
We should examine patients with lower limb asymmetries not only from the perspective of limb length discrepancy but also considering gait abnormalities.
Dr. Junya Shimizu, Department of Orthopaedic Surgery, Sapporo Medical University School of Medicine, Sapporo, Japan. E-mail: jshimizu@sapmed.ac.jp
Abstract
Introduction: There are numerous etiologies relating to limb length discrepancy (LLD). Clinical manifestations of LLD may include gait abnormality and compensatory scoliosis. Congenital short femur (CSF) is a rare congenital skeletal abnormality with several manifestations, including coxa vara, abnormalities of the cruciate ligaments, hypoplasia of the lateral femoral condyle, fibular hemimelia, ball-in-socket ankle, and tarsal coalition.
Case Report: A 4-month-old female was referred to a primary care hospital following findings of LLD and significant thigh circumference discrepancy. She was initially monitored with regular radiographic assessment. On achieving independent standing, she was prescribed an orthosis. At the age of 3 years, she was referred to a specialized pediatric orthopedic facility because her LLD exceeded 3 cm. At the age of 8 years, her LLD had increased to 5.6 cm, and she suffered from gait abnormality. We thereafter performed several surgeries, including external fixation, contralateral epiphysiodesis, intramedullary nail insertion, and partial fibular resection, accompanied by three-dimensional gait analysis (3DGA), over the period from age 8.0 to 14.3 years. At age 14.3 years, LLD had improved to within 1 cm on radiographic findings. On 3DGA, her gait profile score improved from 20.4° at 8.0 years to 7.9° at 14.6 years, corresponding to 7.8 times the minimal clinically important difference.
Conclusion: This is the first report of both pre- and post-operative 3DGA across several surgeries for a patient with CSF. Although CSF is a challenging disorder, amelioration of LLD and avoidance of long-term immobilization across the knee joint might lead to improved gait function. Physicians who manage children involved with severe LLD should assess improvement not only based on radiographic findings but also on activities of daily living, including gait function.
Keywords: Congenital short femur, bone lengthening, epiphysiodesis, pathological fractures, three-dimensional gait analysis.
The etiologies of limb length discrepancy (LLD) include early physeal arrest, syndromes relating to hemihypertrophy or hypotrophy, and tumor [1,2]. Clinical manifestations of LLD may include gait abnormality and compensatory scoliosis, especially in younger children with more remaining growth. This report describes a case of right congenital short femur (CSF) and mid-term follow-up with instrumented three-dimensional gait analysis (3DGA) data over 6 years (age 8.0–14.3 years), during which the patient underwent several orthopedic surgeries. This report was approved by the institutional review board of the institution where the surgeries and measurements were performed.
Case: Four-month-old female
Chief complaint: LLD.
A 4-month-old female was referred to an orthopedic hospital following findings of LLD and significant thigh circumference discrepancy at a regular checkup (Fig. 1a). She was prescribed an orthosis and monitored, with regular radiographic assessments, until she reached the age of 3, when LLD exceeded 3 cm. At that time, she was referred to our facility for further treatment and follow-up (Fig. 1b). We continued conservative treatment, considering her young age (3.6 years).
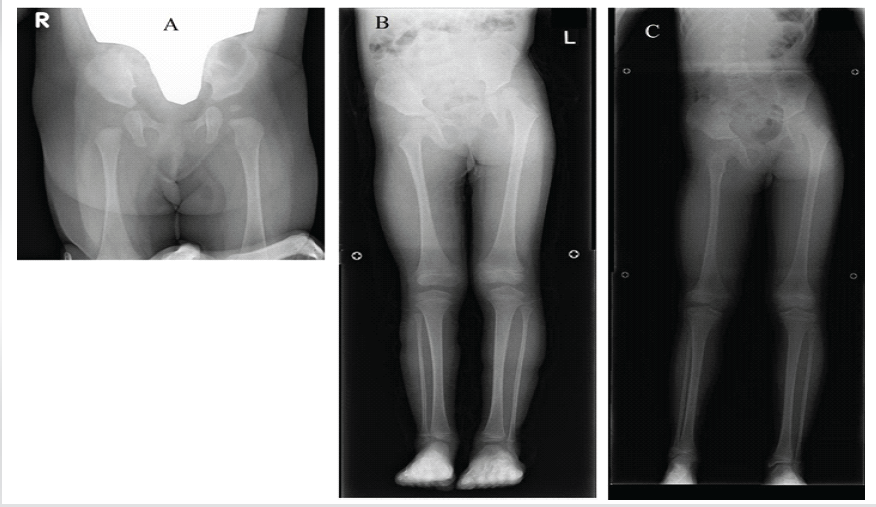
Figure 1: Radiographic findings prior to the first operation. Anteroposterior radiographs: (A) Pelvis and hips at age 4 months. (B) Lower limbs at age 3.0 years. (C) Lower limbs at age 8.0 years.
