
Extensive Achilles tendon loss with associated skin defect can achieve acceptable functional recovery without formal reconstruction, underscoring the importance of individualized, context-based management.
Dr. Chester Ian F. Barroga, Department of Orthopaedics, Jose R. Reyes Memorial Medical Center, Manila, Philippines. E-mail: barrogaian0@gmail.com
Abstract
Introduction: The Achilles tendon, the strongest tendon in the body, is essential for plantar flexion and gait. Segmental tendon loss with soft-tissue defects is uncommon and difficult to manage, with most reported cases requiring complex reconstructions using tendon grafts or flaps. In contaminated or resource-limited settings, however, less invasive alternatives may still yield satisfactory outcomes.
Case Report: A 35-year-old male sustained an open calcaneal fracture with complete midsubstance Achilles tendon transection following a motor vehicle accident. Due to delayed presentation, contamination risk, and resource limitations, no tendon reconstruction was performed. The patient underwent serial debridement, immobilization in plantar flexion, and four cycles of negative pressure wound therapy using an improvised system. By 22 weeks, the wound was fully healed with soft-tissue coverage, and ultrasound confirmed tendon continuity through scar-mediated bridging. Functionally, he demonstrated 25° dorsiflexion, 45° plantarflexion, negative Matles and Thompson tests, and independent ambulation with minimal discomfort.
Discussion: This case demonstrates that segmental Achilles tendon defects may achieve functional recovery without formal reconstruction. Scar-mediated healing, supported by wound care and immobilization, provided continuity sufficient for ambulation and strength restoration. While technically demanding reconstructive methods remain the standard, this outcome highlights the potential of conservative management as a pragmatic alternative, particularly where infection, soft-tissue loss, or limited resources preclude surgery.
Conclusion: Conservative treatment of complex Achilles tendon injuries can restore both tendon integrity and function without reconstruction, underscoring its value as a viable option in carefully selected patients.
Keywords: Achilles tendon defect, open calcaneal fracture, tendon rupture, wound management, negative pressure wound therapy.
The Achilles tendon, the strongest tendon in the body, is vital for plantar flexion and gait, and its disruption often results in significant long-term functional limitations [1]. Achilles tendon ruptures (ATR) commonly occur in individuals aged 30–50 years [2]. When combined with soft-tissue defects, often from high-energy trauma or infection, these injuries present major reconstructive challenges given tendon loss, poor vascularity, and contamination risk, with reported cases describing technically demanding secondary procedures yielding good results [3,4,5]. One such case involved an infected ATR with an overlying soft-tissue defect that was successfully managed with debridement and an anterolateral thigh free flap, simultaneously addressing both tendon integrity and soft-tissue coverage [3].
Contaminated open Achilles tendon injuries have been managed with extensive debridement, direct repair or use of the proximal tendon segment, and soft-tissue coverage using reverse sural artery flaps, achieving good outcomes including return to normal gait and tiptoe standing within months [6]. Other techniques involving vascularized or free flaps have been reported to provide coverage alongside tendon reconstruction [7,8]. Although effective, these methods are technically demanding, resource-intensive, and carry risks such as infection, flap failure, and prolonged hospitalization [9]. In low-resource settings, alternative strategies may be necessary.
We present a case of segmental Achilles tendon loss with overlying skin defects managed without formal reconstruction or flap coverage, instead utilizing serial debridement, immobilization, and modified negative pressure wound therapy (NPWT). This approach underscores the potential for functional recovery through less invasive means, consistent with reports that satisfactory outcomes may be achieved even without tendon reconstruction in complex or infected cases [10,11], where merely filling the tendon gap and ensuring reliable soft-tissue cover can still yield favorable results.
A 35-year-old male, non-smoker, presented 17 days after a motor vehicle accident with an open calcaneal fracture initially managed at another hospital by multiple debridements and K-wire fixation. Due to financial constraints, he transferred to our institution for continued wound care. Examination revealed a posterior heel wound with granulation tissue overlying an avulsed area and necrotic skin inferior to the calcaneal region. A 3 cm dorso-plantar avulsion flap was noted on the posterior heel with visible retained K-wires (Fig. 1).

Figure 1: Gross image of the wound on presentation at our emergency room (17 days post-injury); avulsed wound at the posterior ankle with exposed transected Achilles tendon. X-ray radiographs after initial debridement and pinning done at previous institution showing a comminuted calcaneal fracture.
Plantar flexion strength was absent on resisted testing. Peripheral pulses were palpable with no signs of neurovascular compromise. There was no evidence of systemic infection. Both Matles and Thompson tests were positive, indicating loss of Achilles tendon continuity. Radiographs showed a comminuted calcaneal fracture fixed with retained K-wires (Fig. 2).

