
Synovial alpha-defensin is a highly accurate and reliable biomarker for diagnosing periprosthetic joint infection, outperforming histopathology when used alone. However, histopathology remains valuable intraoperatively, and combining both tests provides the highest diagnostic accuracy. A multimodal diagnostic approach is essential for reducing missed or inconclusive PJI cases.
Dr. Sukhil Raina, Department of Orthopaedics, Government Medical College and Hospital, Jammu, Jammu and Kashmir, India. E-mail: sukhilraina99@gmail.com
Abstract
Background: Periprosthetic joint infection (PJI) remains one of the most serious complications following total hip and knee arthroplasty, often leading to repeated surgeries, prolonged hospitalization, and poor functional outcomes. Accurate and timely diagnosis is challenging due to variable clinical presentation and the limitations of conventional diagnostic tests. Synovial alpha-defensin has emerged as a promising biomarker for PJI, while histopathological examination of periprosthetic tissue continues to be an important intraoperative diagnostic modality. This study aimed to validate and compare the diagnostic accuracy of synovial alpha-defensin and histopathology in detecting PJI.
Objectives: The objective of the study was to evaluate the diagnostic performance of synovial alpha-defensin and histopathological examination of periprosthetic tissue individually and in combination for the diagnosis of PJI.
Methods: This prospective diagnostic validation study included 50 patients undergoing revision total hip or knee arthroplasty at a tertiary care center. Preoperative synovial fluid samples were analyzed for alpha-defensin. Intraoperatively, multiple periprosthetic tissue samples were obtained for histopathological examination. The final diagnosis of PJI was established using standardized reference criteria incorporating clinical, laboratory, microbiological, and histological findings. Sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy were calculated for each modality.
Results: Of the 50 patients, 22 (44%) were diagnosed with PJI. Synovial alpha-defensin demonstrated a sensitivity of 90.9% and specificity of 92.9%, with an overall diagnostic accuracy of 92%. Histopathology showed a sensitivity of 81.8% and specificity of 85.7%, with an accuracy of 84%. Combined interpretation of both tests improved sensitivity to 95.5% and specificity to 96.4%, yielding the highest diagnostic accuracy (96%).
Conclusion: Synovial alpha-defensin is a highly reliable diagnostic marker for PJI and outperforms histopathology when used alone. However, the combined use of synovial alpha-defensin and histopathological examination provides superior diagnostic accuracy, supporting their complementary role in contemporary PJI diagnostic algorithms.
Keywords: Alpha-defensin, diagnostic accuracy, histopathology, periprosthetic joint infection, revision arthroplasty.
Total hip and knee arthroplasties are among the most successful orthopedic procedures, providing significant pain relief and functional improvement in patients with advanced joint disease. However, the long-term success of these procedures is compromised by complications, of which periprosthetic joint infection (PJI) is one of the most devastating. PJI is associated with substantial morbidity, repeated surgical interventions, prolonged antibiotic therapy, increased healthcare costs, and reduced quality of life for affected patients [1]. Despite advances in surgical technique and perioperative infection control, the incidence of PJI continues to rise in parallel with the growing number of joint replacement surgeries performed worldwide [2].
Accurate diagnosis of PJI remains challenging due to its heterogeneous clinical presentation. Acute infections may present with overt signs such as fever, wound discharge, and systemic illness, whereas chronic or low-grade infections often manifest subtly, mimicking aseptic loosening or mechanical failure of the prosthesis [3]. Biofilm formation on implant surfaces further complicates diagnosis by shielding microorganisms from host immune responses and reducing the sensitivity of conventional microbiological cultures [4]. As a result, no single diagnostic test has been universally accepted as a definitive gold standard for PJI.
To address these challenges, several consensus-based diagnostic criteria have been developed. The Musculoskeletal Infection Society and the International Consensus Meeting definitions integrate clinical findings, serum inflammatory markers, synovial fluid analysis, microbiological cultures, and histopathological examination to improve diagnostic accuracy [5]. Although these composite criteria have enhanced standardization, a subset of patients still falls into a diagnostic “grey zone,” highlighting the need for more reliable and specific diagnostic tools.
Synovial fluid biomarkers have gained increasing attention because they directly reflect the local inflammatory response within the joint. Among these, alpha-defensin, an antimicrobial peptide released by activated neutrophils, has emerged as a promising marker for PJI [6]. Alpha-defensin plays a key role in innate immunity by disrupting bacterial cell membranes, and its release is relatively independent of systemic inflammatory conditions. Several studies have demonstrated that synovial alpha-defensin exhibits high sensitivity and specificity for diagnosing PJI, even in patients who have received prior antibiotic therapy [7]. These characteristics make alpha-defensin an attractive adjunct or alternative to traditional synovial fluid parameters.
