
Simultaneous staged total hip and knee arthroplasty can restore ambulation in severe ankylosing spondylitis with autoarthrodesis when carefully planned with attention to positioning, neurovascular risk, and staged rehabilitation.
Varun M. Trivedi, The University of Texas Medical Branch, School of Medicine, Galveston, Texas, USA. E-mail: vatrived@utmb.edu
Abstract
Introduction: Ankylosing spondylitis (AS) is a chronic inflammatory disease that can lead to progressive joint ankylosis, most commonly affecting the spine and hips. Severe cases may result in functional autoarthrodesis of multiple lower extremity joints, significantly impairing mobility and quality of life. Although total hip and knee arthroplasty are well-described individually in AS, management of simultaneous multi-joint ankylosis in extreme flexion deformity is rarely reported.
Case Report: We report the case of a 23-year-old male with advanced AS resulting in bilateral hip and knee autoarthrodesis fixed in severe flexion, rendering him wheelchair-bound for 3 years. He underwent four staged arthroplasty procedures over the course of 1 year, consisting of bilateral total hip arthroplasties followed by bilateral total knee arthroplasties, with approximately 8-week intervals between procedures. Significant intraoperative challenges included absent normal joint anatomy, extreme flexion deformities (hips 80–85° and knees 70–75°), and complex patient positioning. The hips were addressed through an anterolateral approach, and the knees through a medial parapatellar approach with adjunctive osteotomies and soft-tissue releases as needed. Postoperatively, the patient underwent intensive rehabilitation and subsequent manipulation under anaesthesia to improve the range of motion. Functional outcome measures demonstrated substantial improvement, with hip disability and osteoarthritis outcome score increasing from 6.9 to 61.3, Harris Hip Score from 15 to 63, and knee injury and osteoarthritis outcome score from 9 to 41.
Conclusion: Staged total hip and knee arthroplasty in severe AS with autoarthrodesis can result in meaningful functional recovery. Careful pre-operative planning, staged reconstruction, and tailored rehabilitation are essential to optimize outcomes and minimize complications in these complex cases.
Keywords: Arthroplasty, ankylosing spondylitis, case report, autoarthrodesis, spontaneous, flexion contracture.
Ankylosing spondylitis (AS) is a chronic, progressive, inflammatory disease with a predilection for the axial joints, specifically the spine and hip joints [1,2]. AS is most commonly present in younger males (15–30 years old) with persistent back pain and stiffness that is worse in the mornings and nights but improves with activity [3]. Despite research efforts, the etiology and pathogenesis of AS remain unclear [4]. Patients with AS commonly experience progressive joint fusion as a result of excessive bone formation, which ultimately results in bone spurs and poor physical function [5,6]. Furthermore, the chronic inflammation in AS can eventually lead to involvement of the spine, hips, knees, and shoulders, among other joints [7]. Hip involvement as AS progresses is more prominent in males, with a younger age of onset, and leads to more significant functional impairment, which eventually requires total hip arthroplasty (THA) [8]. The knee remains an uncommonly affected joint in AS; however, abnormal weight-bearing in the presence of inflammation may result in knee damage that necessitates total knee arthroplasty (TKA) [9]. Here, we report a unique case of a young male undergoing bilateral THA and TKA secondary to the progression of his AS. The patient was informed that data concerning his case would be submitted for publication, and he provided consent.
A 23-year-old male presented to the orthopedics clinic with spontaneous progressive fusion of the bilateral knee and hip joints. The patient’s hips are fully fused in 80–85° flexion, neutral rotation, and slight adduction, whereas his knees are fused in 70–75° flexion. The patient states that before his first visit to the clinic, he had been immobile and wheelchair-bound for 3 years. He remarks no specific prior deterioration timeline knowledge other than “trouble moving for years”. After discussion with the patient, it was decided to perform arthroplasties on all four affected joints over the course of a year as his recovery permitted. The patient was dissuaded from undergoing multiple arthroplasties in one setting due to the complexity of the procedures and anticipated difficulties in recovery. Hip replacements were performed first due to the potential operative complications from a fixed hip joint during a knee replacement, as well as awkward post-surgery physical therapy. On July 26, 2023, a left THA was performed. Postoperative imaging following bilateral THA is shown in Fig. 1a. Pre-operative imaging demonstrated severe bilateral hip autoarthrodesis in extreme flexion with absent normal joint anatomy (Figs. 1b and c).