Figure 2: Gross and follow-up X-ray images at 22 weeks post-operation after removal of pin.
The patient was started on broad-spectrum antibiotics and subsequently underwent extensive debridement with K-wire revision. Findings included minimal purulent discharge, non-viable soft tissue, and complete mid-substance Achilles tendon transection approximately 3 cm from its calcaneal insertion. Given resource limitations, a modified NPWT system was assembled using sterile gauze, an incise drape, a size 14 nasogastric tube, and a standard hospital suction machine as a cost-effective alternative to commercial devices. Intermittent suction at – 125 mmHg (2 h on, 2 h off) was applied, with dressing changes every 5 days. During hospitalization, the patient underwent five serial debridements with four cycles of NPWT. After each debridement, an anterior blocking splint was applied for immobilization. By hospital day 36, the wound demonstrated healthy granulation tissue, infection markers normalized, and cultures were negative. Despite a persistent 3 cm tendon gap, no reconstructive procedure was undertaken. The patient was discharged for outpatient follow-up and rehabilitation.
Segmental ATR with calcaneal involvement is rare and poses major challenges due to tendon loss, soft-tissue disruption, and high risk of contamination and infection [12]. These difficulties are compounded by the tendon’s poor vascularity, particularly in the mid-portion “watershed zone” prone to ischemia and impaired healing [13]. Deep infection after reconstruction is a serious complication with no standardized guidelines, making traditional repair high-risk in such cases.
Traditional management of segmental Achilles tendon defects usually involves primary repair or reconstruction with tendon grafts combined with soft-tissue coverage using local or free flaps to restore continuity [1]. Composite grafts that include both tendon and soft tissue have also been reported with success [5,8]. However, these procedures are technically demanding, resource-intensive, and carry risks such as infection, wound dehiscence, and iatrogenic nerve injury, especially when tendon margins are devitalized or contaminated [10]. Deep infection after reconstruction also remains a difficult complication without standardized protocols [14]. In contrast, recent reports suggest that acceptable functional outcomes may still be achieved without tendon reconstruction, using soft-tissue cover alone in selected post-infective or contaminated cases [5,11]. This non-reconstructive approach may shorten operative time, reduce morbidity, and avoid the risks associated with staged reconstructions.
In selected cases, functional recovery without tendon reconstruction has been documented. A report described management of segmental Achilles tendon loss using a free gracilis muscle flap solely for soft-tissue coverage, without tendon grafting [5]. Over time, the flap remodeled and functionally bridged the tendon gap, consistent with the principle that muscle can adapt to act as a tendon substitute. At 2-year follow-up, dynamic ultrasound showed flap shortening during resisted plantarflexion with continuity from the gastro-soleus to the calcaneus, while magnetic resonance imaging demonstrated fatty transformation without a cleavage plane between flap and native tendon [5]. These findings highlight that with adequate healing and coverage, good functional outcomes may be achieved even without formal reconstruction [11].
The use of NPWT has been reported to stimulate granulation tissue formation capable of bridging Achilles tendon defects. One case achieved closure of an infected tendon gap without flap or graft reconstruction [15], while another showed its effectiveness in complex posterior heel injuries with exposed tendon and calcaneus, where it reduced healing time and the need for extensive reconstruction [16]. In the present case, NPWT combined with immobilization was initially applied to control contamination and manage exudates. Over four cycles in 3 months, the wound progressively filled with granulation tissue, the defect decreased in size, and complete soft-tissue coverage was achieved without the need for reconstruction. By 5 months, the patient regained independent ambulation with 25° dorsiflexion, 45° plantarflexion, negative Thompson and Matles tests, and only mild stiffness. The likely mechanism involves subatmospheric pressure enhancing local perfusion, reducing edema, and stimulating fibroblast activity, thereby promoting scar-mediated bridging across tendon gaps and supporting functional recovery [17,18]. (Fig. 3). Immobilization in plantarflexion likely contributed to stabilizing the repair, and our improvised NPWT system, assembled from hospital suction equipment, sterile gauze, and a nasogastric tube, provided a practical low-cost alternative to commercial devices. Consistent with existing literature [10,11,15,16,17], this case suggests that with meticulous wound care, NPWT can serve not only as an adjunct but, in select situations, as a definitive strategy for segmental ATR. A major limitation in our case was the absence of a structured rehabilitation program due to irregular follow-up. While the patient achieved near-normal ambulation, targeted physical therapy may have further improved outcomes. Future cases would benefit from an integrated rehabilitation protocol focused on gait retraining, calf strengthening, proprioception, and graded weight-bearing. In addition, long-term durability of scar-mediated tendon healing remains uncertain, especially under high-load conditions. (Fig. 4).