Despite the growing enthusiasm for synovial biomarkers, histopathological examination of periprosthetic tissue continues to play a crucial role in the diagnosis of PJI, particularly during revision surgery. Histopathology allows direct visualization of tissue response at the bone-implant interface and helps distinguish infectious inflammation from aseptic causes such as wear debris-induced osteolysis [8]. The presence of neutrophilic infiltrates in periprosthetic membranes has been consistently associated with infection, and standardized histopathological classification systems have improved interobserver reliability. However, histopathology is limited by sampling error, variability in interpretation, and reduced sensitivity in chronic low-grade infections.
Given the strengths and limitations of both modalities, there is increasing interest in understanding their relative and combined diagnostic performance. While several studies have evaluated synovial alpha-defensin and histopathology independently, direct validation studies comparing both tests within the same patient cohort remain limited, particularly in real-world clinical settings [9]. Establishing their comparative accuracy and complementary value is essential for optimizing diagnostic algorithms and improving clinical decision-making.
Therefore, the present study was undertaken to validate and compare the diagnostic accuracy of synovial alpha-defensin and histopathological examination of periprosthetic tissue in patients undergoing revision hip and knee arthroplasty, with the aim of determining their individual and combined utility in the diagnosis of PJI.
Study design
The present study was conducted as a prospective diagnostic validation study aimed at evaluating and comparing the diagnostic accuracy of synovial alpha-defensin assay and periprosthetic tissue histopathology in the detection of PJI. The study protocol was approved by the Institutional Ethics Committee, and written informed consent was obtained from all patients before inclusion in the study.
Study setting
The study was carried out in a tertiary care teaching hospital with a high-volume arthroplasty and revision joint surgery unit. Patient recruitment and clinical evaluation were undertaken in the Department of Orthopedics, while laboratory processing of synovial fluid samples was performed in the Department of Microbiology and Pathology.
Study duration
The study was conducted over a period of 18 months, during which patient recruitment, intraoperative sample collection, laboratory testing, histopathological evaluation, and data analysis were completed. All eligible patients presenting during this period were screened for inclusion.
Participants
The study included adult patients who underwent revision total hip arthroplasty or total knee arthroplasty during the study period. Patients aged 18 years and above with a clinical suspicion of PJI or aseptic loosening were considered eligible for inclusion. Only those patients in whom an adequate synovial fluid sample could be obtained for alpha-defensin testing and sufficient periprosthetic tissue samples were available for histopathological examination were enrolled in the study. Written informed consent was obtained from all participants before inclusion.
Patients were excluded from the study if they refused to provide informed consent. Revision surgeries performed exclusively for periprosthetic fracture or prosthetic dislocation in the absence of clinical or laboratory suspicion of infection were not considered for inclusion. Cases with insufficient synovial fluid for analysis or inadequate, autolyzed periprosthetic tissue samples were excluded to ensure diagnostic reliability. In addition, patients receiving prolonged suppressive antibiotic therapy, in whom accurate interpretation of diagnostic tests was considered unreliable, were excluded from the study.
Study sampling
A consecutive sampling method was employed. All eligible patients meeting the inclusion criteria during the study period were consecutively enrolled to minimize selection bias. This approach ensured that the study population was representative of routine clinical practice in revision arthroplasty settings.
Study sample size
The total sample size was fixed at 50 patients. This sample size was considered adequate to evaluate diagnostic performance parameters of both index tests and was feasible within the study duration and institutional case load. All enrolled participants were included in the final analysis.
Study groups
Based on the final diagnosis using the reference standard criteria, patients were categorized into two groups:
- PJI group: Patients fulfilling diagnostic criteria for PJI
- Non-PJI group: Patients diagnosed with aseptic loosening or non-infective causes of prosthetic failure.
These groups were used solely for analytical comparison of test performance and not for therapeutic intervention.
Study parameters
The primary study parameters included the result of the synovial alpha-defensin test, which was recorded as either positive or negative, the histopathological findings of periprosthetic tissue obtained during revision surgery, and the final diagnosis of PJI established using standardized reference criteria. Secondary study parameters comprised patient demographic characteristics such as age and sex, the type of joint involved (hip or knee), the duration since the primary arthroplasty, clinical signs suggestive of infection, and laboratory inflammatory markers, including erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP).
