
Intraoperative ropivacaine-clonidine infiltration at the hamstring donor site and intra-articullarly significantly reduces immediate post-operative pain, facilitating early mobilization and accelerated functional recovery – outcomes central to successful orthopedic management of knee arthroscopy.
Dr. Sukesh Rao Sankineani, Department of Orthopaedics, Yashoda Hospital, Secunderabad, Telangana, India. E-mail: sukeshrao.sankineni@gmail.com
Abstract
Introduction: Internal derangement of the knee (IDK) is among the most common musculoskeletal conditions managed in orthopedic practice, with knee arthroscopy serving as the gold standard for its surgical treatment. Despite the minimally invasive nature of the procedure, post-operative pain remains a significant barrier to early rehabilitation and functional recovery. This study evaluated whether intraoperative infiltration of a local anesthetic cocktail at the hamstring donor site and intra-articullarly offers superior immediate post-operative pain control compared to regional spinal anesthesia alone.
Materials and Methods: This prospective, double-blinded, and randomized controlled study was conducted at the Department of Orthopaedics, Yashoda Hospital, Secunderabad, over 1 year. Sixty patients with IDK undergoing arthroscopic surgery were randomly allocated into two groups of 30 each. Group-A received intraoperative infiltration of 0.2% ropivacaine (25 mL) with 0.2% clonidine at the donor hamstring site and intra-articullarly in addition to regional spinal anesthesia, while Group-B received regional spinal anesthesia alone. Post-operative pain was assessed using the Visual Analogue Scale (VAS) in the immediate post-operative period. Statistical analysis was performed using Statistical Package for the Social Sciences version 20, with P < 0.05 considered significant.
Results: Both groups were comparable in terms of age (mean 31.3 ± 8.54 vs. 32.73 ± 7.65 years; P = 0.5) and sex distribution (P = 0.75). Road traffic accidents constituted the most frequent mechanism of injury in both groups. Immediate post-operative VAS scores were significantly lower in Group-A compared to Group-B (mean 0.53 ± 1.04 vs. 4.67 ± 1.84; P < 0.001), with 76.67% of Group-A patients reporting a complete absence of pain.
Conclusion: Intraoperative infiltration of ropivacaine and clonidine at the hamstring donor site and intra-articullarly provides significantly superior immediate post-operative pain relief compared to spinal anesthesia alone, facilitating early mobilization and improved orthopedic recovery following knee arthroscopy.
Keywords: Internal derangement of knee, knee arthroscopy, post-operative analgesia, visual analogue scale, hamstring donor site.
Internal derangement of the knee (IDK) represents one of the most frequently encountered musculoskeletal conditions in orthopedic practice, encompassing a heterogeneous group of intra-articular pathologies including meniscal tears, ligamentous injuries, and chondral lesions [1]. The condition predominantly affects young, physically active individuals and carries significant functional morbidity if left untreated, often resulting in progressive joint deterioration, impaired mobility, and diminished quality of life. The orthopedic management of IDK has been fundamentally transformed by the advent of knee arthroscopy, which has emerged as the gold standard surgical modality for both definitive diagnosis and targeted therapeutic intervention, offering superior visualization of intra-articular structures with minimal soft-tissue disruption compared to open surgical approaches [2].
Despite the minimally invasive nature of knee arthroscopy, post-operative pain remains a substantive clinical challenge that directly impacts the orthopedic outcomes of the procedure. Inadequately controlled post-operative pain delays early joint mobilization, impairs participation in post-operative physiotherapy, prolongs hospital stay, and ultimately compromises the functional recovery that arthroscopic intervention is intended to achieve [3]. In procedures involving hamstring tendon harvest, the donor site constitutes a distinct and often underappreciated source of post-operative pain that compounds the intra-articular pain burden and further hinders rehabilitation. Cai et al., in a randomized controlled trial, demonstrated that local infiltration analgesia at the hamstring donor site effectively reduced early post-operative pain and opioid consumption following arthroscopic hamstring tendon autograft reconstruction, without adversely affecting short-term functional outcomes, thereby establishing donor site pain as a distinct and targetable pain generator in the orthopedic context [4].