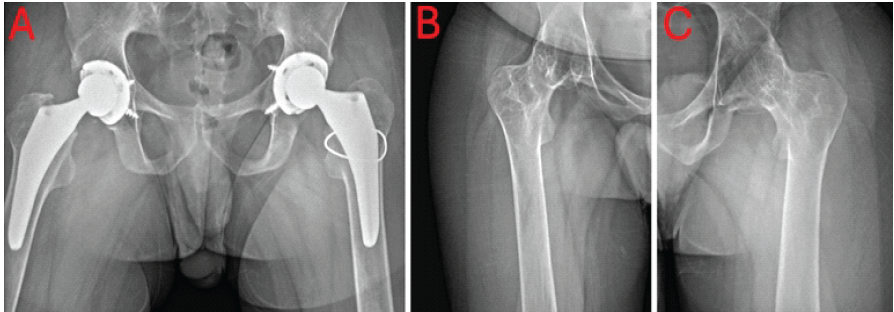
Figure 1: (a) Post-operative anteroposterior (AP) X-ray of bilateral hips. (b) Pre-operative AP X-ray of the right hip. (c) Pre-operative AP X-ray of the left hip.
After uneventful spinal and general anaesthesia, the patient was placed in the lateral decubitus position. An anterolateral approach was used. The iliotibial band was split, and the anterior third of the gluteus medius and gluteus minimus were released. The anterior capsule was excised, and the anterior and superior neck identified. There was no distinguishable joint or labrum to use as a landmark. A 1–1.5 cm wide wedge osteotomy was created in the general location of a typical femoral neck osteotomy for a THA. The osteotomy was completed with an osteotome. The leg was then able to be externally rotated enough to perform a more accurate neck osteotomy. Once completed, a cable was passed due to a small cortical defect created by the osteotome during the initial osteotomy. Fluoroscopy was used next to get orientated, and then the remaining neck and head were gradually resected using a rongeur. Fortunately, the cotyloid notch was quickly encountered, still having the typical anatomy and interposed fat. This gave a solid, familiar landmark to continue. A small reamer was used initially, and the position was confirmed on fluoroscopy. Reaming progressed to 50 mm, and a Stryker Trident II Tritanium multi-hole acetabular component was inserted. Screws were placed due to concerns about overall bone quality. A trial liner was placed, and the femur was addressed next. The femoral preparation proceeded uneventfully, and a size 7 Stryker Accolade II stem was placed with good stability. The hip was reduced and taken through a range of motion (ROM). All components appeared well-positioned, and this was confirmed on fluoroscopy (Fig. 1a). Internal and external rotation were surprisingly good; however, as expected, the hip extension was restricted. The hip would extend with a flexion contracture of approximately 20°. A flexor tenotomy was not done. We did not want to contribute any more to weakness in this difficult setting, thinking the patient would be able to rehabilitate the hip and improve his extension over time. Post-operative rehabilitation was modified due to obvious limitations involving the other joints. Focus was placed on hip extension, active flexion, and rotation. On September 08, 2023, the right hip was replaced. At this time, the patient had improved to only a 10° hip flexion contracture. He was actively flexing to >95° and could actively internally and externally rotate 10° and 30°, respectively. The right hip arthroplasty proceeded essentially like the first, apart from the proximal femur cable. No cable was needed in this case. A similar rehabilitation protocol was used for active ROM and passive hip extension. The decision was made to proceed with the left total knee on October 27, 2023. Pre-operative imaging demonstrated bilateral knee ankylosis with severe flexion deformity and joint obliteration (Fig. 2a, b, c).