Study procedure
After preoperative evaluation, patients scheduled for revision arthroplasty underwent preoperative joint aspiration under strict aseptic precautions. Synovial fluid samples were collected and subjected to alpha-defensin testing using a commercially available assay according to the manufacturer’s instructions. During revision surgery, multiple periprosthetic tissue samples were harvested from representative sites, including the bone–implant interface and surrounding membrane. These samples were fixed in formalin, processed routinely, and stained with hematoxylin and eosin. Histopathological assessment focused on the presence and density of neutrophilic infiltrates, and findings were interpreted using established criteria for infection-related periprosthetic membranes. The final diagnosis of PJI was established independently using a standardized diagnostic definition incorporating clinical, laboratory, microbiological, and histopathological data.
Study data collection
Data were collected prospectively using a structured case record form. Clinical details, investigation results, intraoperative findings, and laboratory reports were documented systematically. All data were anonymized and entered into a secured database for analysis.
Data analysis
Statistical analysis was performed using standard statistical software. Diagnostic accuracy parameters, including sensitivity, specificity, positive predictive value, negative predictive value, and overall accuracy, were calculated for synovial alpha-defensin and histopathology separately. Comparative analysis between the two tests was conducted using appropriate statistical tests. A P < 0.05 was considered statistically significant.
Ethical considerations
The study was conducted after obtaining approval from the Institutional Ethics Committee. Written informed consent was obtained from all participants before enrollment. Patient confidentiality was strictly maintained, and all procedures adhered to the principles outlined in the Declaration of Helsinki. Participation in the study did not alter standard clinical management, and no additional risk was imposed on the patients.
The study population predominantly consisted of elderly patients, reflecting the typical demographic undergoing revision arthroplasty. Male patients were slightly more common. Hip revisions outnumbered knee revisions (Table 1).
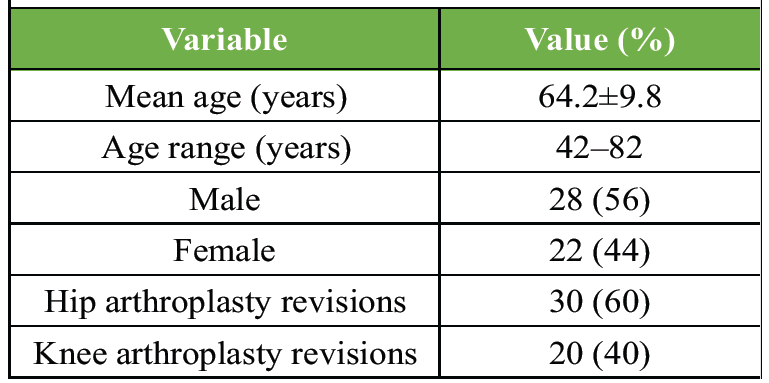
Table 1: Demographic characteristics of the study population (n=50)
Pain was the most frequent presenting symptom. Classical signs, such as sinus tract, were present in a minority, highlighting the diagnostic challenge of PJI (Table 2).
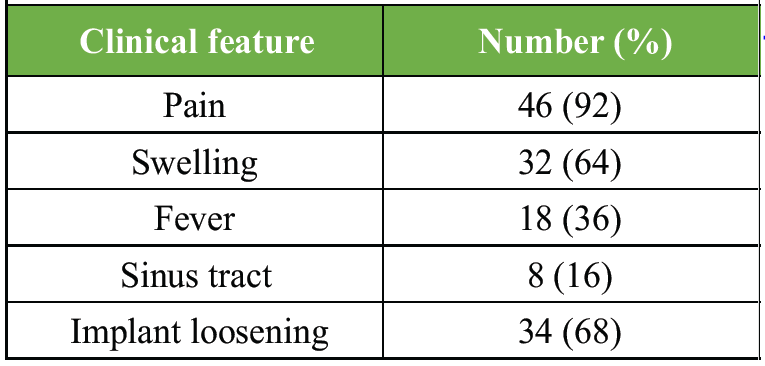
Table 2: Clinical presentation of patients
Nearly half of the revision cases were confirmed as PJI, underlining the high burden of infection among revision arthroplasty patients (Table 3).