From an orthopedic analgesia standpoint, the optimization of post-operative is not merely a comfort measure but a functional imperative. Conventional systemic analgesics, including opioids and non-steroidal anti-inflammatory drugs, while effective in isolation, carry risks of systemic side effects that can interfere with early post-operative rehabilitation and delay discharge, thereby limiting their utility as standalone analgesic strategies in the orthopedic setting [5]. These limitations have driven the evolution of targeted intraoperative local infiltration analgesia as a technique that delivers effective, site-specific pain control without the burden of systemic adverse effects, thereby creating conditions more conducive to early mobilization and accelerated orthopedic recovery.
Ropivacaine, a long-acting amino-amide local anesthetic with a well-established safety profile, has been studied extensively in knee arthroscopy. Zhou et al., in a systematic review and meta-analysis, confirmed that single-dose ropivacaine administration significantly reduced post-operative pain scores in arthroscopic knee surgery without increasing the risk of adverse effects, supporting its use as a safe and effective component of multimodal analgesia in the orthopedic context [3]. The analgesic efficacy of ropivacaine is further augmented by clonidine, a selective alpha-2 adrenoceptor agonist that reduces afferent nociceptive transmission and prolongs local anesthetic action through local vasoconstriction, thereby extending the duration of effective pain relief into the critical early post-operative and rehabilitation window [6]. Thamrongskulsiri et al. described an intraoperative anesthetic cocktail infiltration technique at the hamstring donor site in arthroscopic knee surgery, reporting its reproducibility and effectiveness in addressing donor site pain as a targeted component of perioperative orthopedic pain management [7].
Notwithstanding the growing body of evidence supporting local infiltration analgesia, comparative data evaluating the intraoperative infiltration of a ropivacaine-clonidine cocktail at the hamstring donor site against regional spinal anesthesia alone, specifically in the context of post-operative orthopedic outcomes in knee arthroscopy, remain limited in the Indian literature. This study was therefore conducted to bridge this gap by comparing the immediate post-operative analgesic efficacy of these two strategies, with the primary objective of identifying the approach most conducive to improved functional recovery and patient outcomes in orthopedic arthroscopic practice.
Study design and setting
This was a prospective, double-blinded, randomized controlled study conducted among patients diagnosed with IDK who underwent knee arthroscopy. The study was carried out in the Department of Orthopaedics at Yashoda Hospital, Secunderabad, over a period of 1 year.
Ethical considerations
The study was conducted in strict accordance with the ethical principles outlined in the Declaration of Helsinki and the guidelines set forth by the Indian Council of Medical Research for biomedical research involving human participants. Before commencement of the study, ethical clearance was obtained from the Institutional Ethics Committee, bearing approval number DNBT/30/2024, dated July 09th, 2024. Written informed consent was obtained from all participating patients in both English and the local language, ensuring that each participant was fully apprised of the nature, purpose, potential risks, and benefits of the study before enrollment. Participation was entirely voluntary, and patients retained the right to withdraw from the study at any point without any compromise to their clinical care. Patient confidentiality and data anonymity were strictly maintained throughout the study period. The double-blind design was upheld to minimize bias while ensuring patient safety was not compromised at any stage of the investigation.
Patient selection
Patients aged 18 years and above who were clinically diagnosed with IDK and who provided willingness to participate were considered eligible for enrollment. Patients below 18 years of age, those presenting with open injuries, and those unwilling to undergo surgical intervention were excluded from the study. All eligible participants were enrolled following the acquisition of written informed consent in both English and the local language prior to any study-related procedures.
Randomization and sample size
A total of 60 patients fulfilling the eligibility criteria were enrolled and randomly allocated into two equal groups of 30 patients each – Group-A and Group-B – using computer-generated random sequences to ensure allocation concealment and minimize selection bias. The sample size was calculated based on detecting a clinically meaningful difference in post-operative Visual Analogue Scale (VAS) scores between the two groups. Assuming a mean difference of 2 units in VAS score, with a standard deviation of 2, a power of 80%, and a two-sided alpha error of 5%, the minimum required sample size was calculated to be 27 patients per group. To account for potential dropouts, 30 patients were included in each group, resulting in a total sample size of 60 participants.
Intervention protocol
Group A received an intraoperative local anesthetic cocktail comprising 0.2% ropivacaine (25 mL) combined with clonidine, administered at the hamstring donor site, in addition to regional (spinal) anesthesia. The infiltration was performed under aseptic conditions at the end of graft harvest, with the solution injected in a fan-shaped manner into the peri-tendinous and subcutaneous tissues around the donor site using a sterile syringe and needle, ensuring uniform distribution of the anesthetic along the harvest tract.
Group B received regional (spinal) anesthesia alone, without any supplementary local infiltration. To maintain the double-blind design, both the patients and the outcome assessor were kept unaware of the treatment allocation. The intervention was performed by the operating surgeon as per the randomization protocol (Figure 1).
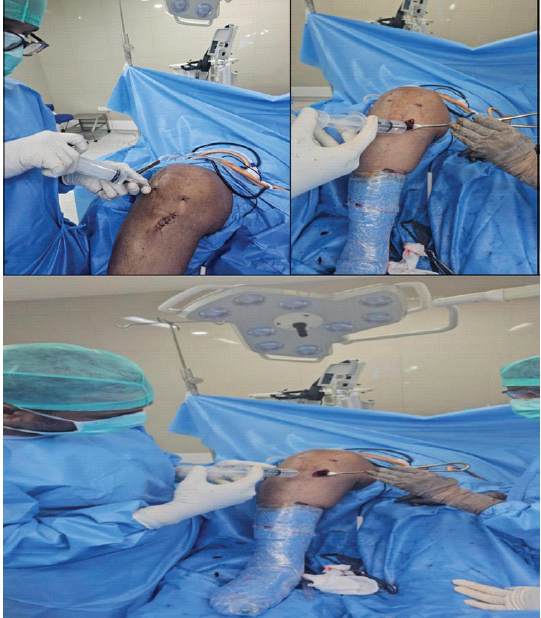 Figure 1: Operative procedure images.
Figure 1: Operative procedure images.
Outcome assessment
Post-operative pain was the primary outcome measure and was evaluated using the VAS, a validated and widely used 10-point numeric tool on which a score of 0 represents complete absence of pain, and 10 represents the worst imaginable pain. Assessment was performed in the immediate post-operative period by the blinded assessor.
Participant flow
A total of 60 patients assessed for eligibility were enrolled in the study and randomized into two groups of 30 each. All randomized patients received the allocated intervention. There were no losses to follow-up or exclusions after randomization. All 60 patients were included in the final analysis. The participant flow through each stage of the trial is illustrated in the CONSORT flow diagram below (Figure 2).
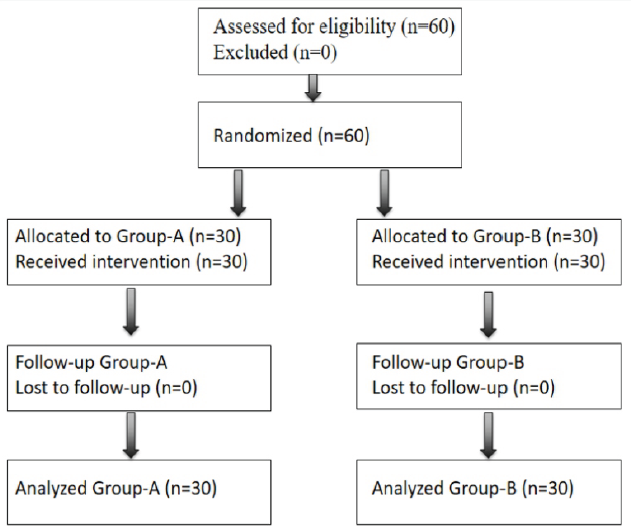
Figure 2: CONSORT diagram.
Statistical analysis
All demographic details, injury characteristics, and clinical findings were recorded in a structured case sheet. Categorical variables were summarized as frequencies and percentages, and comparisons between groups were performed using the Pearson Chi-square test for independence of attributes. Continuous variables were expressed as mean ± standard deviation and were compared between the two groups using the independent samples t-test. Statistical analysis was performed using the Statistical Package for the Social Sciences software, version 20. A two-tailed alpha level of 5% was set as the threshold for statistical significance, whereby any P < 0.05 was considered statistically significant.
As presented in Table 1, the demographic characteristics of both groups were comparable at baseline.
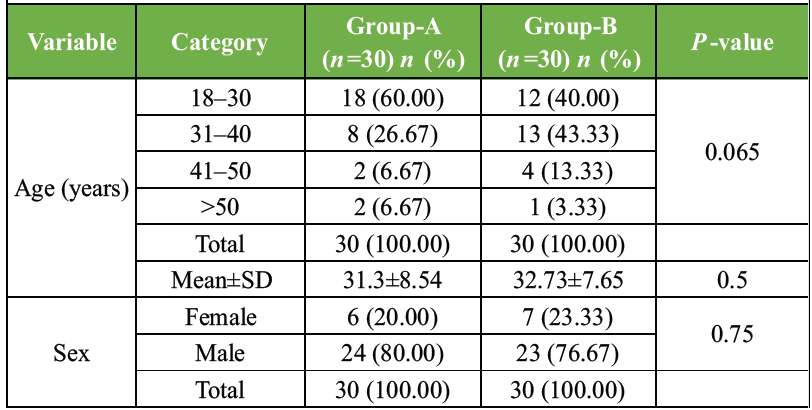 Table 1: Demographic distribution of patients in both groups
Table 1: Demographic distribution of patients in both groups
The majority of patients in both groups fell within the 18–30 year age bracket, reflecting the relatively younger demographic typically associated with knee injuries requiring arthroscopic intervention. The mean ages of Group-A and Group-B were closely matched, and no statistically significant difference was observed between the two groups with respect to age distribution (P = 0.5). Similarly, both groups were predominantly male, and the sex distribution between the two groups showed no statistically significant difference (P = 0.75). The homogeneity of both groups across these baseline variables confirmed that any subsequent differences in outcome measures could be attributed to the intervention rather than demographic confounders.
The distribution of injury mechanisms across both groups is detailed in Table 2.
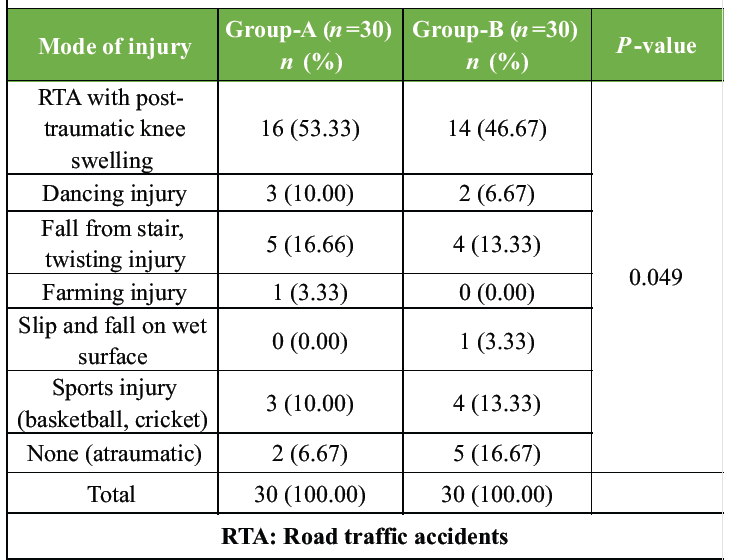 Table 2: Distribution according to mode of injury in both groups
Table 2: Distribution according to mode of injury in both groups
Road traffic accidents (RTA) presenting with post-traumatic knee swelling constituted the most frequent cause of IDK in both groups, followed by fall from stairs with twisting injury and sports-related injuries. A small proportion of patients in both groups reported atraumatic onset. While the overall distribution of injury modes reached statistical significance (P = 0.049), the pattern of injury types was broadly similar across both groups, and this difference is unlikely to have materially influenced the post-operative outcomes assessed in this study.
