
Neurological symptoms in young pregnant females can be due to tumor-related bone diseases.
Dr. Deepthy Balakrishnan, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India. E-mail: obgyn_deepthy@aiimsbhubaneswar.edu.in
Abstract
Introduction: Aneurysmal bone cysts (ABCs) are benign yet locally aggressive osseous lesions characterised by blood-filled cystic cavities. Association of this tumor with pregnancy is rare and can cause diagnostic difficulties due to neurological manifestations and the rarity of the tumor.
Case Report: The report details our clinical experience managing a pregnant patient with an ABC presenting with neurological manifestations late in her pregnancy.
Discussion: Obstetric, neurological, vascular, infectious, and miscellaneous causes – including transverse myelitis, multiple sclerosis, metastatic lesions, Guillain-Barré syndrome, and spinal-epidural abscess – are differential diagnoses for patients with neurological symptoms. Magnetic resonance imaging remains the most effective diagnostic tool. Since there are no specific guidelines for managing obstetric patients with ABCs, cesarean delivery is advised for women in the third trimester, followed by spinal fixation procedures.
Conclusion: This case underscores the necessity of considering rare bone tumors when obstetric patients present with unusual symptoms such as paraparesis.
Keywords: Aneurysmal bone cysts, neurological manifestations, pregnancy.
Aneurysmal bone cysts (ABCs) are benign yet locally aggressive osseous lesions characterised by blood-filled cystic cavities [1]. They are rare, accounting for approximately 1–2% of all bone tumors [1].
The etiology of ABCs remains unknown, although they are often associated with USP6 gene rearrangements [2,3]. These lesions predominantly involve the metaphysis of long bones, with about one-third arising in the spine, constituting 15% of primary spinal tumors. In spinal cases, ABCs typically affect the posterior elements of the vertebrae, leading to local bone destruction, pain, and potential complications, including vertebral fractures, spinal instability, and neurological deficits from neural compression [4].
Association of this tumor with pregnancy is rare and can cause diagnostic difficulties due to neurological manifestations and the rarity of the tumor. This case report details our clinical experience managing a pregnant patient with an ABC presenting with neurological manifestations late in her pregnancy.
A 24-year-old patient was admitted at 38 weeks of gestation due to the sudden onset of lower limb weakness. This weakness began in the left lower limb and progressed over 5 days to involve both knees and thighs. On admission, she was unable to stand or walk independently and reported severe pain in her left knee. There were no bladder or bowel symptoms, fever, vomiting, or diarrhea, although she continued to perceive fetal movements. The patient’s obstetric history indicated that she was primiparous, with no significant antenatal complications or noteworthy medical history. On examination, the patient was conscious, oriented, and in generally good condition, with a healthy fetus. Neurological assessment revealed normal speech and reactive pupils, and no signs of meningitis or increased intracranial pressure. Motor evaluation showed normal power in the upper limbs and proximal lower-limb muscles; however, there was reduced tone in the distal lower-limb muscles, exaggerated deep tendon reflexes, and a flexor plantar reflex. Sensory examination demonstrated intact sensation in both upper and lower limbs, with an unaffected autonomic nervous system. Given the atypical clinical presentation, the differential diagnosis included spastic paraparesis or a lesion affecting the nerve roots of the spinal cord.
Labor commenced before radiological evaluation could be completed, and a cesarean section was performed due to the lack of a definitive diagnosis and the difficulties presented during labor positioning. A healthy baby weighing 2.7 kg was delivered.
Subsequent investigations to exclude immunological diseases were negative. Magnetic resonance imaging (MRI) of the whole spine revealed a multiseptated cystic lesion measuring 7.4 × 6.6 cm, which displaced the left psoas and paraspinal muscles, contributing to significant spinal canal stenosis (anteroposterior diameter of 3.4 mm). This affected both the exiting bilateral nerve roots and the cauda equina, in addition to a fracture, resulting in nearly complete collapse of the L3 vertebra. Findings were consistent with an ABC involving the L3 vertebra (Fig. 1).

Figure 1: Aneurysmal bone cyst involving the L3 vertebra.
Ultrasound-guided biopsy revealed dilated cystic spaces with mononucleated stromal cells and osteoclast-like giant cells. The intercystic spaces showed marked fibrosis, confirming the diagnosis.
The patient was referred to the neurosurgery department for evaluation and underwent posterior decompression with pedicle screw and rod fixation. During the initial surgery, the posterior elements of the L3 vertebra and part of the tumor were excised, with the bilateral L3 and L4 nerve roots preserved. Pedicle screws were placed at various levels from L1 to L5, and contour rods were secured. A subsequent surgical intervention was performed to excise the residual tumor, a 6 × 5 cm ABC at the L3 level, utilising a retroperitoneal approach. The procedure involved the removal of the encapsulated, vascularized, and fibrotic tumor in sections, 3 weeks subsequent to the initial operation.
Due to the absence of significant clinical improvement, a posterior segment re-exploration was conducted, resulting in the removal of a portion of the tumor adherent to the L3 nerve root. A 12 × 30 mm mesh cage was implanted into the L3 vertebral body space, and the minimal dural tear was repaired. The cage’s positioning was confirmed with a C-arm, and the rod was repositioned and tightened.
All Surgeries were conducted over a 2-month period. The patient required two procedures because the tumor could not be entirely removed during the initial surgery. Post-surgery, the patient exhibited symptomatic improvement, notably in the strength of her lower-limb muscles, although residual weakness in left foot dorsiflexion persisted. A foot splint was applied to support and facilitate her recovery. The diagnosis of aneurysmal cyst was confirmed through histopathological examination (Fig. 2).
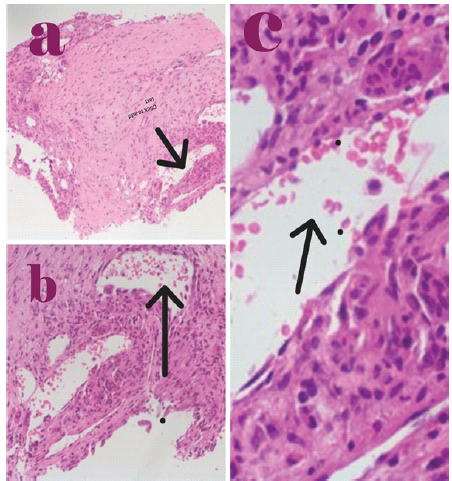
Figure 2: (a-c) The diagnosis of aneurysmal cyst was confirmed through histopathological examination.
The patient received rehabilitation in the physiotherapy unit. After 10 months of follow-up, she has fully recovered and can walk independently without support (Fig 3).

Figure 3: Sagittal computed tomography scan image post-surgery.
ABCs can be classified as primary or secondary, often arising before age 20, with a higher prevalence in females [5]. Approximately one-third of these tumors are located in the spine, which aligns with the age and site of occurrence noted in our case.
The precise etiology of ABCs remains unclear; however, it is hypothesised that they may result from hemodynamic changes in arteriovenous anastomoses, leading to venous outflow obstruction. This obstruction can subsequently lead to dilation and rupture of the local vascular network within the bone [5].
The incidence of ABCs during pregnancy is notably rare, with limited cases documented across various sites. The impact of pregnancy on the clinical behavior of these tumors is still not fully understood, as some instances report an increase in tumor size while others show regression [5,6,7].
Patients with ABC in the spine present with pain, unsteady gait, lower limb weakness, radiculopathy, local back swelling, Spastic paraparesis and decreased sphincter tone according to the site of involvement [8]. In our case, the patient experienced abrupt bilateral lower-limb weakness in the third trimester of pregnancy. A comparable instance of thoracic ABC manifesting as acute paraparesis in a pregnant patient has been previously documented [4].
MRI is the most effective diagnostic tool, revealing characteristic multiple fluid-fluid levels within a multiloculated, non-homogeneous lesion, particularly on T2-weighted images; however, this finding is not specific for an ABC [9]. Histopathological analysis remains the gold standard, typically demonstrating blood-filled spaces lined by fibroblasts, osteoclast-type giant cells, and reactive bone [5].
Differential diagnosis
Other differential diagnoses of these conditions include obstetric, neurological, vascular, infectious, and miscellaneous causes, such as transverse myelitis, multiple sclerosis, metastatic lesions, Guillain-Barré syndrome, and spinal-epidural abscess. Obstetric conditions include a gravid uterus compressing the lumbosacral plexus, prolonged lithotomy position, and complications of epidural anesthesia [10].
All the above conditions are ruled out using different hematological parameters and radiological investigations.
Outcome and follow-up
Management of ABCs during pregnancy necessitates a careful balance between maternal benefit and fetal safety. Options for treatment may range from conservative monitoring to surgical intervention, depending on factors such as lesion size, location, symptoms, and the associated risk of fracture or neurological compromise. Surgical procedures during pregnancy, particularly in the second trimester, are generally considered relatively safe when necessary. A multidisciplinary approach involving neurosurgery, orthopedics, obstetrics, and anesthesia is crucial. Key considerations include fetal monitoring, lateral positioning to avoid aortocaval compression, and minimizing operative time. Due to the absence of specific guidelines regarding the management of obstetric patients with ABCs, and given the risks of fractures and intralesional bleeding, cesarean delivery is advised for women presenting in the third trimester, followed by spinal fixation [5,6]. In our case, we opted for termination via cesarean section, with subsequent surgical intervention planned postpartum, as the patient had entered labor before definitive diagnosis.
This case underscores the necessity of considering rare bone tumors when obstetric patients present with unusual symptoms such as paraparesis. Individualized, multidisciplinary management during pregnancy can improve outcomes for both the mother and the child.
When women exhibit neurological symptoms during pregnancy, such manifestations are seldom attributed to an orthopedic origin. This article emphasizes the importance of excluding bone tumors, even in cases of acute neurological presentations. Furthermore, the obstetric management of pregnant women with osseous tumors is addressed.
References
- 1. Stevens KJ, Stevens JA. Aneurysmal bone cysts. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2025. [Google Scholar] [PubMed]
- 2. Nasri E, Reith JD. Aneurysmal bone cyst: A review. J Pathol Transl Med 2023;57:81-7. [Google Scholar] [PubMed]
- 3. Lau AW, Pringle LM, Quick L, Riquelme DN, Ye Y, Oliveira AM, et al. TRE17/ubiquitin-specific protease 6 (USP6) oncogene translocated in aneurysmal bone cyst blocks osteoblastic maturation via an autocrine mechanism involving bone morphogenetic protein dysregulation. J Biol Chem 2010;285:37111-20. [Google Scholar] [PubMed]
- 4. Li L, Tan LA, Wewel JT, Kasliwal MK, O’Toole JE. Spinal aneurysmal bone cyst presenting as acute paraparesis during pregnancy. J Clin Neurosci 2016;28:167-9. [Google Scholar] [PubMed]
- 5. Elkattah R, Foulk B. A suspected pelvic aneurysmal bone cyst in pregnancy. Case Rep Obstet Gynaecol 2012;2013:676087. [Google Scholar] [PubMed]
- 6. Stevens-Simon C, Stewart J, Nakashima II, White M. Exacerbation of fibrous dysplasia associated with an adolescent pregnancy. J Adolesc Health 1991;12:403-5. [Google Scholar] [PubMed]
- 7. Goel SR, Purohit D, Sekhawat J, Mittal RS. Aneurysmal bone cyst and pregnancy: Is there any association? Indian J Neurosurg 2015;4:185-9. [Google Scholar] [PubMed]
- 8. Aljoghaiman MS, Alhamad SM, Homan MA, Harfouch BF. Aneurysmal bone cyst of the spine: Report of four cases and review of the literature. Interdiscip Neurosurg 2019;16:18-21. [Google Scholar] [PubMed]
- 9. Dormans JP, Pill SG. Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-67. [Google Scholar] [PubMed]
- 10. Hosley CM, McCullough LD. Acute neurological issues in pregnancy and the peripartum. Neurohospitalist 2011;1:104-16. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Surgical Management of Pott’s Paraplegia in a 27-Week Pregnant Woman with Continuation of Pregnancy: A Case Report
May 1, 2026 Surgical Management of Pott’s Paraplegia in a 27-Week Pregnant Woman with Continuation of Pregnancy: A Case Report March 1, 2026 Knee Deep in Discovery: Incidental Contralateral Non-Ossifying Fibroma in an Adolescent Male – A Case Report
March 1, 2026 Knee Deep in Discovery: Incidental Contralateral Non-Ossifying Fibroma in an Adolescent Male – A Case Report October 1, 2025 A Rare Clinical Dilemma: Humeral Shaft Fracture in a Full-Term Pregnant Patient – A Case Report with Review of Literature
October 1, 2025 A Rare Clinical Dilemma: Humeral Shaft Fracture in a Full-Term Pregnant Patient – A Case Report with Review of Literature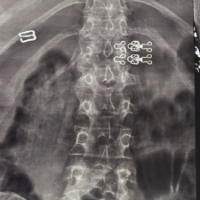 November 1, 2024 Pregnancy and Lactation Associated Osteoporosis in a 24-Year-Old Presenting with Multiple Fragility Fractures in the Dorsolumbar Spine: A Case Report and Review of Literature
November 1, 2024 Pregnancy and Lactation Associated Osteoporosis in a 24-Year-Old Presenting with Multiple Fragility Fractures in the Dorsolumbar Spine: A Case Report and Review of Literature