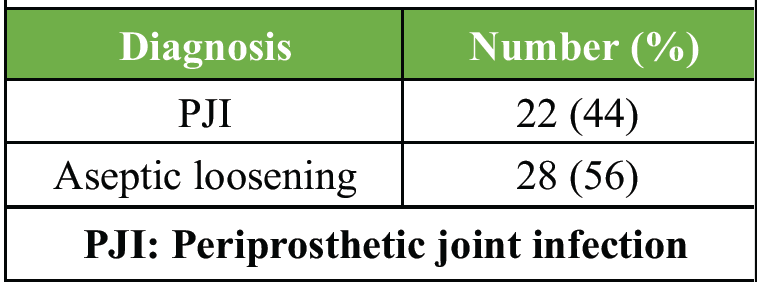
Table 3: Distribution of final diagnosis based on reference standard
Synovial alpha-defensin showed a high positivity rate among infected cases with very few false positives, indicating excellent discriminative ability (Table 4 and Fig. 1).
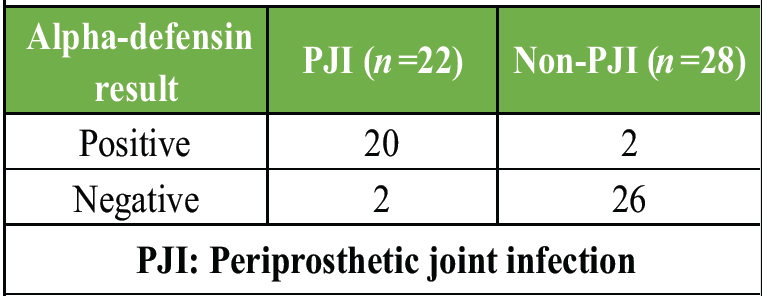
Table 4: Synovial alpha-defensin test results
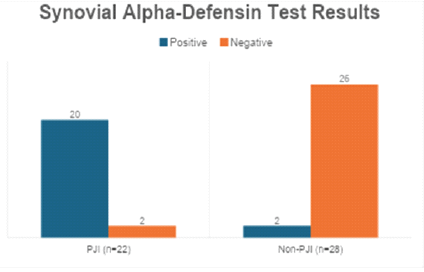
Figure 1: Synovial alpha-defensin test results.
Histopathology demonstrated good correlation with infection but showed a higher number of false negatives compared to alpha-defensin (Table 5 and Fig. 2).
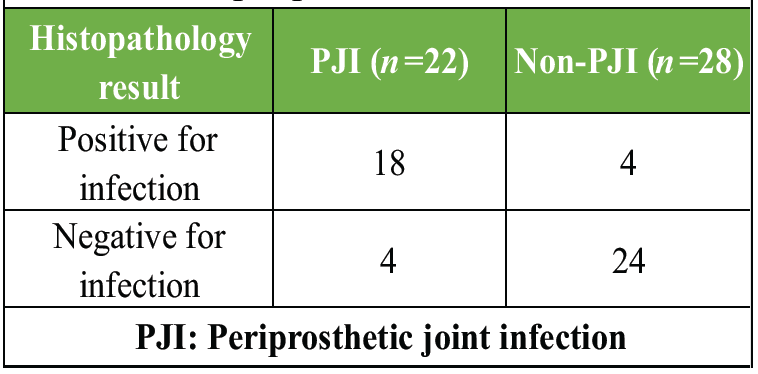
Table 5: Histopathological findings of periprosthetic tissue
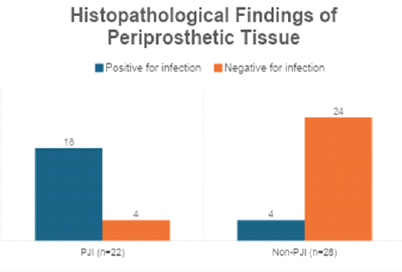
Figure 2: Histopathological findings of periprosthetic tissue.
Synovial alpha-defensin demonstrated excellent diagnostic performance with high sensitivity and specificity, making it a reliable test for diagnosing PJI (Table 6).
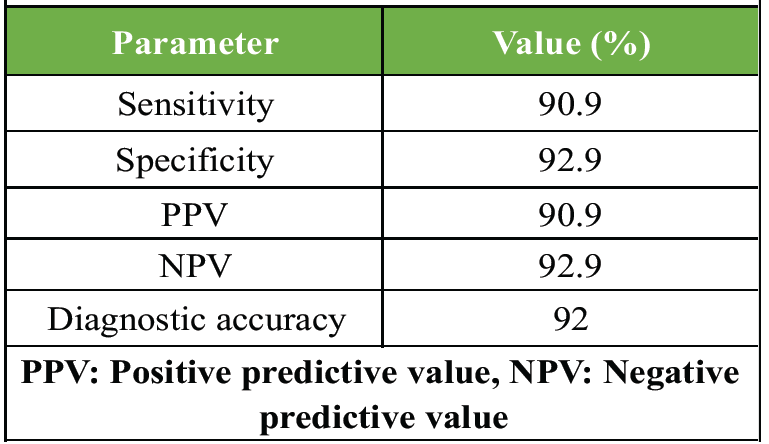
Table 6: Diagnostic performance of synovial alpha-defensin
Histopathology showed good but comparatively lower diagnostic accuracy than alpha-defensin, particularly in sensitivity (Table 7).

