spine surgery, minimizing risks of neurological injury and excessive bone removal.
Dr. Parth K Shah, Department of Spine, Sancheti Institute of Orthopaedics and Rehabilitation, Pune, Maharashtra, India. E-mail: pkshah2012.ps@gmail.com
Abstract
Background: The Hartshill rectangle with sublaminar wiring was a widely used spinal stabilization method, now largely replaced by pedicle screw systems due to superior biomechanical stability and reduced neurological risks. However, removal of such constructs in revision surgeries poses significant challenges, including fibrosis, implant corrosion, and risk of dural injury.
Case Report: We report two cases requiring removal of previously implanted Hartshill constructs. The first patient, a 46-year-old female, presented with acute back pain and radiculopathy due to an L1 burst fracture and prior L2–L4 Hartshill instrumentation. The second patient, a 50-year-old male, presented with myelopathy from implant backout and cord compression at D12. Both underwent implant removal and revision with pedicle screw fixation under O-arm guidance. Intraoperative navigation allowed precise localization and safe removal of broken sublaminar wires, minimizing the risk of neural injury. One sublaminar wire adherent to fibrotic tissue was left in situ in the second case to avoid complications.
Conclusion: Hartshill construct removal can be technically demanding due to fibrosis, metallosis, and broken sublaminar wires. The use of intraoperative navigation enhances safety and precision in revision spine surgery, making it a valuable adjunct in managing such complex cases.
Keywords: Hartshill rectangle, o-arm navigation, revision surgery.
Luque [1] was the first to introduce sublaminar wiring (SLW) for posterior stabilization of the spine in 1984. In Luque’s method, wires were combined with two different rods. The Hartshill system was later developed by Dove in 1986 to improve rotational stability by combining the two Luque rods into a rectangular shape [2]. It is attached to the spine in a rectangular pattern with two wire loops at each level. Comparing this configuration to the first single-loop approach, it has shown better biomechanical performance [3].
Sublaminar wires are no longer widely utilized due to advances in spinal instrumentation and surgical methods [4]. Major worries about them are neurological issues such as dural tears [5], anxiety about the long-term negative effects on the spinal cord, and wire and rod fractures – insufficient corrective pressures.
Classic posterior instrumentation relies solely on the purchase of posterior column structures, whereas pedicle screws allow for direct control of all three columns.
The revision involving the removal of the Hardshell rectangle and SLW is equally complex, with the possibility of dural rupture and wire breakage in the canal. As vital as proper sublaminar wire insertion is, its removal is equally challenging, with the same challenges and hazards. With the newer instrumentation available such as pedicle screws, the knowledge of the Hartshill rectangle and sublaminar wires becomes absolute. Revision spine surgeries increase with the latest advent of instrumentation. The technique for removing Hartshill was necessary.
We are illustrating the challenges and methods of removing Hartshill and sublaminar wires and revising them with pedicle screw implants under O-arm guidance.
Case Report 1
A 46-year-old female who was injured on her back while falling from her scooter presented with acute back pain (Visual Analog Scale 8/10) and difficulty in changing posture from supine to sitting. Left-sided hip flexion weakness 3/5 with left lower limb radicular pain in the upper thigh region. Bladder and bowel functions were normal.
We took a radiograph (Fig. 1), which indicated a previous L2–L4 Hartshill with sublaminar wires operation 15 years ago for an acute L2 burst fracture.
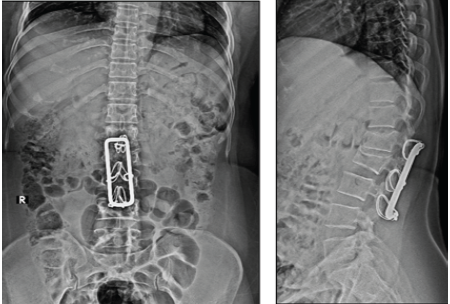
Figure 1: X-ray dorsolumbar spine-anteroposterior and lateral
At that time, the patient had left-sided knee extension and ankle dorsiflexion weakness 3/5, with left lower-limb radicular pain. After Hartshill with sublaminar wire, the patient recovered. Due to unsatisfactory visibility in magnetic resonance imaging (MRI) with Hartshill in situ, we chose computed tomography (CT) myelography (Fig. 2), which revealed an L1 burst fracture.
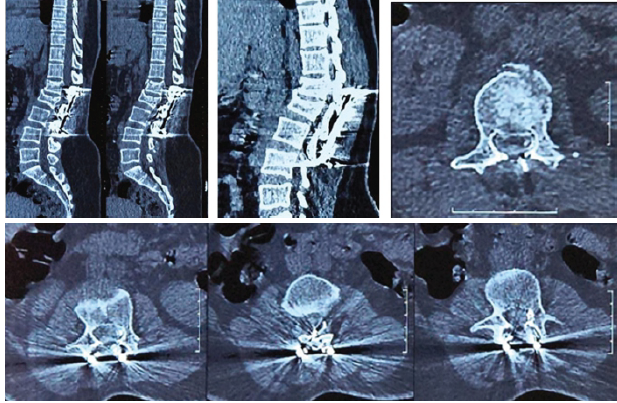
Figure 2: Computed tomography myelography showing no significant canal compression
With these investigations, the diagnosis of L1 burst fracture with the previous implant in situ was confirmed. Routine laboratory investigations were normal, and due to a history of trauma, the fracture was considered to be of traumatic origin. The patient was offered treatment in the form of revision surgery with the removal of the implant and instrumented fusion.
Surgery
The standard midline approach was used over the previous incision, and the spine was exposed. There were a lot of adhesions and fibrosis because of the previous surgery, which was carefully dissected. Here, we cannot use cautery over the stainless steel implant. We have to expose the rods from adherent tissue. The Hartshill rectangle was exposed (Fig. 3a), and the laminar wires looped over the implant were cut.
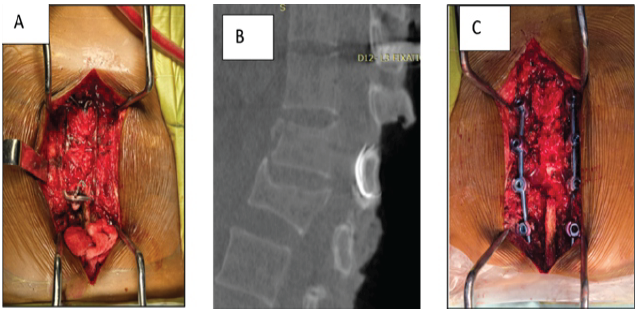
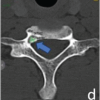
Figure 3: [A] Hartshill rectangle with sublaminar wire, [B] Broken sublaminar wire seen on computed
tomography scan under O-arm navigation, [C] Final construct with pedicle screws and rods
The post-operative patient was relieved of back pain and neurology was improved. The patient is walking with support on post-operative day 1 (POD1). Follow-up after 3 months, 6 months, and 12 months shows a well-maintained curve (Fig. 4).
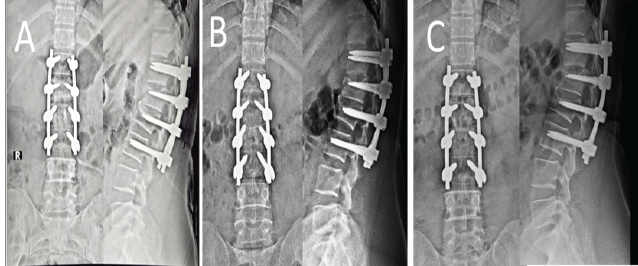
Figure 4: [A] Post-operative X-rays, [B] 3-month follow-up X-rays, [C] 12-month follow-up X-ray
A 50-year-old male presented with mid and lower back pain with spasticity and weakness in both lower limbs. The patient had myelopathic gait, with Nurick grade 4. Reflexes were hyper, and bowel/bladder not involved. Plantar reflexes were upward.