The comparison of immediate post-operative pain scores between the two groups, as outlined in Table 3, revealed a clinically and statistically compelling difference in favor of Group-A.
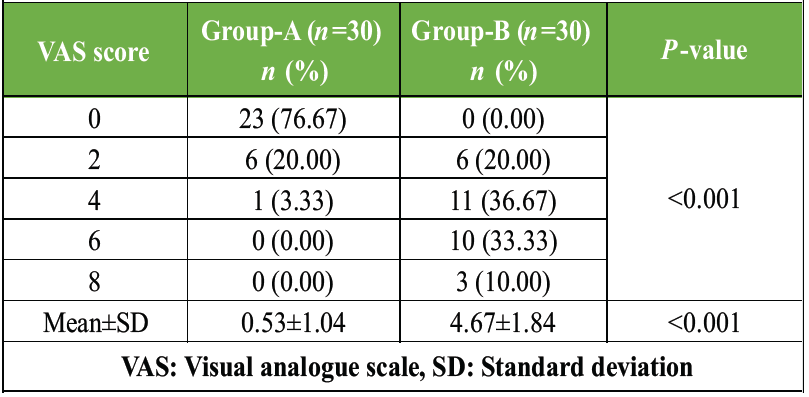 Table 3: Comparison of post-operative pain using VAS score in the immediate post-operative period between group-A and group-B
Table 3: Comparison of post-operative pain using VAS score in the immediate post-operative period between group-A and group-B
The vast majority of patients in Group-A reported a complete absence of pain in the immediate post-operative period, whereas all patients in Group-B experienced varying degrees of pain, with a considerable proportion reporting moderate to severe pain scores. The difference in mean VAS scores between the two groups was highly significant (P < 0.001), clearly establishing the superiority of the intraoperative local anesthetic cocktail administered in Group-A over regional anesthesia alone in Group-B for immediate post-operative pain control following knee arthroscopy.
The orthopedic management of IDK through arthroscopic intervention has evolved significantly over the past two decades, establishing knee arthroscopy as an indispensable tool in the orthopedic surgeon’s armamentarium. However, the surgical success of arthroscopic knee procedures is inextricably linked to the quality of perioperative pain management, since inadequately controlled post-operative pain directly impairs the patient’s ability to participate in early rehabilitation, delays functional recovery, and ultimately compromises the orthopedic outcomes that the procedure is designed to achieve. The demographic profile of patients enrolled in this study – predominantly young males in their early thirties sustaining knee injuries through RTA and physical activity – mirrors the population most functionally dependent on successful orthopedic recovery, lending particular clinical weight to the analgesic outcomes observed.
The primary orthopedic finding of this study is that intraoperative infiltration of a ropivacaine-clonidine cocktail at the hamstring donor site, as an adjunct to spinal anesthesia, delivers dramatically superior immediate post-operative pain control compared to spinal anesthesia alone, with a mean VAS score of 0.53 ± 1.04 in Group-A versus 4.67 ± 1.84 in Group-B (P < 0.001). In orthopedic surgical practice, the immediate post-operative period is the most critical analgesic window, as pain intensity during this phase directly governs the patient’s tolerance for early joint mobilization exercises, which are foundational to restoring knee function, preventing stiffness, and optimizing the long-term outcome of arthroscopic intervention. The VAS, as the most widely validated and responsive instrument for quantifying post-operative pain in orthopedic surgical research, confirmed this difference with a level of statistical significance that leaves no ambiguity regarding the clinical superiority of the Group-A approach [8].
From a purely orthopedic functional recovery perspective, the near-complete abolition of immediate post-operative pain in Group-A patients carries implications that extend well beyond mere comfort. Effective analgesia in the early post-operative phase enables earlier initiation of physiotherapy, facilitates quicker return of quadriceps activation, promotes earlier weight-bearing, and reduces the risk of post-operative joint stiffness – all of which are recognized determinants of both short-term and long-term functional outcomes following knee arthroscopy. Karpetas et al., in a multicenter comparative study of analgesic strategies following knee surgery, demonstrated that patients managed with targeted local analgesic infiltration achieved earlier post-operative mobilization milestones compared to those receiving epidural or nerve block-based analgesia alone, directly affirming the orthopedic rehabilitation advantage conferred by site-specific analgesic techniques of the kind employed in Group-A of the present study [9].
The pharmacological basis of the superior orthopedic analgesic outcomes in Group-A lies in the complementary mechanisms of ropivacaine and clonidine. Ropivacaine, a long-acting amino-amide local anesthetic, exerts its effect through sodium channel blockade at the infiltration site, producing reliable and sustained sensory blockade with a well-established safety profile in orthopedic settings. Singh et al. confirmed in a randomized controlled trial that periarticular ropivacaine-based cocktail infiltration in knee surgery produced excellent pain control in the immediate post-operative period, with patients in the infiltration group demonstrating significantly lower pain scores and reduced analgesic requirements compared to controls, consistent with the findings of the present study [10]. Clonidine, as an alpha-2 adrenoceptor agonist adjuvant, synergistically enhances and prolongs the local analgesic effect of ropivacaine by attenuating afferent nociceptive transmission and retarding systemic drug absorption through local vasoconstriction at the donor site, thereby extending meaningful analgesic coverage into the early rehabilitation window. Suresh et al. confirmed that clonidine as an adjuvant to ropivacaine in the context of knee surgery significantly prolonged the duration of post-operative sensory blockade and reduced supplementary analgesic requirements, providing pharmacological support for the analgesic architecture underpinning the Group-A protocol [11].
The orthopedic significance of minimizing post-operative opioid dependence in this patient population cannot be overstated. The young, active demographic that predominantly sustains IDK and undergoes arthroscopic intervention is precisely the group most at risk from opioid-related adverse effects that impair early rehabilitation, including sedation, nausea, and delayed return of neuromuscular coordination. Day and Boryan, in a contemporary evidence-based review of pain management strategies following arthroscopic and knee preservation surgery, emphasized that multimodal analgesic regimens incorporating local anesthetic infiltration have demonstrated consistent success in reducing post-operative opioid requirements while maintaining superior pain control, enabling the early functional recovery milestones that define successful orthopedic outcomes in this setting [12]. The near-complete pain scores in Group-A patients suggest that the ropivacaine-clonidine donor site cocktail may function effectively as an opioid-sparing cornerstone within such multimodal orthopedic analgesia frameworks. This is further supported by Passias et al., [13] and Pedersen et al., who reported that targeted perioperative local analgesic interventions in knee surgery patients resulted in meaningful reductions in post-operative opioid consumption, with direct positive implications for rehabilitation trajectory and patient satisfaction [14].
The findings of this study carry a clear practical message for orthopedic surgical practice: the addition of an intraoperative local anesthetic cocktail infiltration at the hamstring donor site is a technically simple, reproducible, and low-risk modification to the standard arthroscopic knee surgery protocol that yields disproportionately significant analgesic and functional recovery benefits. Lu et al. demonstrated that combining site-specific local infiltration analgesia with regional anesthesia in knee arthroscopy patients significantly reduced post-operative pain scores and analgesic consumption compared to regional anesthesia alone, a finding that directly parallels the results of the present study and reinforces the orthopedic rationale for integrating donor site infiltration into routine arthroscopic practice [8].
The limitations of this study include its single-center design, modest sample size, and restriction of pain assessment to the immediate post-operative period. Longer-term orthopedic outcome data – encompassing range of motion recovery, time to full weight-bearing, return to occupational and sporting activity, and patient-reported functional scores – would further delineate the complete orthopedic benefit of this analgesic strategy. Larger multicentric randomized trials with extended follow-up are warranted to consolidate these findings and guide formal incorporation of this technique into standard perioperative orthopedic protocols for knee arthroscopy.
Effective post-operative pain management is central to functional recovery following knee arthroscopy. Intraoperative infiltration of 0.2% ropivacaine and 0.2% clonidine at the donor hamstring site, as an adjunct to regional spinal anesthesia, delivers superior immediate post-operative pain control over spinal anesthesia alone, with significantly lower VAS scores in Group-A confirming its clinical efficacy. This technique reduces early pain burden, facilitates earlier mobilization, and improves patient outcomes in orthopedic practice. It merits adoption as a routine component of perioperative protocol in knee arthroscopy.
Post-operative pain control is a critical determinant of rehabilitation success following knee arthroscopy, and the hamstring donor site represents a distinct and targetable pain generator that is frequently overlooked in routine orthopedic perioperative protocols. Intraoperative infiltration of 0.2% ropivacaine and 0.2% clonidine at the donor hamstring site, as an adjunct to regional spinal anesthesia, produces markedly superior immediate post-operative analgesia compared to spinal anesthesia alone, with the majority of patients reporting a complete absence of pain, thereby creating optimal conditions for early joint mobilization and accelerated functional recovery. This simple, reproducible, and easily integrated technique carries a strong clinical case for adoption as a standard component of perioperative pain management in arthroscopic knee surgery, with direct positive implications for orthopedic patient outcomes.
References
- 1. Bushnell BD, Sakryd G, Noonan TJ. Hamstring donor-site block: Evaluation of pain control after anterior cruciate ligament reconstruction. Arthroscopy 2010;26:894-900. [Google Scholar] [PubMed]
- 2. Kristensen PK, Pfeiffer-Jensen M, Storm JO, Thillemann TM. Local infiltration analgesia is comparable to femoral nerve block after anterior cruciate ligament reconstruction with hamstring tendon graft: A randomised controlled trial. Knee Surg Sports Traumatol Arthrosc 2014;22:317-23. [Google Scholar] [PubMed]
- 3. Zhou Y, Yang TB, Wei J, Zeng C, Li H, Yang T, et al. Single-dose intra-articular ropivacaine after arthroscopic knee surgery decreases post-operative pain without increasing side effects: A systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc 2016;24:1651-9. [Google Scholar] [PubMed]
- 4. Cai Z, Yang Y, Liu D, Lu W, Pan L, He M, et al. The effect of hamstring donor-site block for functional outcomes and rehabilitation after anterior cruciate ligament reconstruction. Front Surg 2023;10:1003022. [Google Scholar] [PubMed]
- 5. Pöpping DM, Elia N, Marret E, Wenk M, Tramèr MR. Clonidine as an adjuvant to local anesthetics for peripheral nerve and plexus blocks: A meta-analysis of randomized trials. Anesthesiology 2009;111:406-15. [Google Scholar] [PubMed]
- 6. Sun R, Zhao W, Hao Q, Tian H, Tian J, Li L, et al. Intra-articular clonidine for post-operative analgesia following arthroscopic knee surgery: A systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc 2014;22:2076-84. [Google Scholar] [PubMed]
- 7. Thamrongskulsiri N, Chancharoenchai P, Limskul D, Itthipanichpong T, Tanpowpong T. A technique for hamstring donor-site injection with anesthetic cocktail in remnant-preserving anterior cruciate ligament reconstruction. Arthrosc Tech 2023;13:102818. [Google Scholar] [PubMed]
- 8. Hou X, Luo Z, Wang H, Zhan Y, Yang L, Li L. Effect of adductor canal block combined with local infiltration anesthesia on rehabilitation of primary total knee arthroplasty. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2018;32:1006-11. [Google Scholar] [PubMed]
- 9. Karpetas GZ, Spyraki MK, Giakoumakis SI, Fligou FG, Megas PD, Voyagis GS, et al. Multimodal analgesia protocol for pain management after total knee arthroplasty: Comparison of three different regional analgesic techniques. J Musculoskelet Neuronal Interact 2021;21:104-12. [Google Scholar] [PubMed]
- 10. Singh H, Agarwal KK, Tyagi S, Makadia P, Oza B, Jain P, et al. Peroperative intra-articular infiltration of tranexamic acid and ropivacaine cocktail in patients undergoing total knee arthroplasty: A randomized controlled trial. Cureus 2022;14:e23091. [Google Scholar] [PubMed]
- 11. Suresh A, Fultambkar G, Vijayanand B, Nair A. A prospective, randomized controlled, double-blinded study comparing dexmedetomidine and clonidine as an adjuvant to ropivacaine in femoral nerve block for postoperative analgesia in patients undergoing total knee arthroplasty. Ain-Shams J Anesthesiol 2021;13:44. [Google Scholar] [PubMed]
- 12. Day MS, Boryan A. Current evidence-based approaches to multimodal pain control and opioid minimization after arthroscopic and knee preservation surgery. J Am Acad Orthop Surg 2024;32:e24-32. [Google Scholar] [PubMed]
- 13. Passias BJ, Johnson DB, Schuette HB, Secic M, Heilbronner B, Hyland SJ, et al. Preemptive multimodal analgesia and post-operative pain outcomes in total hip and total knee arthroplasty. Arch Orthop Trauma Surg 2023;143:2401-7. [Google Scholar] [PubMed]
- 14. Pedersen C, Vilhelmsen FJ, Laigaard J, Mathiesen O, Karlsen AP. Opioid consumption and non-opioid multimodal analgesic treatment in pain management trials after hip and knee arthroplasties: A meta-epidemiological study. Acta Anaesthesiol Scand 2023;67:613-20. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Evaluation of Post-operative Analgesic Efficacy of Adductor Canal Block Compared to Conventional Intravenous Analgesics in Knee Arthroscopy Surgery
January 1, 2026 Evaluation of Post-operative Analgesic Efficacy of Adductor Canal Block Compared to Conventional Intravenous Analgesics in Knee Arthroscopy Surgery July 1, 2026 All-Inside Versus Inside-Out Meniscal Repair: A Comparative Study of Healing Rates And Functional Outcomes
July 1, 2026 All-Inside Versus Inside-Out Meniscal Repair: A Comparative Study of Healing Rates And Functional Outcomes June 1, 2026 A Comparative Study between Local Infiltration of Ropivacaine Cocktail and Post-operative Epidural Bupivacaine in Post-operative Analgesia in Primary Total Knee Arthroplasty
June 1, 2026 A Comparative Study between Local Infiltration of Ropivacaine Cocktail and Post-operative Epidural Bupivacaine in Post-operative Analgesia in Primary Total Knee Arthroplasty June 1, 2026 Creatine Supplementation in Pediatric Orthopedic Rehabilitation: A Translational Review and Proposed Clinical Trial Framework
June 1, 2026 Creatine Supplementation in Pediatric Orthopedic Rehabilitation: A Translational Review and Proposed Clinical Trial Framework