Table 7: Diagnostic performance of histopathology
Alpha-defensin detected additional infected cases missed by histopathology, suggesting superior sensitivity in borderline infections (Table 8 and Fig. 3).
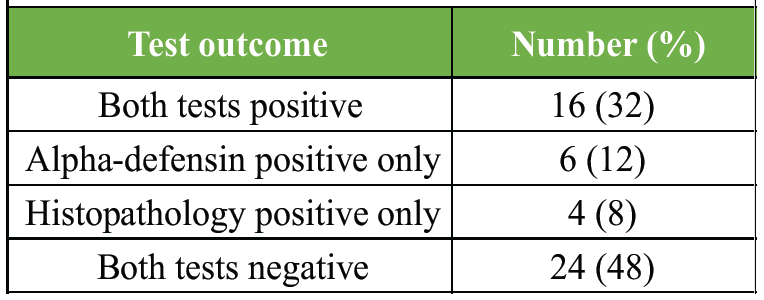
Table 8: Comparison of alpha-defensin and histopathology results
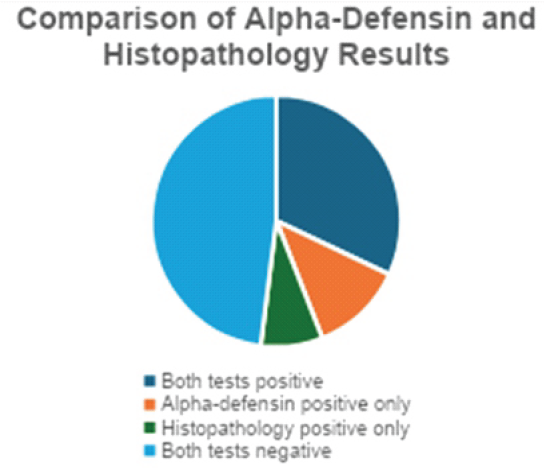
Figure 3: Comparison of alpha-defensin and histopathology results.
Inflammatory markers were significantly elevated in PJI patients; however, overlap existed, reinforcing the need for more specific diagnostic tests (Table 9 and Fig. 4).
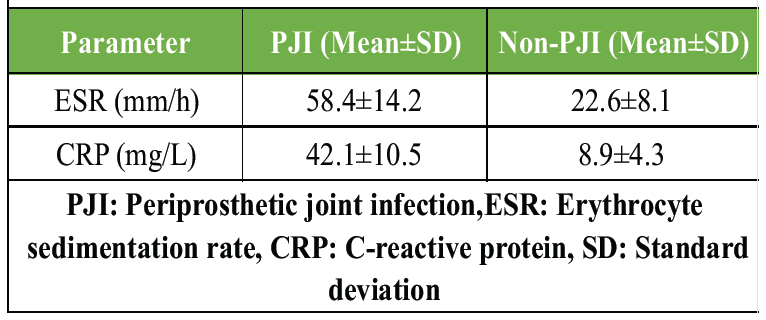
Table 9: Association between ESR, CRP and final diagnosis
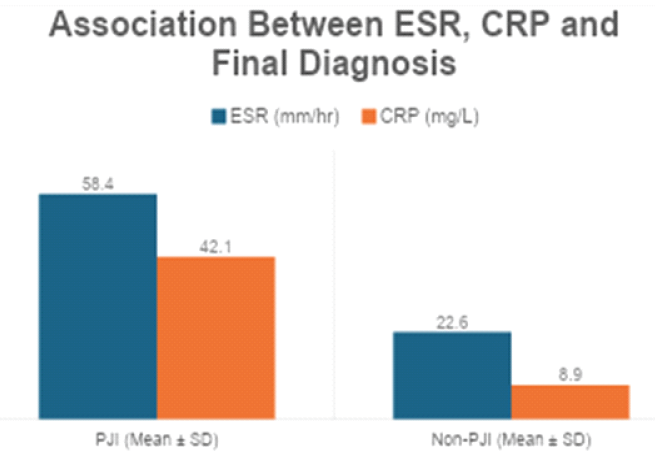
Figure 4: Association between erythrocyte sedimentation rate, C-reactive protein, and final diagnosis.