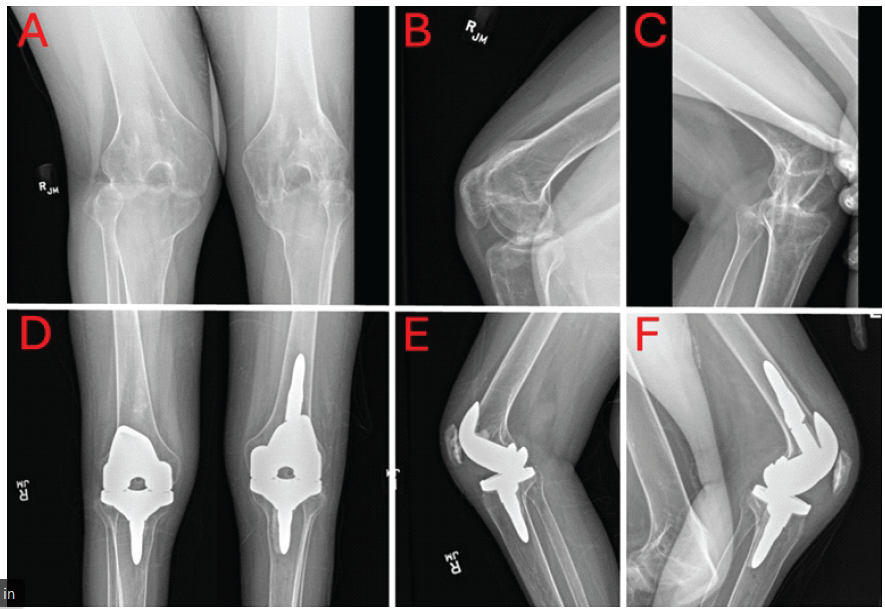
Figure 2: (a) Pre-operative anteroposterior (AP) X-ray of bilateral knees. (b) Pre-operative lateral X-ray of the right knee. (c) Pre-operative lateral X-ray of the left knee. (d) Post-operative AP X-ray of bilateral knees. (e) Post-operative lateral X-ray of the right knee. (f) Post-operative lateral X-ray of the left knee.
The patient had continued to see hip improvement. The left hip had a 5° flexion contracture and the right a 10° flexion contracture. The knee was also done using spinal and general anaesthesia. After prepping, the leg was exsanguinated, and the tourniquet inflated. An anterior incision and medial parapatellar approach were performed. The patella was completely fused to the femur; however, the joint line area was distinguishable. An osteotome was used to cut down to the center of the trochlear groove. Freeing the lateral facet proved more difficult. The quadriceps tendon was surprisingly mobile; however, the inferior lateral aspect could not be reached. When the patella was elevated, a small piece of the patella remained on the femur. It was able to be mobilised enough to do a provisional patella osteotomy, which allowed for more visualization of the femur. An osteotome was then used to release the femur from the tibia. This was done using fluoroscopic assistance. The intramedullary guide was used, and an initial 10 mm resection of the distal femur was completed. Making the cut to free the femur from the tibia naturally disturbed the normal posterior condyle reference, so revision instruments were used to perform the remaining femoral osteotomies using the epicondylar axis as a reference. The tibia was prepared using the intramedullary guide in the standard fashion. As expected, the extension gap was significantly less than the flexion gap. A 4 mm additional resection of the distal femur was done, and the femur was upsized with posterior augments to decrease the flexion gap. Doing this, the knee was able to extend to 20°. A posterior capsule release was done, and manual stretching improved extension to about a 10–15° contracture. This range was accepted due to fear of peroneal nerve stretch and again thinking that at his age he would be able to undergo rehabilitation and improve postoperatively. On December 26, 2023, the right total knee was performed in the same fashion as the left knee, with post-operative radiographs confirming implant positioning (Fig. 2d, e, f). A similar rehabilitation protocol was used for active ROM and passive knee extension. A few months later, on February 09, 2024, the patient underwent bilateral manipulation of the knee joints. We started with about 25° of flexion on the right and got him down to a little less than 10° and started with about 15° on the left and got him down to a little less than 10°. Flexion was excellent but was manipulated gently. The patient tolerated the procedure well with no significant complications postoperatively. To quantify the improvement in quality of life, the patient completed several questionnaires both before and after surgery. For hip assessment, we used the hip disability and osteoarthritis outcome score (HOOS) [9] and the Harris hip score (HHS) [10]. For knee assessment, we used the Knee Injury and Osteoarthritis Outcome Score (KOOS) [11,12]. The patient demonstrated improvement across all measures: The HOOS increased from 6.9 to 61.3 points, the HHS rose from 15 to 63 points, and the KOOS improved from 9 to 41 points.
To our knowledge, this is the only case in which all four joints were replaced within the same year because of progressively worsening AS with an added complication of the unique spontaneous fusion positioning. As arthroplasty after arthrodesis, either spontaneous or operative, has been shown to be an effective treatment course [13,14,15], we had no cause to think that the outcome for these four arthroplasties would be any different. The only thing that concerned our team when approaching this issue was the lack of available information on the potential risks and methodology of operating on joints that are fused in such unusual positions. As hip arthrodesis flexions are typically between 20° and 35° [16], and knee arthrodesis is generally performed with the joint in 5–7° of valgus and 15 ± 5° of flexion [17,18], sources detailing the specific techniques used during takedown surgery are not directly applicable to this case where we had a hip and knee flexion of 80–85°. Positioning the patient and preparing the surgical field presented some unique challenges that had to be addressed on a case-by-case basis. The first hip surgery was the most difficult, due to the total lack of mobility, and extra precautions were taken to not apply undue force and torque to the fused joints that could lead to fractures. For the second surgery, we were able to extend the non-operative hip, removing the left knee from the surgical field. This allowed for improved flexion and external rotation of the operative hip during the osteotomy of the femur and reaming of the acetabulum. During the first knee surgery, we had to slightly externally rotate the non-operative leg’s hip to remove it from the surgical field. Although inconvenient and awkward, it did not interfere with the operative knee’s final ROM testing. The last surgery was the easiest, with the only deviation from normal being the excessive starting flexion; however, it proceeded smoothly after releasing the tibia from the femur. For the hip joints, our primary concern was achieving the desired extension without putting too much strain on the iliopsoas. Because of the chronic flexion contracture and the immediate improvement in surgery of getting near full extension, it was thought that post-surgery rehabilitation would allow for full recovery of ROM in the patient. There was a slight concern for femoral nerve palsy following the procedure, but this is a rare complication [19,20], and near-complete recovery with only mild motor deficits can be expected [21]. Hip rehabilitation went smoothly, and the patient was adequately motivated. Steady improvement was seen bilaterally. For the knee joints, our primary concern was to avoid stretching the peroneal nerve. Peroneal nerve injury is a rare but devastating complication post-total knee replacement [22]. Injury can occur due to retractor placement or, more commonly, in patients with a valgus deformity, previous laminectomy, or significant flexion contracture [23,24], which we were dealing with in this case. We are not aware of any specific guidelines on the correction of deformities and risk of nerve injury, as that is multifactorial and would be difficult to quantify. Knee rehabilitation presented more difficulties with psychological barriers and patient exhaustion after multiple surgeries in such a short period. Therapy progressed more slowly than expected. At the conclusion of rehabilitation, there was still a slight flexion contracture.
This case highlights the benefits of a logical and evidence-based approach to surgical planning and how a thoughtful rehabilitation protocol tailored to the patient’s complex needs can improve outcomes. Future research would benefit from more literature on AS on multiple joint takedowns and surgical techniques for addressing extreme flexion contractures. We reported on a 23-year-old male presenting with bilateral hip and knee autoarthrodesis, fixed in a seated position, secondary to progressive AS. To minimise the risk of complications, we addressed the patient’s hips before his knees to promote a focused recovery in rehab. The surgical treatment schedule consisted of four surgeries separated by approximately 8 weeks, along with continuous physical therapy. The progressive improvement in mobility and quality of life, as portrayed by the substantial increases in HOOS, HHS, and KOOS scores, reflects the success of the staged surgical approach and an individualized rehabilitation plan. Prior to the intervention, the patient was completely unable to move his legs and relied on either a wheelchair or the assistance of a caretaker for daily activities. Following the surgeries, he can now walk with the aid of a walker and perform daily tasks independently. In addition, he has experienced improved mobility, allowing him to sleep on his back for the first time in years. Such quality-of-life improvements can significantly enhance both the mental and physical health of affected individuals, particularly in young patients with severe mobility limitations who have many years ahead of them. At the most recent follow-up, approximately 1 year after the initial surgery, the patient is functionally ambulatory and gainfully employed.
- When approaching challenging cases, maintain a realistic expectation for improvement based on literature outcomes. These cases may result in a final ROM that is less than expected for a primary arthroplasty for osteoarthritis. Be sure to communicate these limitations clearly to the patient and caregivers, to allow for informed decision-making and post-operative management
- Addressing bilateral joint issues requires careful planning to mitigate post-operative rehabilitation difficulties. After the first surgery, the persistent disability in the remaining joint can significantly impact recovery by hindering mobility and strengthening exercises
- When encountering cases with significant initial flexion contractures, carefully assess the risk of stretching the peroneal nerve. While a more aggressive releasing technique may allow for increased extension, it is crucial to weigh the benefits against the substantial risk of peroneal nerve palsy.
References
- 1. Wenker KJ, Quint JM. Ankylosing Spondylitis. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. [Google Scholar] [PubMed]
- 2. Murphy SN, Nguyen BA, Singh R, Brown NJ, Shahrestani S, Neal MT, et al. A brief human history of ankylosing spondylitis: A scoping review of pathogenesis, diagnosis, and treatment. Surg Neurol Int 2022;13:297. [Google Scholar] [PubMed]
- 3. Miller TL, Cass N, Siegel C. Ankylosing spondylitis in an athlete with chronic sacroiliac joint pain. Orthopedics 2014;37:e207-10. [Google Scholar] [PubMed]
- 4. Haroon N. Ankylosis in ankylosing spondylitis: Current concepts. Clin Rheumatol 2015;34:1003-7. [Google Scholar] [PubMed]
- 5. Schett G, Rudwaleit M. Can we stop progression of ankylosing spondylitis? Best Pract Res Clin Rheumatol 2010;24:363-71. [Google Scholar] [PubMed]
- 6. Lories RJ, Schett G. Pathophysiology of new bone formation and ankylosis in spondyloarthritis. Rheum Dis Clin North Am 2012;38:555-67. [Google Scholar] [PubMed]
- 7. Oommen AT, Hariharan TD, Chandy VJ, Poonnoose PM, Arun Shankar A, Kuruvilla RS, et al. Total hip arthroplasty in fused hips with spine stiffness in ankylosing spondylitis. World J Orthop 2021;12:970-82. [Google Scholar] [PubMed]
