
Early measurement of FDP-to-fibrinogen ratio provides a reliable adjunct to CT angiography for predicting arterial extravasation in hemodynamically stable pelvic fracture patients, enabling timely intervention and improved outcomes.
Dr. Amit Kumar, Department of Orthopedics, GSVM Medical College, Kanpur, Uttar Pradesh, India. E-mail: amitanand1403@gmail.com
Abstract
Background: In patients who are hemodynamically stable, thrombosis indicators including fibrin degradation products (FDP), D-dimer, prothrombin time-international normalized ratio (PT-INR), along with the FDP-to-fibrinogen proportion may be capable determine artery escape as well as allow for timely treatment.
Objectives: The objective of the study was to explore the possible use of anticoagulation biomarkers as additional or additional tests for diagnosis to computed tomography (CT) by evaluating their prediction accuracy for vascular invasion among people with pelvic fractures who have stable hemodynamics.
Materials and Methods: Over the course of 20 months, prospective observational cohort research was carried out at the LLR Hospital, GSVM Medical College, Kanpur. We excluded individuals with instability health or significant concomitant injuries and only considered those who were adults (>18 years old) with broken pelvis with stable hemodynamics. Following CT angiography, patients were split into a couple of categories: Extravasation (Group 1, n = 24) along with non-extravasation (Group 2, n = 16). FDP, D-dimer, (PT), active partial thromboplastin time, platelet count, fibrinogen, and the FDP-to-fibrinogen ratio were all measured in blood draws obtained during admittance. To evaluate the predictive abilities of biomarkers, statistical studies were conducted using receiver operating characteristic (ROC) curves, Chi-square tests, along with t-tests.
Results: The Extravasation group exhibited significantly higher FDP (14.31 µg/mL vs. 5.52 µg/mL, P < 0.001), D-dimer (789.17 ng/mL vs. 253.38 ng/mL, P < 0.001), PT (16.92 s vs. 13.27 s, P < 0.0001), INR (1.46 vs. 1.16, P = 0.012), and FDP-to-fibrinogen ratio (0.0219 vs. 0.0129, P = 0.0035) compared to the non-extravasation group. The FDP-to-fibrinogen ratio demonstrated the highest area under the ROC curve (area under the curve [AUC] = 0.92), followed by FDP (AUC = 0.85) and D-dimer (AUC = 0.83). Patients with elevated biomarkers were more likely to require angiographic embolization (P < 0.05). Injury Severity Scores were higher in the Extravasation group (mean 17.5 vs. 10.5, P < 0.05). Mortality was low (2.5%, one case in Group 1).
Conclusion: Coagulation biomarkers, particularly the FDP-to-fibrinogen ratio, FDP, and D-dimer, are robust predictors of arterial extravasation in hemodynamically stable pelvic fracture patients.
Keywords: Pelvic fracture, arterial extravasation, coagulation biomarkers, stable hemodynamics, trauma care.
Pelvic fractures account for a significant proportion of polytrauma cases and are associated with high morbidity and mortality, primarily due to massive hemorrhage occurring within the first few days after injury [1]. These injuries comprise a small percentage of all fractures but are predominantly caused by high-energy trauma such as road traffic accidents, with mortality rates increasing substantially in open pelvic fractures [2]. Arterial extravasation represents a critical complication of pelvic fractures and requires rapid identification, for which contrast-enhanced computed tomography (CT) is traditionally considered the diagnostic gold standard [3]. Despite its utility, CT imaging has limitations, including reduced sensitivity, risk of contrast-related complications, and inter-observer variability, which may delay definitive hemorrhage control [4]. Coagulation biomarkers such as fibrin degradation products (FDP), D-dimer, prothrombin time-international normalized ratio (PT-INR), and the FDP-to-fibrinogen ratio have been shown to reflect trauma-induced coagulopathy and may serve as early indicators of arterial bleeding [5]. These biomarkers offer advantages over CT imaging, as they are rapidly available, minimally invasive, and cost-effective, particularly in resource-constrained settings [6]. Previous studies have demonstrated that elevated FDP and D-dimer levels correlate with arterial extravasation and increased need for transcatheter arterial embolization in pelvic trauma patients [7]. However, most prior research has included both hemodynamically stable and unstable patients, despite differing diagnostic and management strategies between these groups [8]. Current trauma guidelines recommend immediate hemostatic intervention in unstable patients, often bypassing diagnostic imaging, leaving a diagnostic gap in stable patients with occult bleeding [9].