At the age of 8.0 years, her LLD had deteriorated to 5.6 cm and she manifested an obvious compensatory spinal curve (Fig. 1c). We calculated her predicted LLD at maturation using a Moseley straight line graph [3], which estimated an LLD of 10.5 cm. We elected to treat her LLD through a combination of femoral lengthening and contralateral epiphysiodesis, considering that the fragility of her femur would pose severe risks of both intra- and post-operative complications if we attempted excessive lengthening. We performed right femoral lengthening using the Limb Reconstruction System (Oxford Srl, Verona, Italy) and contralateral distal femoral epiphysiodesis using tension band plates (Fig. 2a and b).
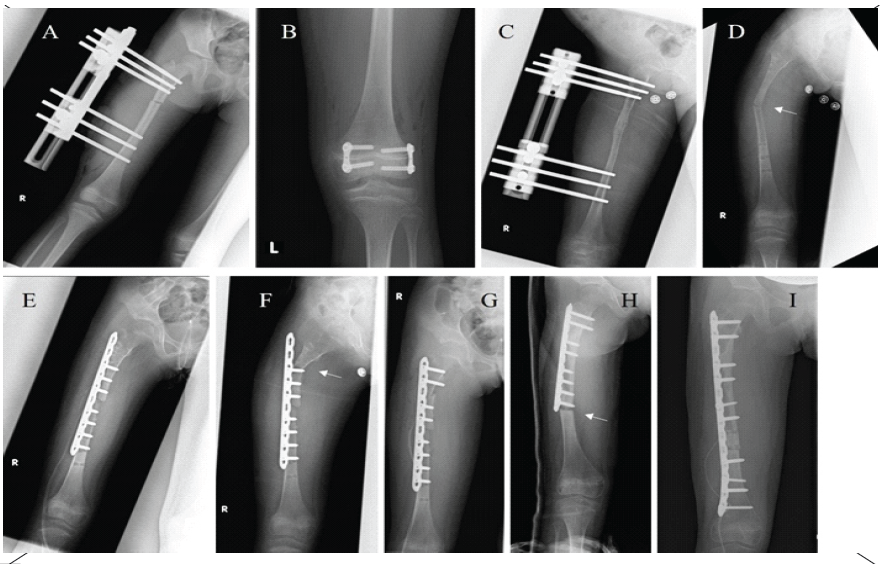
Figure 2: Radiographic treatment history. Anteroposterior radiographs: (A) External fixator (age 8.1 years). (B) Contralateral distal femoral epiphysiodesis (age 8.1 years). (C) Consolidation phase immediately prior to removal of hardware (age 8.6 years). (D) First fracture (age 8.6 years). (E) First osteosynthesis (age 8.6 years). (F) Second fracture (age 8.6 years). (G) Second osteosynthesis (age 8.6 years). (H) Third fracture (age 9.3 years). (I) Third osteosynthesis (age 9.3 years). Arrows indicate fractures.
Lengthening was initiated 1 week later, at a rate of 0.75 cm/day, obtaining 4.2 cm of lengthening over approximately 1.9 months. During the consolidation period, we ordered partial weight bearing. Eight months after the initial operation (Fig. 2c), we removed the external fixator. However, following removal, three additional osteosynthesis operations were needed in response to pathological fractures (Fig. 2d, e, f, g, h, I).
At the age of 11.0 years, because her fractured femur had obtained complete union, we decided to remove the plate system. We chose to insert a telescopic rod (diameter: 5 mm, length: 300 mm), which is a useful device in children with osteogenesis imperfecta (Fig. 3a and b), to reduce the risk of recurring fractures, increase bone strength and modulate her growth.