Radiographs were taken (Fig. 5), and they revealed that the procedure was previously performed from D12 to L4 with Hartshill rectangle and spinous process wires, with burst fractures of L1 and L4, implant back out, and breakage. An MRI and CT scan were done (Fig. 6), which showed cord compression at the D12 level due to implant breakage and kyphotic deformity at the proximal junctional level. The patient explained about the surgical intervention in the form of implant removal and instrumented fixation with decompression.
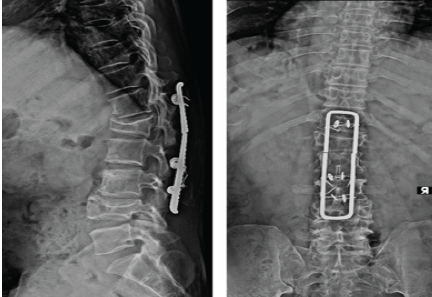
Figure 5: Pre-operative X-rays
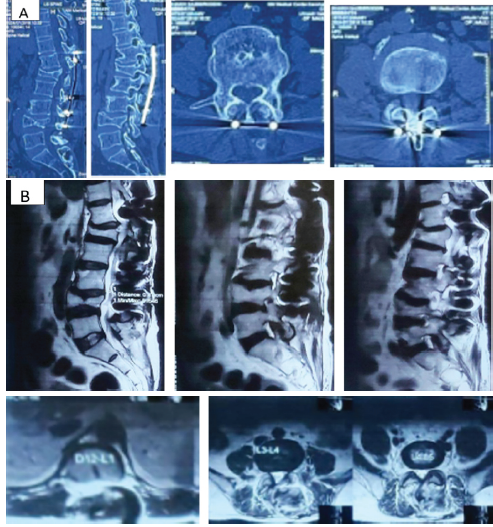
Figure 6: [A] Computed tomography scan showing retro pulsed fragment at L1 and L4.
[B] Magnetic resonance imaging showing cord compression at D12-L1 level and bothsided
foraminal stenosis at L4-L5 level.
Midline incision is placed over the previous incision. Implant exposure is done without the use of cautery. Spinous process wires were removed as discussed in the previous case, but L4 vertebrae laminar wire failed to be removed. Hartshill rectangle was found broken (Fig. 7) and explanted.

Figure 7: Hartshill rectangle (intraoperative image).
Pedicle screws were inserted under O-arm navigation from D10 to L4. Dorsal decompression was done. Rods were contoured and fixed to the screws. L4 sublaminar wire was tried to remove but was adherent with the fibrosis which will eventually lead to neurological complications so left in situ.
Postoperatively, gradually shifted to neurorehabilitation. The patient was able to walk with support from POD1 without any difficulty. At 3 months, the patient was able to walk without support, and lower limb power improved. The patient was followed up for 3 months, 6 months, and 9 months. Follow-up showed a well-maintained curve (Fig. 8).
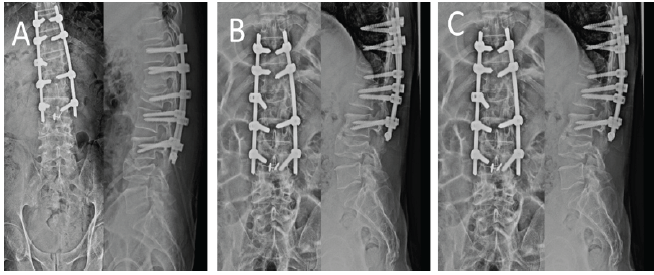
Figure 8: [A] Immediate post-operative X-ray. [B] 3-month post-operative X-ray. [C] 12-month follow-up X-ray.
Pedicle screw fixation of spinal fractures has supplanted sublaminar wire procedures in many facilities. Biomechanical studies have suggested that such systems provide greater stability than the Hartshill system, especially in rotation [6]. Difficulties in removing the Hartshill rectangle have not yet been studied in depth.
In vitro, corrosion is known to occur with stainless-steel implants [7,8,9,10]. It is seen less commonly with cobalt-chromium alloys and rarely with titanium. Corrosion may weaken the metal, and the late failure of segmental wires may be caused by a combination of repeated cyclical loading and fretting corrosion at the rod-wire junction. The potential for epidural fibrosis with passing the sublaminar wires in the canal may occur.