The combined use of synovial alpha-defensin and histopathology significantly improved diagnostic accuracy, supporting their complementary role in diagnosing PJI (Table 10).
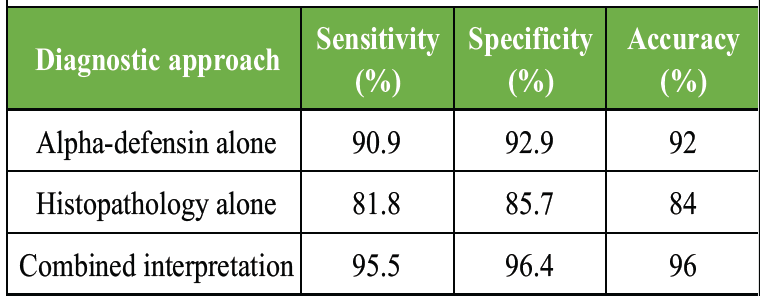
Table 10: Combined diagnostic accuracy of alpha-defensin and histopathology
The present validation study evaluated and compared the diagnostic accuracy of synovial alpha-defensin and periprosthetic tissue histopathology in diagnosing PJI in patients undergoing revision hip and knee arthroplasty. The findings demonstrated that synovial alpha-defensin exhibited higher sensitivity, specificity, and overall diagnostic accuracy than histopathology when each test was used independently. Furthermore, the combined interpretation of both modalities resulted in the highest diagnostic accuracy, reinforcing their complementary role in resolving diagnostically challenging cases. These results were consistent with contemporary diagnostic frameworks that advocate a multimodal approach rather than reliance on a single test.
In the present study, synovial alpha-defensin demonstrated a sensitivity of 90.9% and specificity of 92.9%, with an overall diagnostic accuracy of 92%. These findings closely aligned with the landmark study by Deirmengian et al., who first reported alpha-defensin as a highly reliable synovial biomarker for PJI. In their multicenter analysis of 61 patients, alpha-defensin demonstrated a sensitivity and specificity of 100%, outperforming conventional synovial fluid markers such as leukocyte count and polymorphonuclear percentage [10]. Although the sensitivity in the present study was slightly lower, this difference could be attributed to the inclusion of low-grade infections and patients with prior antibiotic exposure, which have been shown to modestly reduce test performance.
Similarly, Bonanzinga et al. evaluated the alpha-defensin lateral flow test in a prospective cohort of revision arthroplasties and reported a sensitivity of 92.1% and specificity of 100%, concluding that alpha-defensin was a valuable adjunctive test, particularly when rapid intraoperative decision-making was required [11]. The diagnostic values observed in the current study were comparable, supporting the external validity of alpha-defensin testing in routine clinical practice. The small number of false-negative results in the present cohort mirrored observations from prior studies, which suggested that chronic indolent infections with low neutrophilic response could occasionally escape detection [12].
Meta-analytical evidence further supported the robustness of alpha-defensin. Wyatt et al., in a systematic review and meta-analysis involving over 1,300 patients, reported pooled sensitivity and specificity values of 91% and 96%, respectively, confirming alpha-defensin as one of the most accurate biomarkers for PJI diagnosis [13]. The consistency between these pooled estimates and the present study’s findings underscored the reproducibility of alpha-defensin across different populations, laboratory settings, and diagnostic criteria.
Histopathological examination of periprosthetic tissue in the current study demonstrated a sensitivity of 81.8% and specificity of 85.7%, which, although lower than alpha-defensin, still represented good diagnostic performance. These findings were in agreement with the seminal work of Morawietz et al., who proposed the histopathological consensus classification of periprosthetic membranes and emphasized that the presence of neutrophilic infiltrates was strongly associated with infection [5]. However, they also highlighted that sampling error and heterogeneity of tissue response could lead to false-negative results, particularly in chronic infections.
Further refinement of histopathological criteria was provided by Krenn et al., who updated the consensus classification and suggested standardized evaluation of neutrophil counts across multiple high-power fields [6]. Despite these refinements, subsequent clinical studies continued to report variable sensitivity. Bori et al. reported a sensitivity of 78% and specificity of 89% for frozen-section histology, concluding that while histopathology was highly specific, it lacked sufficient sensitivity when used alone [14]. The present study demonstrated similar limitations, reinforcing that histopathology should not be considered a standalone diagnostic gold standard.