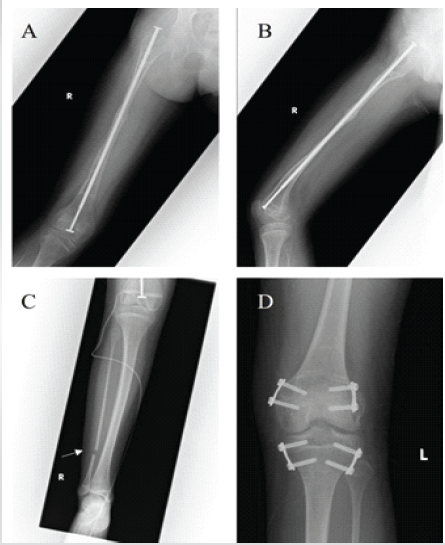
Figure 3: Treatment history following fracture healing. X-ray imaging at 11.0 years. (A) Right femur anteroposterior (AP) view after telescopic rod insertion. (B) Right femur lateral view. (C) Right lower leg AP view. Arrow indicates partial fibular resection. (D) Left knee AP view.
Intraoperatively, we confirmed that she had a hypoplastic right anterior cruciate ligament (data not shown), and we also decided to perform partial resection of the right fibula because it was hypoplastic, which might lead to tibia valgus (Fig. 3c). In addition, we replaced the tension band plates at the left distal femur and inserted new plates at the left proximal tibia (Fig. 3d). Examination at age 14.3 showed that the physes of her lower limbs had matured and had little expected remaining growth, so we removed the contralateral tension band plates. LLD at age 14.3 was estimated at 0.7 cm (Fig. 4).

Figure 4: Radiographic findings at latest follow-up. Anteroposterior radiograph of lower limbs at age 14.3 years.
Multiple instrumented 3DGA data were used to assess gait function both preoperatively and at the latest follow-up. We employed quantitative scoring systems, i.e., the gait deviation index (GDI) and the movement analysis profile (MAP), which includes the gait variable scores (GVS) and gait profile score (GPS) [4,5,6]. 3DGA data was collected using an MX-F 20 camera (Vicon, Oxford, UK) and two force plates (AMTI, Watertown, Massachusetts). Kinematic data were calculated using Plug-in Gait (Vicon, Oxford, UK). A score of 100 on the GDI indicates no pathological abnormalities. Every 10-point decrease below 100 indicates one standard deviation away from the reference data. The constituents of MAP are GVS and GPS, which were invented by Baker et al. [5] Both GVS and GPS are measured in degrees. Higher GVS and GPS indicate deterioration of motion at each joint and of gait in general. GVS is the root mean square difference of the individual’s kinematic data, consisting of nine kinematic parameters: pelvic tilt, pelvic obliquity, pelvic rotation, hip flexion, hip abduction, hip rotation, knee flexion, ankle dorsiflexion, and foot rotation. GPS is calculated as the root mean square average of GVS variables. Statistical analysis employed a paired t-test, performed using Statistical Package for Social Sciences (SPSS) ver. 24 for Windows (SPSS Inc., Armonk, New York). P < 0.05 was considered statistically significant.
The patient’s GPS was 20.4° at age 8.0 (Fig. 5). At the age of 14.3, GPS had improved to 7.9° (Fig. 6). The difference between the initial and latest GPS corresponded to 7.8 times the minimal clinically important difference (MCID) of 1.6° [6].
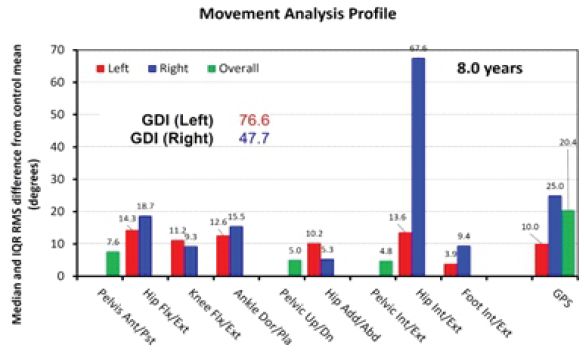
Figure 5: Movement analysis profile at 8.0 years. GDI: Gait deviation index; GPS: Gait profile score. A score of 100 on the GDI indicates no pathological abnormalities. Every 10-point decrease below 100 indicates one standard deviation away from the reference data. The constituents of the movement analysis profile are gait variable scores (GVS) and GPS. Both GVS and GPS are measured in degrees. Higher GVS and GPS indicate deterioration of motion at each joint, and of gait in general, respectively.