Our case illustrates that conservative management of segmental Achilles tendon loss, when combined with effective wound care and immobilization, can result in favorable outcomes even without primary tendon reconstruction. In select patients, particularly in the presence of infection, soft-tissue loss, or limited resources, modified NPWT may serve as both a bridge and a substitute for invasive reconstructive strategies. The main advantages of this approach include reduced technical demands, lower infection risk, cost-effectiveness, and the ability to achieve wound healing and restored tendon continuity without the need for grafts or soft-tissue flaps. However, literature reflects the absence of a standardized algorithm for these injuries [14]. There is no established consensus on whether to prioritize immediate reconstruction, delayed repair, or a conservative approach, making clinical decisions highly case dependent. In our case, the patient’s return to ambulation, restoration of functional ankle motion, and negative clinical tests for rupture suggest that conservative management is a safe and effective alternative most especially when surgical intervention is not feasible.

Figure 3: Matles and Thompson tests at 22 weeks post-operation.
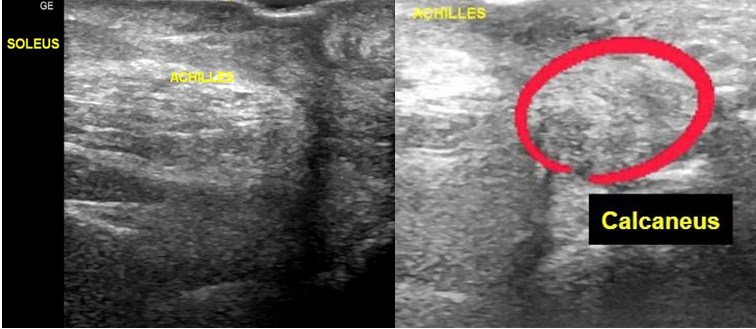
Figure 4: Ultrasound of the posterior ankle at 22 weeks post-operation with noted increased echogenicity of adjacent soft tissues (in red circle).
The patient demonstrated progressive and satisfactory wound and functional recovery over the course of follow-up. By 8–10 weeks, the wound showed marked reduction in size with healthy granulation tissue, absence of purulence, and complete coverage of deeper structures, allowing discontinuation of NPWT and transition to conventional dressings. Clinical improvement was accompanied by tolerable pain levels, negative Thompson testing, and initiation of passive range-of-motion exercises, indicating early restoration of Achilles tendon continuity despite the absence of formal reconstruction. At 22 weeks, definitive healing was achieved. The wound was fully epithelialized with durable soft-tissue coverage and no signs of ongoing infection. Radiographic evaluation demonstrated callus formation with preserved fracture alignment, consistent with progressive osseous healing. Functional assessment revealed recovery of ankle motion (25° dorsiflexion and 45° plantarflexion) with residual stiffness but adequate strength for independent ambulation. Negative Matles and Thompson tests, together with ultrasound findings of an intact Achilles tendon and soleus muscle, confirmed tendon continuity, albeit with distal fibrosis and poor echogenicity consistent with scar-mediated healing. Overall, this case illustrates that in selected high-risk situations, a conservative and staged approach utilizing NPWT and immobilization can result in successful wound closure, tendon continuity through biological bridging, and acceptable functional outcomes without formal Achilles tendon reconstruction.
This report suggests that not all segmental Achilles tendon losses require immediate reconstructive surgery. In carefully selected patients, structured wound care, immobilization, and NPWT can achieve tendon continuity and functional ambulation, expanding non-reconstructive treatment as a practical alternative when infection risk or limited resources make surgery unfavorable.