- 8. Ward MM. Increased rates of both knee and hip arthroplasties in older patients with ankylosing spondylitis. J Rheumatol 2019;46:31-7. [Google Scholar] [PubMed]
- 9. Nilsdotter AK, Lohmander LS, Klässbo M, Roos EM. Hip disability and osteoarthritis outcome score (HOOS)–validity and responsiveness in total hip replacement. BMC Musculoskelet Disord 2003;4:10. [Google Scholar] [PubMed]
- 10. Söderman P, Malchau H. Is the Harris hip score system useful to study the outcome of total hip replacement? Clin Orthop Relat Res 2001;384:189-97. [Google Scholar] [PubMed]
- 11. Roos EM, Lohmander LS. The knee injury and osteoarthritis outcome score (KOOS): From joint injury to osteoarthritis. Health Qual Life Outcomes 2003;1:64. [Google Scholar] [PubMed]
- 12. Collins NJ, Prinsen CA, Christensen R, Bartels EM, Terwee CB, Roos EM. Knee Injury and osteoarthritis outcome score (KOOS): Systematic review and meta-analysis of measurement properties. Osteoarthritis Cartilage 2016;24:1317-29. [Google Scholar] [PubMed]
- 13. Parvizi J, Duffy GP, Trousdale RT. Total knee arthroplasty in patients with ankylosing spondylitis. J Bone Joint Surg Am 2001;83:1312-6. [Google Scholar] [PubMed]
- 14. Jauregui JJ, Buitrago CA, Pushilin SA, Browning BB, Mulchandani NB, Maheshwari AV. Conversion of a surgically arthrodesed knee to a total knee arthroplasty-is it worth it? A meta-analysis. J Arthroplasty 2016;31:1736-41. [Google Scholar] [PubMed]
- 15. Jauregui JJ, Kim JK, Shield WP 3rd, Harb M, Illical EM, Adib F, et al. Hip fusion takedown to a total hip arthroplasty-is it worth it? A systematic review. Int orthop 2017;41:1535-42. [Google Scholar] [PubMed]
- 16. Ahlbäck SO, Lindahl O. Hip arthrodesis. The connection between function and position. Acta Orthop Scand 1966;37:77-87. [Google Scholar] [PubMed]
- 17. Wood JH, Conway JD. Advanced concepts in knee arthrodesis. World J Orthop 2015;6:202-10. [Google Scholar] [PubMed]
- 18. Conway JD, Mont MA, Bezwada HP. Arthrodesis of the knee. J Bone Joint Surg Am 2004;86:835-48. [Google Scholar] [PubMed]
- 19. Simmons C Jr., Izant TH, Rothman RH, Booth RE Jr., Balderston RA. Femoral neuropathy following total hip arthroplasty: Anatomic study, case reports, and literature review. J Arthroplasty 1991;6:S59-66. [Google Scholar] [PubMed]
- 20. DeHart MM, Riley LH Jr. Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg 1999;7:101-11. [Google Scholar] [PubMed]
- 21. Fleischman AN, Rothman RH, Parvizi J. Femoral nerve palsy following total hip arthroplasty: Incidence and course of recovery. J Arthroplasty 2018;33:1194-9. [Google Scholar] [PubMed]
- 22. Carender CN, Bedard NA, An Q, Brown TS. Common peroneal nerve injury and recovery after total knee arthroplasty: A systematic review. Arthroplast Today 2020;6:662-7. [Google Scholar] [PubMed]
- 23. Park JH, Restrepo C, Norton R, Mandel S, Sharkey PF, Parvizi J. Common peroneal nerve palsy following total knee arthroplasty: Prognostic factors and course of recovery. J Arthroplasty 2013;28:1538-42. [Google Scholar] [PubMed]
- 24. Idusuyi OB, Morrey BF. Peroneal nerve palsy after total knee arthroplasty. Assessment of predisposing and prognostic factors. J Bone Joint Surg Am 1996;78:177-84 [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Lumbar Hyperextension Fracture after Direct Anterior Total Hip Arthroplasty
January 1, 2026 Lumbar Hyperextension Fracture after Direct Anterior Total Hip Arthroplasty August 1, 2025 Elbow Interpositional Arthroplasty using an Achilles Tendon Allograft: A Case Report
August 1, 2025 Elbow Interpositional Arthroplasty using an Achilles Tendon Allograft: A Case Report October 1, 2024 Co-existing Ankylosing Spondylitis and Rheumatoid Arthritis in a Patient Undergoing Total Knee Arthroplasty Under Peripheral Nerve Blocks
October 1, 2024 Co-existing Ankylosing Spondylitis and Rheumatoid Arthritis in a Patient Undergoing Total Knee Arthroplasty Under Peripheral Nerve Blocks July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report
July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report