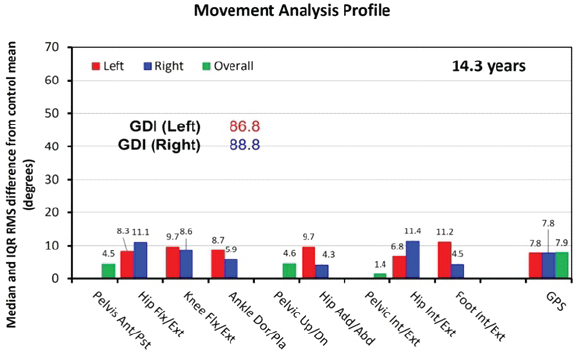
Figure 6: Movement analysis profile at 14.3 years. GDI: Gait deviation index. GPS: Gait profile score. A score of 100 on the GDI indicates no pathological abnormalities. Every 10-point decrease below 100 indicates one standard deviation away from the reference data. The constituents of the movement analysis profile are gait variable scores (GVS) and GPS. Both GVS and GPS are measured in degrees. Higher GVS and GPS indicate deterioration of motion at each joint, and of gait in general, respectively.
CSF is a rare congenital skeletal abnormality with several orthopedic manifestations, including coxa vara, abnormalities of the cruciate ligaments, hypoplasia of the lateral femoral condyle, fibular hemimelia, ball-in-socket ankle, and tarsal coalition [7,8,9,10]. We excluded the possibility of a tumor following extensive screenings. We based our diagnosis of CSF on imaging and physical findings, including ball-in-socket ankle, fibular hemimelia, and congenital LLD, as well as the intraoperative finding of hypoplasia of the anterior cruciate ligament, referring to previous reports [2,7,8,9,10].
The surgical options available for patients with LLD of 5–10 cm, as in the present case, include orthotic use, shortening, lengthening using either external fixation or intramedullary nailing, and epiphysiodesis [1,2]. There are several reports relating to patients with CSF who have undergone limb lengthening, with a particular focus on complications [8,9,10]. Aston et al. described outcomes among CSF patients who underwent lengthening using the Ilizarov technique. They recommended that lengthening should be limited to within 6 cm or 20% of the original femoral length, in order to reduce the risk of complications [9]. Hazra et al. reported a rare case of a patient who suffered from hip and knee dislocation during femoral lengthening [10]. Our assessment of the risk of complications was a key consideration in the process of surgical decision-making, due to the multi-joint involvement, including hip, knee, and ankle, present in this case. Therefore, we opted for a combination of lengthening on the involved side and epiphysiodesis on the contralateral side, with continuous physical therapy during hospitalization, in order to quickly achieve the patient’s treatment goals while minimizing the risk of complications.
We performed partial fibular resection to prevent subsequent tibia valgus and promote normal tibial growth. However, we are aware of no previous reports relating to fibular osteotomy as a means of treating fibular hemimelia or reducing the risk of subsequent tibia valgus. While our results cannot prove the effectiveness of this method, it did not lead to further deterioration of the tibial deformity in the present case.
Aiona et al. [11] evaluated gait patterns in patients with LLD, including CSF. They concluded that stress patterns due to compensatory reactions depend on the primary location of the shortening, with increased stress/loading on the ankles in cases of femoral shortening and increased pelvic obliquity in cases of tibial shortening. Because the femoral component of the patient’s LLD accounted for 75% of the total discrepancy, this case was classified as femoral shortening. Although preoperative ankle kinematic data did not support Aiona’s theory, ankle GVS showed statistically significant improvement, decreasing from 12.6/15.5° (left/right) to 8.7/5.9° (both P < 0.01). Correcting the patient’s LLD might lead to decreased compensatory reactions around the ankle.
Fujita et al. described 3DGA outcomes across several orthopedic surgeries in a patient with acquired LLD, concluding that despite improvement of LLD, gait eventually deviated from control, requiring several orthopedic surgeries [12]. In the present case, preoperative 3DGA revealed prominent ipsilateral hip rotation abnormality compared to other kinematic items, which are shown as GVS. The patient’s GPS were 25.0 (right), 10.0 (left), and 20.4° (overall), and this difference relating to asymmetry corresponded with 9.38 times the MCID (Fig. 4). In contrast, by age 14.3 years, GPS were 7.8 (right), 7.8 (left), and 7.9° (overall), showing that the asymmetry in GPS found preoperatively had been eliminated (Fig. 5). The surgical interventions had ameliorated her impaired gait function, suggesting the importance of correcting congenital LLD to within 1.0 cm.
This is the first report of a CSF patient who has undergone multiple corrective orthopedic surgeries with evaluation by 3DGA spanning a period of over 6 years. The observed post-operative improvement of gait function was likely influenced by a variety of factors, including the avoidance of long-term immobilization across the knee joint, predominantly femoral shortening rather than mixed tibial/femoral shortening, and lack of obvious contracture of the lower limb joints at the latest physical examination. Assessment of patients with LLD using a variety of modalities, including plain radiographs and quantitative gait parameters, can aid clinicians in the evaluation of gait abnormalities and accompanying compensatory reactions.