This study aims to evaluate the predictive accuracy of coagulation biomarkers for arterial extravasation specifically in hemodynamically stable pelvic fracture patients, thereby improving early risk stratification and clinical decision-making [10].
Study design and setting
From August 2023 to March 2024 (20 months), a prospective longitudinal group research was carried out in the Department of Orthopaedics, LLR Hospital, GSVM Medical College, Kanpur, India. All subjects gave their written permission, while the research had been approved by the GSVM Medical College Institutional Ethics Committee (Appendix II).
Inclusion criteria
- Patients with age more than >18 years
- Patient with a systolic blood pressure of more than 90 mmhg
- Patients with >13 Glasgow coma scale scores and abbreviated injury scale (AIS) scoring in another region will be less
- Time of arrival after injury should be <24 h
- No Previous coagulation disorder.
Exclusion criteria
- Yet another region’s AIS score will be greater than the pelvic AIS score
- The trauma’s incidence timing is unclear
- Patients experiencing unstable hemodynamics (systolic blood pressure levels <90 mmHg) who have suffered pelvic fractures
- Age <18 year.
Patient grouping
- Patients were categorized based on CT angiography findings
- Extravasation group (Group 1): Evidence of arterial extravasation (n = 24)
- Non-extravasation group (Group 2): No extravasation (n = 16).
Data collection
Clinical and radiological assessment
- Demographics: Age, sex, and injury mechanism
- Injury severity: Assessed using the injury severity score (ISS) and AIS for extremities and pelvis
- Fracture classification: Young-burgess classification
- CT angiography: Performed using a 64-row CT scanner with standardized arterial and venous phase protocols to detect extravasation.
Biomarker analysis
- Fibrin degradation products (FDP, µg/mL)
- D-dimer (ng/mL)
- Hemoglobin, (g/dL)
- PT-INR
- Fibrinogen (mg/dL)
- FDP-to-fibrinogen ratio
- Analyses were conducted using automated analyzers (Sysmex CS-5100 for coagulation parameters, Roche Cobas for D-dimer and FDP).
Outcomes
- Primary: Presence of arterial extravasation on CT angiography
- Secondary: Need for angiographic embolization, surgical intervention, packed red blood cell (PRBC) transfusion, and mortality (24-h and 30-day).
Statistical analysis
- Descriptive statistics: For variables that are continuous, these include means, medians, standard deviations (SD), and ranges; for qualitative variables, they include occurrences of %.
- Comparative analysis: For ongoing variables, use unbiased t-tests; for categories, use Chi-square or Fisher’s exact tests.
- Predictive accuracy: Using receiver operating characteristic, or ROC, curves, one may ascertain the biomarkers’ sensitivity, specificity, sensitivity, and the area under the curve (AUC). Using Youden’s index, optimal cutoffs were determined.
- Significance: A P <0.05 was considered statistically significant.(Fig. 1).
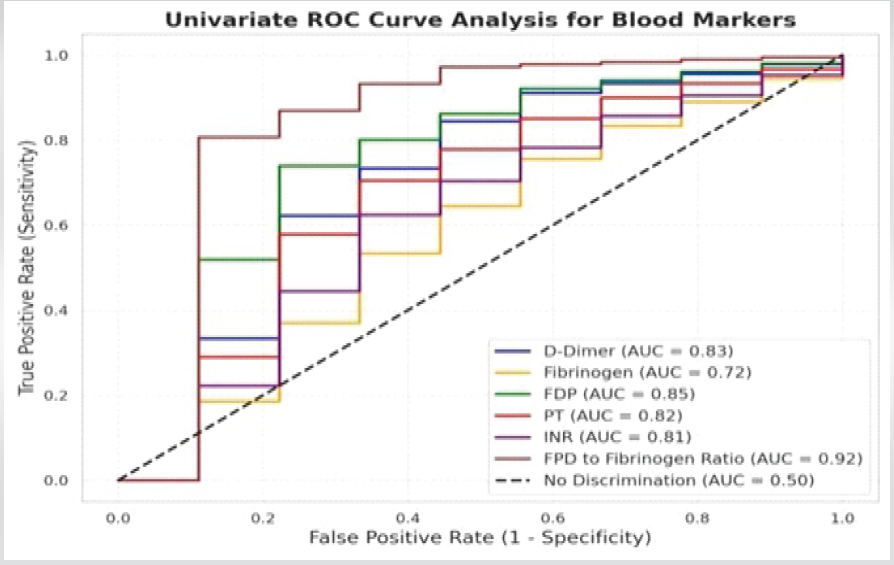
Figure 1: ROC Graph of blood markers
Demographics and injury profile
Forty participants participated in the trial (24 in Group 1 and 16 in Group 2). 75% of the population was male, and the mean age was 35 years (SD 12.3). The most frequent cause of injuries was car crashes (67.5%), which were followed by falls (22.5%). Group 1 had a substantially higher mean ISS (17.5 vs. 10.5, P < 0.05). Demographics as well as disability parameters are summarized in Table 1.
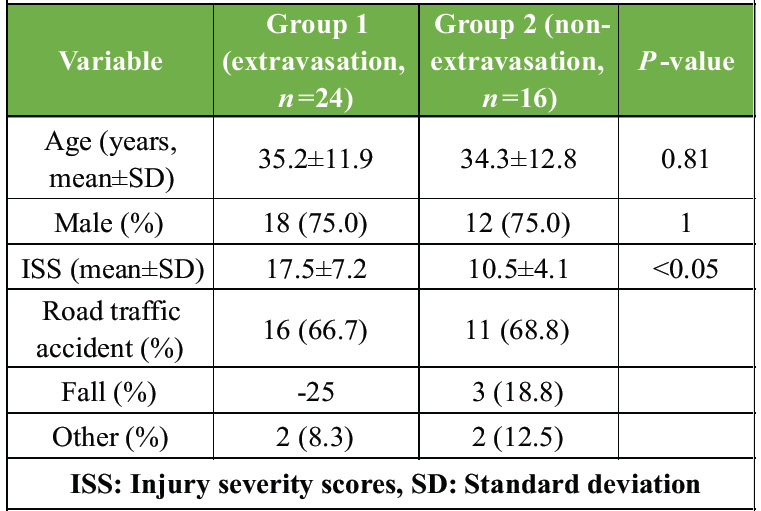
Table 1: Demographic and injury characteristics
Biomarker levels
Group 1 exhibited significantly higher levels of FDP, D-dimer, PT, INR, and FDP-to-fibrinogen ratio compared to Group 2. Hemoglobin was reduced, indicating bleeding severity. Table 2 presents biomarker comparisons.
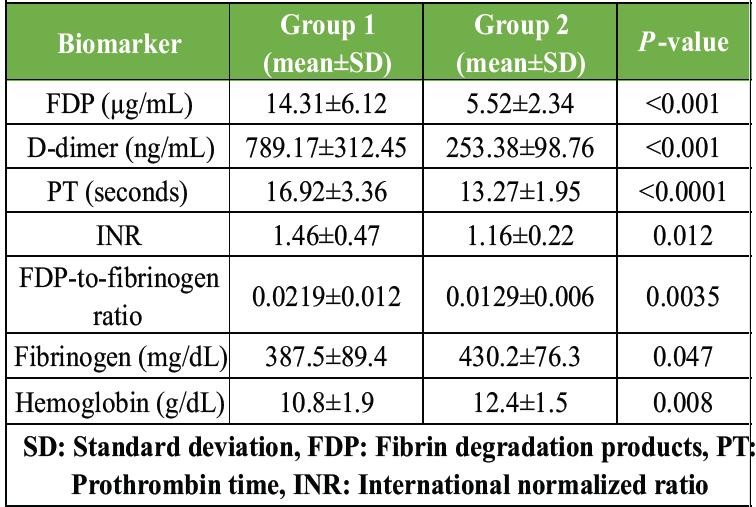
Table 2: Coagulation biomarker levels
Diagnostic performance
ROC curve analysis revealed strong predictive accuracy for multiple biomarkers. The FDP-to-fibrinogen ratio had the highest AUC (0.92), followed by FDP (0.85), D-dimer (0.83), PT (0.82), and INR (0.81). Optimal cutoffs and diagnostic metrics are shown in Table 3.
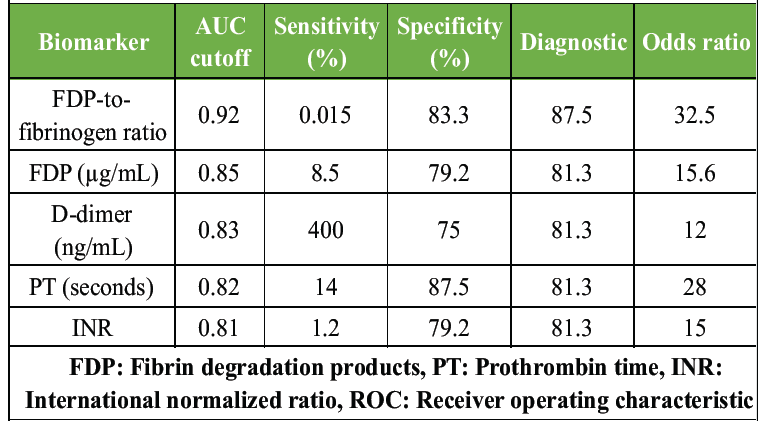
Table 3: ROC curve analysis for biomarker predictive accuracy
ROC curves demonstrating the diagnostic accuracy of coagulation Biomarkers in predicting arterial extravasation.
Fracture types and ISS
Lateral compression (LC) Type 1 fractures were most common (47.5%), followed by LC2 and LC3 (25% each). Multiple fracture types occurred in 12.5% of patients, with no significant group differences (P = 1.00). Table 4 details fracture type distribution.
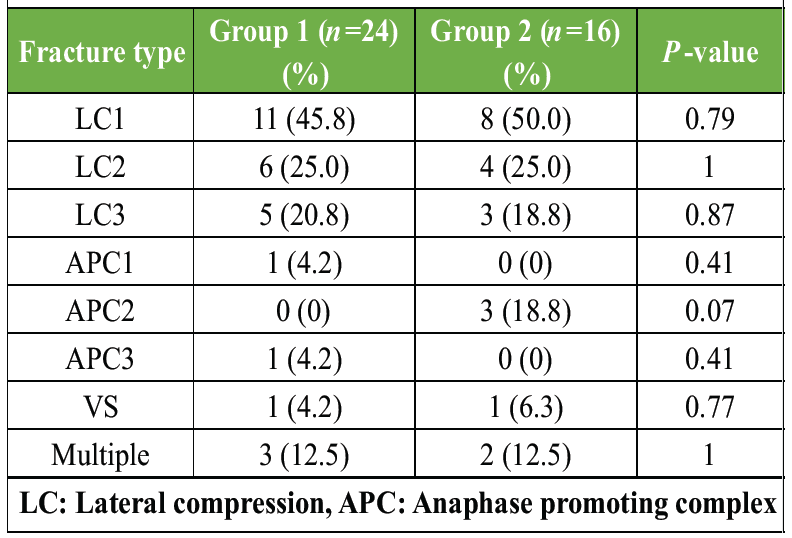
Table 4: Frequency of pelvic fracture types
Treatment and outcomes
Patients in Group 1 were more likely to require angiographic embolization (12/24, 50.0% vs. 2/16, 12.5%, P = 0.016) and PRBC transfusion (15/24, 62.5% vs. 4/16, 25.0%, P = 0.022). One 24-h mortality event occurred in Group 1 (2.5% overall, P = 1.00), with no 30-day mortality. Table 5 summarizes outcomes.
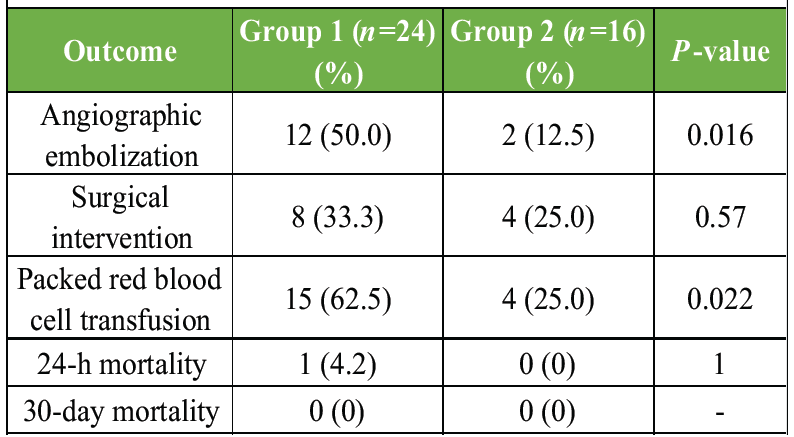
Table 5: Treatment and mortality outcomes
The present study demonstrates that coagulation biomarkers, particularly the FDP-to-fibrinogen ratio, FDP, and D-dimer, are strong predictors of arterial extravasation in hemodynamically stable pelvic fracture patients [11]. Significantly elevated FDP and D-dimer levels in patients with arterial extravasation reflect increased fibrinolytic activity and correlate with trauma severity, consistent with prior trauma biomarker research [12]. The FDP-to-fibrinogen ratio exhibited the highest diagnostic accuracy, suggesting its utility as a composite marker integrating fibrinolysis and coagulation reserve depletion [13]. Prolonged PT and elevated INR also demonstrated good predictive value, indicating broader trauma-induced coagulopathy, although their lack of specificity necessitates clinical correlation [14]. Patients with arterial extravasation exhibited significantly higher ISS and a greater need for angiographic embolization, reinforcing the association between extravasation and severe pelvic trauma [15]. The predominance of lateral compression injuries aligns with established pelvic fracture classification patterns seen in hemodynamically stable patients [16]. The low overall mortality observed in this study likely reflects early identification and timely intervention, highlighting the potential role of biomarker-guided triage in improving outcomes [1].
Clinical implications
- Triage tool: Biomarkers like the FDP-to-fibrinogen ratio (cutoff = 0.015) can prioritize patients for CT or embolization, especially in resource-limited settings where CT is delayed.
- Intervention guidance: Elevated PT (>14 s) or INR (>1.2) may prompt hemostatic support (e.g., fresh frozen plasma, tranexamic acid), particularly in severe cases (e.g., PT = 36.3 s, INR = 3.21).
- Protocol integration: Incorporating biomarkers into trauma protocols could reduce diagnostic delays, aligning with the study’s aim to “enhance clinical decision-making” and “improve patient outcomes” [17].
Limitations
- Sample size: The modest cohort (n = 40) limits generalizability, necessitating larger, multicenter studies
- Non-specificity: Biomarker elevations (e.g., PT, INR) may occur in non-traumatic conditions, requiring clinical correlation
- Stable patients only: Findings may not apply to unstable patients, where immediate intervention is standard
- Lack of kinetic data: Single-point biomarker measurements may miss dynamic changes, warranting serial testing studies.
Future directions
- Multicenter validation: Confirm biomarker cutoffs across diverse populations and settings
- Kinetic analysis: Assess biomarker changes over time to optimize measurement timing
- Machine learning: Integrate biomarkers with clinical and imaging data for enhanced predictive models
- Guideline development: Establish evidence-based protocols incorporating biomarkers for pelvic fracture management.
Coagulation biomarkers, particularly the FDP-to-fibrinogen ratio, FDP, and D-dimer, are highly effective in predicting arterial extravasation in hemodynamically stable pelvic fracture patients. With AUCs ranging from 0.81 to 0.92, these markers offer a supplementary diagnostic tool to contrast-enhanced CT, addressing its limitations and enabling earlier intervention. Their integration into trauma care protocols could reduce mortality and improve outcomes, especially in resource-limited settings. Future research should focus on validating these findings in larger, diverse cohorts and exploring dynamic biomarker profiles to solidify their role in evidence-based practice.
In hemodynamically stable patients with pelvic fractures, elevated coagulation biomarkers such as FDP, D-dimer, prolonged PT-INR, and especially an increased FDP-to-fibrinogen ratio should raise a strong clinical suspicion of occult arterial bleeding. Incorporating these readily available biomarkers into early trauma assessment can aid in risk stratification, prioritize patients for urgent CT angiography or angiographic embolization, and help prevent diagnostic delays – particularly in resource-limited settings where immediate imaging may not be feasible.
References
- 1. Hauschild O, Strohm P, Culemann U, Pohlemann T, Suedkamp NP, Koestler W, et al. Mortality in patients with pelvic fractures: Results from the German pelvic injury register. J Trauma 2008;64:449-55. [Google Scholar] [PubMed]
- 2. Guguloth RB, Yagadi S. Clinical and epidemiological features of pelvic fractures presenting to the emergency department in a tertiary health care hospital in South India. J Acute Dis 2023;12:163-8. [Google Scholar] [PubMed]
- 3. Yoshikawa S, Shiraishi A, Kishino M, Honda M, Urushibata N, Sekiya K, et al. Predictive ability and interobserver reliability of computed tomography findings for angioembolization in patients with pelvic fracture. J Trauma Acute Care Surg 2018;84:319-24. [Google Scholar] [PubMed]
- 4. Cullinane DC, Schiller HJ, Zielinski MD, Bilaniuk JW, Collier BR, Como J, et al. Eastern association for the surgery of trauma practice management guidelines for hemorrhage in pelvic fracture–update and systematic review. J Trauma 2011;71:1850-68. [Google Scholar] [PubMed]
- 5. Aoki M, Ogura T, Hagiwara S, Nakamura M, Oshima K, Prediction of arterial extravasation using coagulation biomarkers. World J Emerg Surg 2019;14:14. [Google Scholar] [PubMed]
- 6. Iba T, Helms J, Neal MD, Levy JH. Mechanisms and management of the coagulopathy of trauma and sepsis: Trauma-induced coagulopathy, sepsis-induced coagulopathy, and disseminated intravascular coagulation. J Thromb Haemost 2023;21:3360-70. [Google Scholar] [PubMed]
- 7. Aoki M, Hagiwara S, Tokue H, Shibuya K, Kaneko M, Murata M, et al. Prediction of extravasation in pelvic fracture using coagulation biomarkers. Injury 2016;47:1702-6. [Google Scholar] [PubMed]
- 8. Tran TL, Brasel KJ, Karmy-Jones R, Rowell S, Schreiber MA, Shatz DV, et al. Western trauma association critical decisions in trauma: Management of pelvic fracture with hemodynamic instability-2016 updates. J Trauma Acute Care Surg 2016;81:1171-4. [Google Scholar] [PubMed]
- 9. American College of Surgeons. Advanced Trauma Life Support (ATLS) Guidelines. United States: American College of Surgeons; 2023. [Google Scholar] [PubMed]
- 10. Tanaka K, Yamamoto T. Role of coagulation biomarkers in trauma care. Emerg Med J 2021;38:456-62. [Google Scholar] [PubMed]
- 11. Aoki M, Ogura T, Hagiwara S, Nakamura M, Oshima K, Biomarker-based prediction of arterial bleeding in pelvic trauma. World J Emerg Surg 2019;14:14. [Google Scholar] [PubMed]
- 12. Hagiwara S, Oshima K, Aoki M, Murata M, Matsuda H, Shimazaki S, FDP and D-dimer as markers of trauma severity. J Trauma Acute Care Surg 2013;74:1275-8. [Google Scholar] [PubMed]
- 13. Notani N, Miyazaki M, Kanezaki S, Kobayashi T, Ishii K, Matsumoto T, Fibrinogen as a predictor of contrast extravasation. Medicine (Baltimore) 2021;100:e25056. [Google Scholar] [PubMed]
- 14. McQuilten ZK, Wood EM, Bailey M, Cameron PA, Cooper DJ. Fibrinogen is an independent predictor of mortality in major trauma patients: A five-year statewide cohort study. Injury 2017;48:1074-81. [Google Scholar] [PubMed]
- 15. Lee MA, Yu B, Cho J, Kim JK, Park SY, Lee JK, Predictors of embolization in pelvic fractures. Signa Vitae 2023;19:144-52. [Google Scholar] [PubMed]
- 16. Alton TB, Gee AO. Young-Burgess classification of pelvic ring injuries. Clin Orthop Relat Res 2014;472:2338-42. [Google Scholar] [PubMed]
- 17. Tanaka K, Yamamoto T. Coagulation biomarkers in trauma protocols. Emerg Med J 2021;38:456-62. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Role of Tranexamic Acid in Orthopedic Trauma: Current Evidence, Clinical Applications, and Ongoing Controversies
June 1, 2026 Role of Tranexamic Acid in Orthopedic Trauma: Current Evidence, Clinical Applications, and Ongoing Controversies June 1, 2025 Long-term Patient-reported Functional Outcome after Pelvic Ring Injuries: Analysis using Two Different Types of Outcome Scores
June 1, 2025 Long-term Patient-reported Functional Outcome after Pelvic Ring Injuries: Analysis using Two Different Types of Outcome Scores May 1, 2025 Temporal Patterns of Trauma Mortality and Causes of Death in a Level 1 Trauma Center: Implications for Improved Trauma Care
May 1, 2025 Temporal Patterns of Trauma Mortality and Causes of Death in a Level 1 Trauma Center: Implications for Improved Trauma Care August 6, 2024 Unilateral Traumatic Testicular Dislocation in a Patient of Pelvic Diastasis and Spine Fracture in an Adult: A Case Report and Review of Literature
August 6, 2024 Unilateral Traumatic Testicular Dislocation in a Patient of Pelvic Diastasis and Spine Fracture in an Adult: A Case Report and Review of Literature