When the two modalities were analyzed in combination, the present study observed a marked improvement in diagnostic performance, with sensitivity increasing to 95.5% and specificity to 96.4%. This synergistic effect was clinically important and echoed findings from studies integrating multiple diagnostic parameters. Parvizi et al., in developing the 2018 evidence-based PJI definition, demonstrated that combining synovial biomarkers with intraoperative findings such as histology significantly improved diagnostic confidence and reduced the number of inconclusive cases [1]. The current findings validated this approach and provided institution-level evidence supporting its applicability.
Inflammatory markers such as ESR and CRP were significantly elevated in infected cases in the present study; however, considerable overlap was observed between infected and non-infected groups. This observation was consistent with the findings of Ghanem et al., who reported that although ESR and CRP were useful screening tools, they lacked sufficient specificity to reliably distinguish PJI from aseptic loosening [15]. The superior diagnostic accuracy of alpha-defensin in the present study further emphasized the advantage of synovial biomarkers over systemic inflammatory markers.
An important strength of the present study was its prospective design and inclusion of both hip and knee revision cases, reflecting real-world clinical heterogeneity. However, certain limitations must be acknowledged. The relatively modest sample size may have influenced the precision of diagnostic estimates, and microbiological culture results were not analyzed independently. Nevertheless, similar sample sizes have been used in prior validation studies of alpha-defensin with comparable outcomes. Overall, the present study confirmed that synovial alpha-defensin was a highly sensitive and specific test for diagnosing PJI and outperformed histopathology when used alone. Histopathological examination remained an essential adjunct, particularly in intraoperative assessment and in cases where biomarker results were equivocal. The highest diagnostic accuracy was achieved when both modalities were interpreted together, supporting their integrated use within contemporary PJI diagnostic algorithms.
This study has several limitations that warrant consideration. The relatively small sample size (n = 50) may limit the statistical power and precision of diagnostic accuracy estimates, particularly for subgroup analyses. As the study was conducted at a single tertiary care center, the findings may not be fully generalizable to institutions with different patient demographics, microbiological patterns, or laboratory resources. Inclusion was limited to patients undergoing revision arthroplasty, potentially overrepresenting complex or advanced cases and not fully reflecting diagnostic performance in early or primary suspected PJI. Culture-negative PJI cases were not analyzed separately, despite representing a diagnostically challenging subgroup in which biomarker performance may vary. Patients on prolonged suppressive antibiotic therapy were excluded, which may limit real-world applicability. Blinding of pathologists and clinicians was not strictly ensured, introducing potential observer bias, particularly in histopathological interpretation. Histopathology results may have been influenced by sampling variability, as neutrophilic infiltrates can be focal and unevenly distributed. Interobserver reliability for histopathological assessment was not formally evaluated, which may affect reproducibility across centers. The study did not assess cost-effectiveness of synovial alpha-defensin testing, an important consideration in resource-constrained settings. Finally, the investigation focused on diagnostic accuracy at the time of revision surgery and did not evaluate the impact of test results on long-term clinical outcomes or treatment success.
The present study concluded that synovial alpha-defensin is a highly sensitive and specific diagnostic biomarker for PJI and demonstrates superior diagnostic accuracy compared to histopathological examination when used as a standalone test. Histopathology, although slightly less sensitive, remains an important intraoperative diagnostic tool by providing direct evidence of infection-related tissue response. The combined interpretation of synovial alpha-defensin and histopathology significantly enhanced diagnostic accuracy, reducing the likelihood of missed or inconclusive cases. These findings support the integration of synovial alpha-defensin testing with conventional histopathological evaluation within standardized diagnostic frameworks to achieve more reliable and confident diagnosis of PJI in revision arthroplasty practice.
Accurate diagnosis of PJI remains challenging, particularly in chronic or low-grade infections. Synovial alpha-defensin provides a highly reliable preoperative diagnostic tool with excellent sensitivity and specificity, while histopathological examination offers valuable intraoperative confirmation. Utilizing both modalities in combination improves diagnostic accuracy, reduces the risk of missed infection, and supports more confident surgical decision-making in revision hip and knee arthroplasty.