Patients with limb length discrepancies of over 2 cm always manifest some degree of gait abnormality. Orthopedic physicians treating these patients should pursue both numerical reduction in limb length discrepancy and quantitative improvement of gait function.
References
- 1. Herring JA, Cummings D. Tachdjian’s Pediatric Orthopaedics. 5th ed. Philadelphia, PA: Elsevier Saunders; 2013. p. 806-69. [Google Scholar] [PubMed]
- 2. Weinstein SL, Flynn JM, Crawford H, Noonan KJ, Halanski MA. Lovell and Winter’s Pediatric Orthopaedics. 8th ed. Philadelphia, PA: Wolters Kluwer; 2020. p. 1296-341. [Google Scholar] [PubMed]
- 3. Moseley CF. A straight-line graph for leg-length discrepancies. J Bone Joint Surg Am 1977;59:174-9. [Google Scholar] [PubMed]
- 4. Schwartz MH, Rozumalski A. The gait deviation index: A new comprehensive index of gait pathology. Gait Posture 2008;28:351-7. [Google Scholar] [PubMed]
- 5. Baker R, McGinley JL, Schwartz MH, Beynon S, Rozumalski A, Graham HK, et al. The gait profile score and movement analysis profile. Gait Posture 2009;30:265-9. [Google Scholar] [PubMed]
- 6. Baker R, McGinley JL, Schwartz M, Thomason P, Rodda J, Graham HK. The minimal clinically important difference for the gait profile score. Gait Posture 2012;35:612-5. [Google Scholar] [PubMed]
- 7. Johansson E, Aparisi T. Missing cruciate ligament in congenital short femur. J Bone Joint Surg 1983;65-A:1109-15. [Google Scholar] [PubMed]
- 8. Renzi-Brivio L, Lavini F, De Bastiani G. Lengthening in the congenital short femur. Clin Ortho Relat Res 1990;250:112-6. [Google Scholar] [PubMed]
- 9. Aston WJ, Calder PR, Baker D, Hartley J, Hill RA. Lengthening of the congenital short femur using the Ilizarov technique: A single-surgeon series. J Bone Joint Surg 2009;91:962-7. [Google Scholar] [PubMed]
- 10. Hazra S, Song HR, Jajodia N, Biswal S, Modi HN, Srinivasalu S. Hip and knee dislocation during femoral lengthening in congenital short femur: A rare case report. Arch Orthop Trauma Surg 2009;129:425-9. [Google Scholar] [PubMed]
- 11. Aiona M, Do KP, Emara K, Dorociak R, Pierce R. Gait patterns in children with limb length discrepancy. J Pediatr Orthop 2015;35:280-4. [Google Scholar] [PubMed]
- 12. Fujita H, Teramoto A, Fusagawa H, Yamashita T, Selber P. Three-dimensional gait analysis spanning 13 years in a patient with unilateral premature physeal arrest: A case report. Prog Rehabil Med 2023;8:1-7. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 The Importance of Closed Reduction and Internal Fixation done with Intramedullary Implants in Pathological Fractures – A Case Series
January 1, 2026 The Importance of Closed Reduction and Internal Fixation done with Intramedullary Implants in Pathological Fractures – A Case Series April 1, 2025 From Trivial Trauma to Major Surgery: Navigating Skeletal Metastases with Sequential Hip Arthroplasty for Pathological Femoral Neck Fractures in Triple-Negative Breast Cancer
April 1, 2025 From Trivial Trauma to Major Surgery: Navigating Skeletal Metastases with Sequential Hip Arthroplasty for Pathological Femoral Neck Fractures in Triple-Negative Breast Cancer October 1, 2025 Pediatric Patient with Septic Arthritis and Necrotising Fascitis: A Case Report
October 1, 2025 Pediatric Patient with Septic Arthritis and Necrotising Fascitis: A Case Report February 1, 2026 Conventional Total Knee Arthroplasty in Severe Anterolateral Femoral Bowing: Lateralized Femoral Entry Point to Approach Navigation Level Alignment – A Case Report
February 1, 2026 Conventional Total Knee Arthroplasty in Severe Anterolateral Femoral Bowing: Lateralized Femoral Entry Point to Approach Navigation Level Alignment – A Case Report