All these complications may further increase the risk of neurological damage during the removal of the sublaminar wires. We incorporated O-arm navigation to accurately extract the sublaminar wires, which would otherwise lead to significant bony destruction and harm to the neurological structures.
The removal of Hartshill rectangles and sublaminar wires during revision spine surgery is technically demanding due to fibrosis, implant breakage, and the risk of dural or neurological injury. Our experience demonstrates that O-arm navigation can facilitate safe and precise wire removal while minimizing bony destruction and potential complications.
Navigated removal of legacy spinal implants combined with pedicle screw fixation provides an effective and safer approach for complex spinal reconstructions in patients with previous Hartshill instrumentation.
References
- 1. Luque ER, editor. Segmental Spinal Instrumentation. Thorofare, NJ: Slack; 1984. [Google Scholar] [PubMed]
- 2. Dove J. Internal fixation of the lumbar spine. The Hartshill rectangle. Clin Orthop Relat Res 1986;203:135-90. [Google Scholar] [PubMed]
- 3. Dove J, Bottenburg H, Arnold P, Carter SR, Conway J. Biomechanical aspects of luque scgmcntal spinal instrumentation. In: Presented at the First European Congress on Scoliosis and Kyphosis. Dubrovnik; 1983. [Google Scholar] [PubMed]
- 4. Songer MN, Spencer DL, Meyer PR Jr., Jayaraman G. The use of sublaminar cables to replace luque wires. Spine (Phila Pa 1976) 1991;16 Suppl 8:S418-21. [Google Scholar] [PubMed]
- 5. Wilber RG, Thompson GH, Shaffer JW, Brown RH, Nash CL Jr. Postoperative neurological deficits in segmental spinal instrumentation. A study using spinal cord monitoring. J Bone Joint Surg Am 1984;66:1178-87. [Google Scholar] [PubMed]
- 6. Cresswell TR, Marshall PD, Smith RB. Mechanical stability of the AO internal spinal fixation system compared with that of the Hartshill rectangle and sublaminar wiring in the management of unstable burst fractures of the thoracic and lumbar spine. Spine (Phila Pa 1976) 1998;23:111-5. [Google Scholar] [PubMed]
- 7. Aulisa L, Di Benedetto A, Vinciguerra A, Lorini G, Tranquilli-Leali P. Corrosion of the Harrington’s instrumentation and biological behaviour of the rod-human spine system. Biomaterials 1982;3:246-8. [Google Scholar] [PubMed]
- 8. Mayor MB, Merritt K, Brown SA. Metal allergy and the surgical patient. Am J Surg 1980;139:477-9. [Google Scholar] [PubMed]
- 9. Merritt K, Brown SA. Tissue reaction and metal sensitivity. An animal study. Acta Orthop Scand 1980;51:403-11. [Google Scholar] [PubMed]
- 10. Scales JT, Winter GD, Shirley HT. Corrosion of orthopaedic implants. Smith-Petersen type hip nails. Br Med J 1961;2:478-82. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 O-arm Navigation-assisted Excision of Cervical Osteoid Osteoma Adjacent to the Vertebral Artery: Technical Note and Case Report
August 1, 2026 O-arm Navigation-assisted Excision of Cervical Osteoid Osteoma Adjacent to the Vertebral Artery: Technical Note and Case Report July 1, 2026 Combined Mechanical and Biological Salvage of Recalcitrant Subtrochanteric Non-union using Valgus Osteotomy, Blade Plate Fixation, and Endomedullary Fibular Graft
July 1, 2026 Combined Mechanical and Biological Salvage of Recalcitrant Subtrochanteric Non-union using Valgus Osteotomy, Blade Plate Fixation, and Endomedullary Fibular Graft October 1, 2025 Failed Primary Fixation of Monteggia Fractures – A Case Series
October 1, 2025 Failed Primary Fixation of Monteggia Fractures – A Case Series July 1, 2025 Revision of Total Hip Arthroplastys Using Short Femoral Stems: Is It Possible?
July 1, 2025 Revision of Total Hip Arthroplastys Using Short Femoral Stems: Is It Possible?