References
- 1. Park SH, Lee HS, Young KW, Seo SG. Treatment of acute achilles tendon rupture. Clin Orthop Surg 2020;12:1-8. [Google Scholar] [PubMed]
- 2. Park HG, Youn D, Baik JM, Hwang JH. Epidemiology of achilles tendon rupture in south korea: Claims data of the national health insurance service from 2009 to 2017. Clin Orthop Surg 2021;13:539-48. [Google Scholar] [PubMed]
- 3. Lee YK, Lee M. Treatment of infected Achilles tendinitis and overlying soft tissue defect using an anterolateral thigh free flap in an elderly patient: A case report. Medicine (Baltimore) 2018;97:e11995. [Google Scholar] [PubMed]
- 4. Liang Yii RS, Chai SC, Zainal HM, Basiron N. Single-stage reconstruction of a traumatic tendocutaneous defect of the Achilles using free composite anterolateral thigh flap with vascularized fascia lata. Jt Dis Relat Surg 2022;33:673-9. [Google Scholar] [PubMed]
- 5. Sabapathy SR, Venkataramani H, Latheef L, Bhardwaj P. Reconstruction of segmental defects of Achilles tendon: Is it a must in infected complex defects? Indian J Plast Surg 2013;46:121-3. [Google Scholar] [PubMed]
- 6. Jepegnanam TS, Nithyananth M, Boopalan PR, Cherian VM, Titus VT. Reconstruction of open contaminated achilles tendon injuries with soft tissue loss. J Trauma 2009;66:774-9. [Google Scholar] [PubMed]
- 7. Bullocks JM, Hickey RM, Basu CB, Hollier LH, Kim JY. Single-stage reconstruction of Achilles tendon injuries and distal lower extremity soft tissue defects with the reverse sural fasciocutaneous flap. J Plast Reconstr Aesthet Surg 2008;61:566-72. [Google Scholar] [PubMed]
- 8. Mao J, Xiang Y, Chu H, Jin G, Su G, Liu CZ, et al. Comparison of long-term ankle joint function after one-stage and staged microsurgical repair of open achilles tendon defects. J Orthop Surg Res 2025;20:149. [Google Scholar] [PubMed]
- 9. Lee JW, Yu JC, Shieh SJ, Liu C, Pai JJ. Reconstruction of the Achilles tendon and overlying soft tissue using antero-lateral thigh free flap. Br J Plast Surg 2000;53:574-7. [Google Scholar] [PubMed]
- 10. Lee HJ, Kim JW, Oh CW, Min WK, Shon OJ, Oh JK, et al. Negative pressure wound therapy for soft tissue injuries around the foot and ankle. J Orthop Surg Res 2009;4:14. [Google Scholar] [PubMed]
- 11. Saunders DE, Hochberg J, Wittenborn W. Treatment of total loss of the Achilles tendon by skin flap cover without tendon repair. Plast Reconstr Surg 1978;62:708-12. [Google Scholar] [PubMed]
- 12. Mukherjee S, Banerjee K. A segmental rupture of achilles tendon, its management, and outcome – a rare case report. J Orthop Case Rep 2023;13:53-7. [Google Scholar] [PubMed]
- 13. Fenech M, Ajjikuttira A, Edwards H. Ultrasound assessment of acute Achilles tendon rupture and measurement of the tendon gap. Australas J Ultrasound Med 2024;27:106-19. [Google Scholar] [PubMed]
- 14. Bowers MW, Turner NS, Ryssman DB, Moran SL. Outcomes following treatment of the infected achilles tendon. Foot Ankle Orthop 2019;4:2473011419846943 . [Google Scholar] [PubMed]
- 15. Saku I, Kanda S, Saito T, Fukushima T, Akiyama T. Wound management with negative pressure wound therapy in postoperative infection after open reconstruction of chronic Achilles tendon rupture. Int J Surg Case Rep 2017;37:106-8. [Google Scholar] [PubMed]
- 16. Vaseenon T, Somsuk W. Negative pressure wound therapy for traumatic foot and ankle wound: Two case reports and review of the literature. J Med Assoc Thai 2015;98:111-6. [Google Scholar] [PubMed]
- 17. Kunze KN, Hamid KS, Lee S, Halvorson JJ, Earhart JS, Bohl DD. Negative-pressure wound therapy in foot and ankle surgery. Foot Ankle Int 2020;41:364-72. [Google Scholar] [PubMed]
- 18. Mosser P, Kelm J, Anagnostakos K. Negative pressure wound therapy in the management of late deep infections after open reconstruction of achilles tendon rupture. J Foot Ankle Surg 2015;54:2-6. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report
June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report January 1, 2026 Comparison of Indigenous Low Cost Vacuum-Assisted Closure Therapy and Standard Wound Therapy in Open Fractures: A Randomized Controlled Trial
January 1, 2026 Comparison of Indigenous Low Cost Vacuum-Assisted Closure Therapy and Standard Wound Therapy in Open Fractures: A Randomized Controlled Trial August 1, 2025 Flexor Pollicis Longus Tendon Rupture after Distal Radius Volar Plating and Reconstruction with Interpositional Palmaris Tendon Graft: A Case Report
August 1, 2025 Flexor Pollicis Longus Tendon Rupture after Distal Radius Volar Plating and Reconstruction with Interpositional Palmaris Tendon Graft: A Case Report October 1, 2024 The effectiveness of negative pressure wound therapy in enhancing skin graft uptake on a burned lower leg stump: A case report
October 1, 2024 The effectiveness of negative pressure wound therapy in enhancing skin graft uptake on a burned lower leg stump: A case report