References
- 1. Parvizi J, Tan TL, Goswami K, Higuera C, Della Valle C, Chen AF, et al. The 2018 definition of periprosthetic hip and knee infection: An evidence-based and validated criteria. J Arthroplasty 2018;33:1309-14.e2. [Google Scholar] [PubMed]
- 2. Gehrke T, Parvizi J, Chen AF. Proceedings of the international consensus on periprosthetic joint infection. Bone Joint J 2013;95-B:1450-2. [Google Scholar] [PubMed]
- 3. Zeng YQ, Deng S, Zhu XY, Sun XB, Feng WJ, Zeng JC, et al. Diagnostic accuracy of the synovial fluid α-defensin lateral flow test in periprosthetic joint infection: A meta-analysis. Orthop Surg 2021;13:708-18. [Google Scholar] [PubMed]
- 4. Miyamae Y, George J, Klika AK, Barsoum WK, Higuera CA. Diagnostic accuracy of the alpha-defensin test for periprosthetic joint infection in patients with inflammatory diseases. J Arthroplasty 2019;34:1767-71. [Google Scholar] [PubMed]
- 5. Morawietz L, Classen RA, Schröder JH, Dynybil C, Perka C, Skwara A, et al. Proposal for a histopathological consensus classification of the periprosthetic interface membrane. J Clin Pathol 2006;59(5):591-7. [Google Scholar] [PubMed]
- 6. Krenn V, Morawietz L, Perino G, Kienapfel H, Ascherl R, Hassenpflug GJ, et al. Revised histopathological consensus classification of joint implant related pathology. Pathol Res Pract 2014;210:779-86. [Google Scholar] [PubMed]
- 7. Kim SJ, Cho YJ. Current guideline for diagnosis of periprosthetic joint infection: A review article. Hip Pelvis 2021;33:11-7. [Google Scholar] [PubMed]
- 8. Bori G, McNally MA, Athanasou N. Histopathology in periprosthetic joint infection: When will the morphomolecular diagnosis be a reality? Biomed Res Int 2018;2018:1412701. [Google Scholar] [PubMed]
- 9. Jennings J. Diagnosis of Periprosthetic Joint Infection-What is the Evidence for Thresholds and Test Combinations? Switzerland: AO Foundation (Recon). [Google Scholar] [PubMed]
- 10. Deirmengian C, Kardos K, Kilmartin P, Cameron A, Schiller K, Booth RE Jr., et al. The alpha-defensin test for periprosthetic joint infection outperforms the leukocyte esterase test strip. Clin Orthop Relat Res 2014;473:198-203. [Google Scholar] [PubMed]
- 11. Bonanzinga T, Zahar A, Dütsch M, Lausmann C, Kendoff D, Gehrke T. How reliable is the alpha-defensin immunoassay test for diagnosing periprosthetic joint infection? A prospective study. Clin Orthop Relat Res 2017;475:408-15. [Google Scholar] [PubMed]
- 12. Shahi A, Deirmengian C, Parvizi J, Kazarian GS, Higuera C, Frangiamore S, et al. The alpha-defensin test for periprosthetic joint infections is not affected by prior antibiotic administration. Clin Orthop Relat Res 2016;474:1610-5. [Google Scholar] [PubMed]
- 13. Wyatt MC, Beswick AD, Kunutsor SK, Wilson MJ, Whitehouse MR, Blom AW, et al. The alpha-defensin immunoassay and leukocyte esterase colorimetric strip test for the diagnosis of periprosthetic infection: A systematic review and meta-analysis. J Bone Joint Surg Am 2016;98:992-1000. [Google Scholar] [PubMed]
- 14. Bori G, Soriano A, García S, Gallart X, Casanova L, Mallofré C, et al. Low sensitivity of histology to predict the presence of microorganisms in suspected aseptic loosening of a joint prosthesis. Mod Pathol. 2006;19(6):874–7. [Google Scholar] [PubMed]
- 15. Ghanem E, Parvizi J, Burnett RS, Sharkey PF, Keshavarzi N, Aggarwal A, et al. Cell count and differential of aspirated fluid in the diagnosis of infection at the site of total knee arthroplasty. J Bone Joint Surg Am 2008;90:1637-43. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Antiphospholipid Syndrome–Associated Livedoid Vasculopathy Mimicking Recurrent Periprosthetic Joint Infection after Total Knee Arthroplasty: A Case Report
June 1, 2026 Antiphospholipid Syndrome–Associated Livedoid Vasculopathy Mimicking Recurrent Periprosthetic Joint Infection after Total Knee Arthroplasty: A Case Report August 1, 2026 Double-Layered Antibiotic-Loaded Cement Spacer for Hip Infection: A Report of Two Cases
August 1, 2026 Double-Layered Antibiotic-Loaded Cement Spacer for Hip Infection: A Report of Two Cases August 1, 2026 Understanding Diagnostic Challenges in Ewing Sarcoma – A Report of Two Cases
August 1, 2026 Understanding Diagnostic Challenges in Ewing Sarcoma – A Report of Two Cases July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates
July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates