
Aneurysmal bone cysts with atypical age, location, or imaging features require thorough metabolic workup and close radiology–pathology correlation, with biopsy and frozen section used to guide site-specific treatment and avoid misdiagnosis of more aggressive lesions.
Dr. Shravani Jagadabi, Department of Orthopaedics, Nizams Institute of Medical Sciences, Hyderabad, Telangana, India. E-mail: jagadabishravani@gmail.com
Abstract
Introduction: To describe the clinical, radiological, and histopathological spectrum of aneurysmal bone cysts (ABC) with unusual presentations and to highlight diagnostic pitfalls and management challenges in these patients.
Materials and Methods: This ambispective study included 20 cases with ABC or ABC-mimicking lesions treated between March 2022 and November 2024 at a tertiary care hospital. Patients were eligible if they had at least one atypical feature. These included uncommon age, rare anatomical location, atypical radiological appearance suggesting alternative diagnoses (including sarcoma), or an inconclusive biopsy report. All patients underwent standardized clinical, radiological, and histopathological evaluations. Selective use of core/open biopsies and intraoperative frozen sections was included. Management was tailored to site- and lesion-specific factors.
Results: Of 20 cases, 11 were males, and 9 were females, with a mean age of 20.3 years (range 5–45 years); most patients were younger than 10 years or older than 30 years, which is outside the usual second-decade peak for ABC. Lesions affected multiple rare sites, including the shaft of the ulna, glenoid, acetabulum, talus, calcaneum, metatarsal, clavicle, wing of the sphenoid, rib, and neck of the femur. Radiological imaging suggested ABC in 13 patients, but alternative diagnoses such as sarcoma, giant cell tumor, fibrous dysplasia, and Brown’s tumor were reported in the remainder, and the final histopathology confirmed a range of entities, including primary and solid variant ABC, simple bone cyst, chondroblastoma, fibrous dysplasia, and osteoclast-rich lesion secondary to Vitamin D deficiency. Most patients were treated with intralesional polidocanol injection and extended curettage with an allogenic bone graft, whereas a few underwent wide resection or adjuvant denosumab; over a mean follow-up of 15 months, one patient developed recurrence after curettage, and one presented with a pathological fracture.
Conclusion: ABCs with unusual age, location, or non-typical imaging and biopsy findings can closely mimic more aggressive pathologies and complicate decision-making. Systematic metabolic evaluation, careful correlation of radiology with core or open biopsy and intraoperative frozen section, and tailoring of treatment to site, size, and confirmed pathology can improve diagnostic accuracy and optimise outcomes in such challenging cases.
Keywords: Aneurysmal bone cyst, unusual presentation, polidocanol, extended curettage, allogenic bone graft.
An aneurysmal bone cyst (ABC) is a rare, benign yet locally aggressive, expansile osteolytic lesion characterized by blood-filled cystic spaces lined by fibroblasts, osteoclast-like giant cells, and reactive bone formation, typically affecting the metaphysis of long bones or spine in adolescents [1]. It typically affects the metaphysis of long bones in young patients during their second decade of life [2]. Although benign, it can be locally aggressive. Radiological features can mimic both benign and malignant tumors [3]. Radiologically, these manifest as eccentric, lytic, expansile lesions with fluid-fluid levels on magnetic resonance imaging (MRI) [4,5], though atypical features such as absent cystic components, marked sclerosis, or solid architecture in solid ABC raise differentials such as giant cell tumour (GCT), telangiectatic osteosarcoma, or fibrous dysplasia. Histopathologically, conventional ABC shows cavernous spaces with hemorrhagic septa containing giant cells [6], whereas solid ABC displays fibroblastic stroma with scattered osteoclastic giant cells and focal osteoid devoid of atypia [7], as confirmed by the absence of malignant cells. Management prioritizes intralesional injection of polidocanol [8], extended curettage with adjuvants (high-speed burr, phenol, cryotherapy, polymethylmethacrylate) [5], and bone grafting to address a 20–30% recurrence risk, particularly in weight-bearing sites such as the proximal femur, where prophylactic fixation (e.g., dynamic hip screw plating) [9] ensures stability. En bloc resection is suitable for accessible sites, such as ribs or clavicles, for achieving curative outcomes. New options include percutaneous sclerotherapy (polidocanol), denosumab for osteoclast suppression [10], and pre-operative embolization for vascular lesions.
This study examined patients both going forward and looking back in time, including 20 people with ABC or growths that appeared to be ABCs, treated between March 2022 and November 2024 at Nizam’s Institute of Medical Sciences, Hyderabad. Approval from the Ethics Committee EC/NIMS/3727/2025(A), held on August 07, 2025, was obtained before the start of the study. Informed consent or waiver of consent was obtained from all the patients before the study. We included patients who had cyst-like bone growths and met at least one unusual feature: having a rare presentation such as a lump or broken bone, especially at an uncommon age; a cyst in a bone location that is not typical for ABC; scan findings that suggested other possible conditions, especially cancer or giant cell tumour; or tissue tests that showed another condition or could not rule out something more serious. The initial evaluation included detailed history, clinical examination, and baseline laboratory investigations, including a metabolic profile. Radiological workup consisted primarily of plain radiographs, with computed tomography, MRI, and bone scan used selectively to further characterize the lesions and plan treatment.
A core needle or open biopsy was performed at the site, and based on radiological suspicion, an intraoperative frozen section was routinely used before proceeding with definitive intralesional procedures. Treatment decisions were planned based on site, size, and histopathological diagnosis. Treatment options included intralesional polidocanol injection, extended curettage with or without adjuvant therapy, allogenic bone grafting, wide resection with or without reconstruction, and adjuvant denosumab in certain aggressive lesions. Patients were followed up clinically and radiologically at regular intervals. The assessment included pain relief, functional outcome, radiological healing, and recurrence or complications such as pathological fracture. The minimum follow-up was 12 months, and the maximum exceeded 30 months.
A total of 20 patients met the inclusion criteria of having one or more unusual features of ABC. There were 11 males and 9 females, with a mean age of 20.3 years (range 5–45 years). Four patients were younger than 10 years old, and two were older than 45 years old. The remainder were between 20 and 40 years old, which is outside the typical second-decade peak in ABC occurrence, with localized pain alone. Six presented with a palpable mass and pain. Two presented with only swelling. Two had a pathological fracture as the initial manifestation, and two were unable to walk due to severe pain. Lesions involved both long and flat bones; rare flat-bone sites included the acetabulum, ribs, sphenoid wing, glenoid notch of the scapula, calcaneus, talus, metatarsals, and iliac bones. Among long bone lesions, about half (11/20) were confined to the metaphysis, but one patient had an ulnar diaphyseal lesion (cortical ABC) extending into surrounding soft tissue, and one lesion was in the clavicle, as shown in Fig. 1.
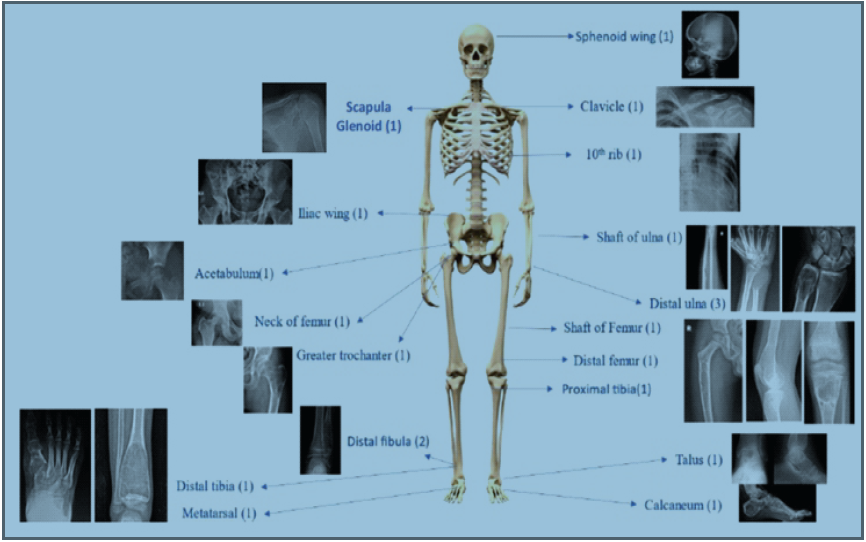
Figure 1: Distribution based on anatomical site, with the respective radiographs containing the lesion.
Radiological evaluation suggested ABC as the primary diagnosis in 14 of 20 patients. Alternative primary radiological diagnoses included Gorham’s disease/ABC in one patient, sarcoma in one, and GCT in two (distal femur and distal ulna). One patient had a differential of GCT/plasmacytoma at the neck of the femur and Ewing’s sarcoma for a cortical-based lesion in the shaft of the ulna. Overall, final pathological diagnoses included primary and solid variant ABC in the majority, with individual cases of chondroblastoma, simple bone cyst, fibrous dysplasia, and osteoclast-rich giant cell lesion secondary to Vitamin D deficiency as shown in figure 2. In seven patients, no pre-operative biopsy was performed; however, an intraoperative frozen section was used in all patients before proceeding with intralesional injection or curettage (Fig. 2, 3 and 4).
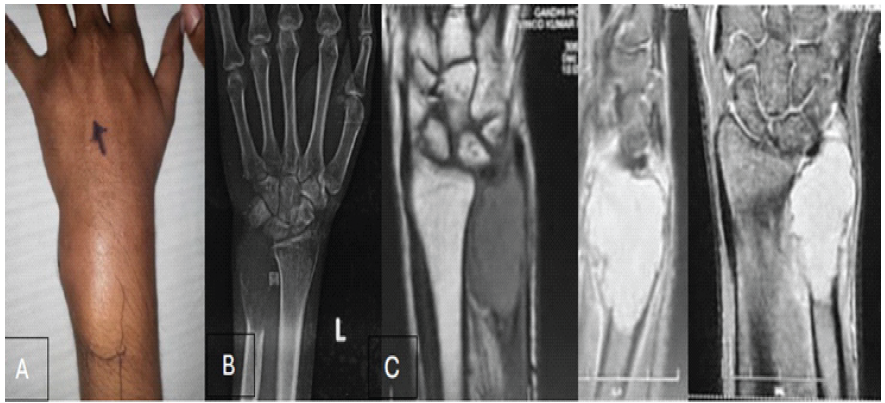
Figure 2: A 28-year-old male with a solid variant of aneurysmal bone cyst/H3.3G34W negative giant cell tumor (GCT) of distal ulna on core biopsy, treated with tumor resection, turned out to be a lesion due to secondary hyperparathyroidism due to severe vitamin deficiency. On parathyroid scintigraphy, mild uptake was seen in the left inferior parathyroid. (Pre-operative serum calcium – 8.9 mg/dL, Vitamin D – 10.50 ng/mL, serum parathyroid hormone-52.1 pg/mL, Serum phosphorus – 2.7 mg/dL, serum magnesium – 0.84 mg/dL). (A) Clinical image, (B) Radiograph at presentation, (C) Magnetic resonance imaging images showing T1 isointense, T2 coronal and sagittal sections with hyperintense lesion, features consistent with GCT.
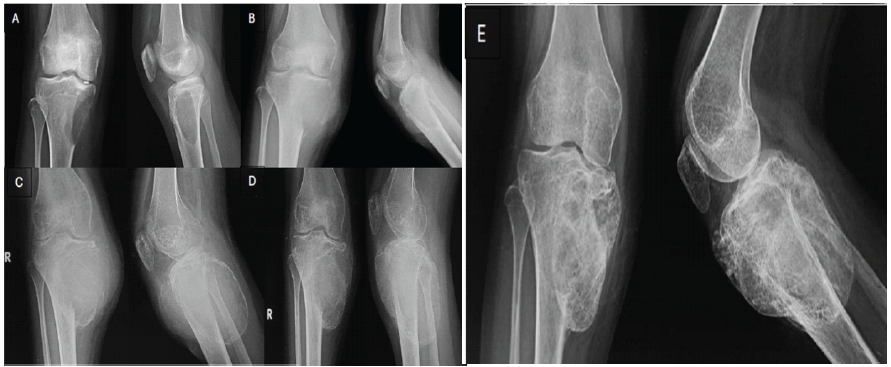
Figure 3: Radiographs of the right knee of a 15-year-old child with aggressive aneurysmal bone cysts in the proximal tibia treated with intra-lesional injection of polidocanol. (A) At presentation, (B) At 1 month following treatment with intralesional polidocanol, (C) 6 weeks following treatment, the lesion consolidated well and marked sclerosis was observed, (D) Increase in size of lesion noted, so embolization + intralesional polidocanol injection was given, (E)
6 weeks follow-up radiograph after embolization and intralesional polidocanol injection.
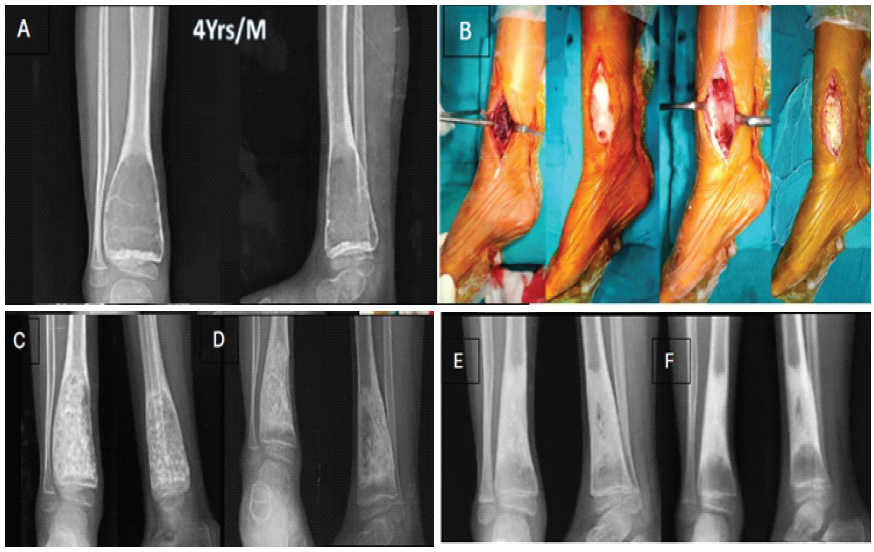
Figure 4: A 4-year-old child with an aneurysmal bone cyst in the distal tibia treated with extended curettage and allogenic bone grafting. (A) Pre-operative radiograph with the lesion encroaching the growth plate, (B) Intraoperative images showing extended curettage + hydrogen peroxide, and allogenic bone grafting, (C,D,E,F ) post-operative follow-up radiographs at 6 weeks, 6 months, 15 months, and 24 months, respectively.
Biopsy techniques included core needle biopsy in 13 patients and open biopsy in 2; the core biopsy established the diagnosis in 10 patients but was inadequate in 3. As for treatment, wide resection was performed in 1 patient with distal ulnar ABC, whereas the remaining patients underwent intralesional polidocanol injection (Fig. 3) and/or extended curettage with adjuvants and allogenic bone grafting (Fig. 4). No adjuvants were used after curettage in five patients. One patient with an aggressive lesion in the neck of the femur, on core needle biopsy, suggested a benign giant cell-rich lesion, favouring an ABC or H3F3A.G34W-negative, H3.3K36M-negative giant cell tumor, received three doses of denosumab 120 mg before tumor resection (Fig. 5).
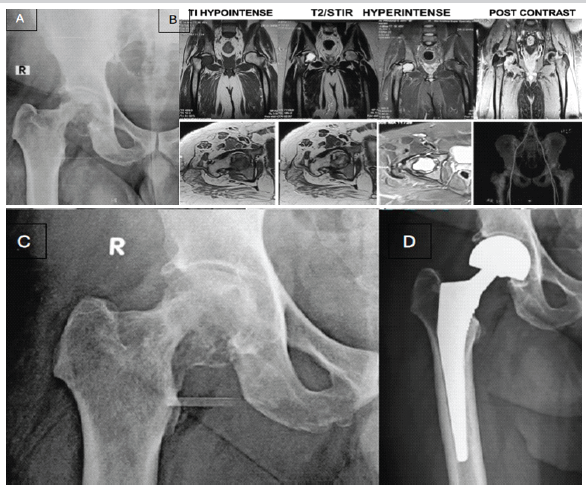
Figure 5: A lesion in a 45-year-old male at the neck of the femur treated with tumor resection + hemiarthroplasty. Core needle biopsy suggested a benign giant cell-rich lesion, favoring aneurysmal bone cyst or H3F3A.G34W negative, H3.3K36M negative giant cell tumor; however, in view of unusual age and site, H3F3A.G34W negative giant cell tumor (GCT) with secondary aneurysmal changes cannot be ruled out. (A ) At presentation, radiograph, ( B ) Magnetic resonance imaging features suggesting GCT with secondary aneurysmal bone cysts/Plasmacytoma, (C ) Radiograph after giving injection of denosumab 3 weekly doses (120mEq each), ( D ) Post-operative radiograph.
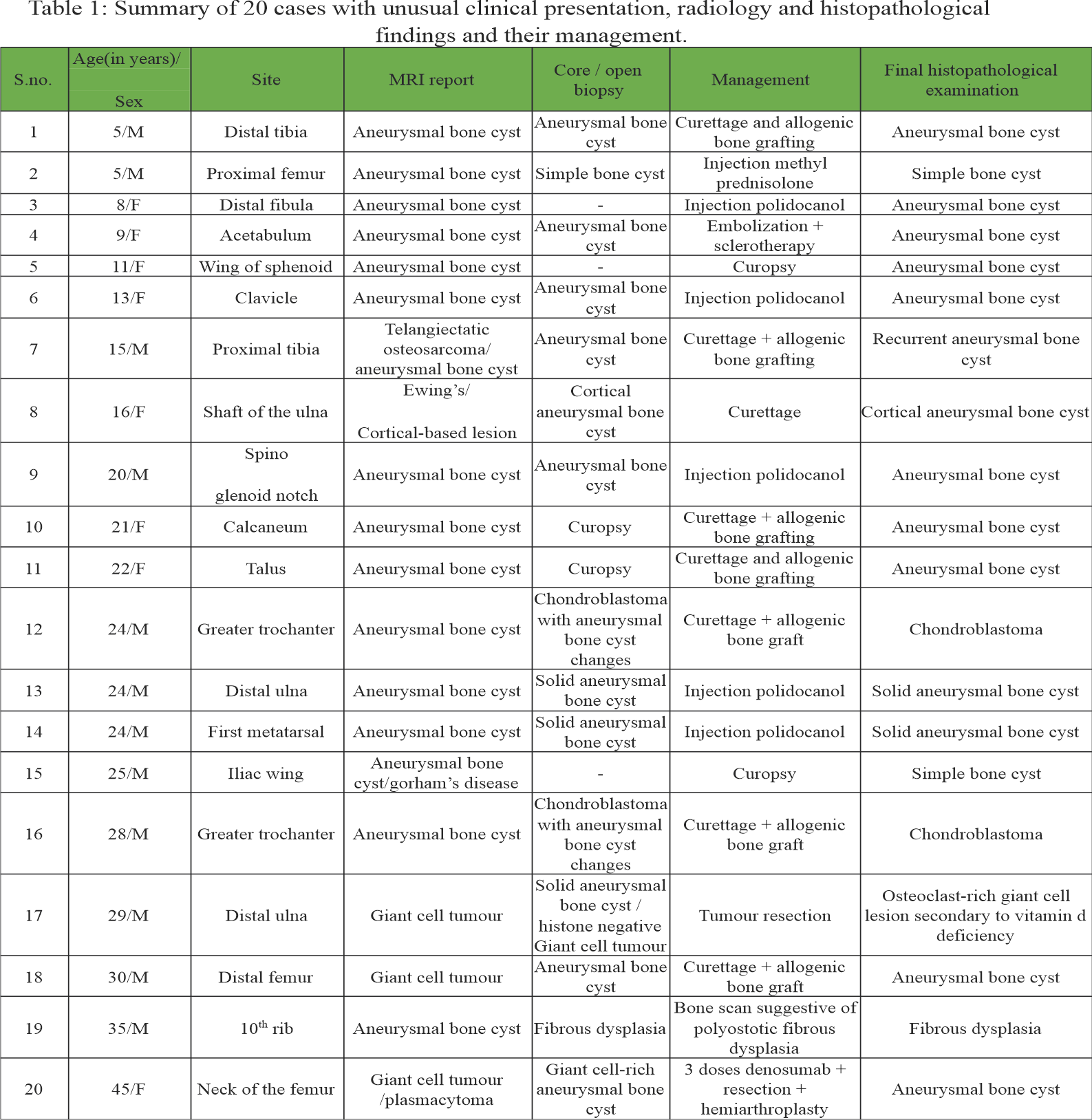
A follow-up period ranged from a minimum of 12 months to more than 30 months. No recurrences were observed in patients treated with wide resection, whereas 1 of 20 patients treated with extended curettage and bone grafting developed recurrence, and 1 patient presented with a pathological fracture during follow-up. A summary of 20 cases with unusual clinical presentation, radiology, and histopathological findings and their management is shown in Table 1.
This study highlights the diverse presentations of ABCs, often involving atypical age, site, radiological, or histopathological findings. Patients were predominantly under 10 or over 40 years old, deviating from the typical second-decade incidence, which heightens diagnostic challenges. Literature echoes this with cases such as a 55-year-old woman with distal ulna ABC [11] and a 51-year-old male with third-rib involvement. The series further reveals ABCs in uncommon locations, including the ulnar shaft, glenoid, acetabulum, talus, calcaneus, metatarsals, clavicle, sphenoid wing, rib, and femoral neck, where they commonly mimic aggressive benign or malignant tumors. Imaging was frequently inconclusive, with initial interpretations favouring sarcoma, GCT, or fibrous dysplasia over ABC. A major observation from this study is the potential mismatch between initial radiology, biopsy results, and definitive histopathology in atypical ABC presentations. For instance, one lesion provisionally identified as solid-variant ABC proved to be a giant cell-rich lesion secondary to Vitamin D deficiency; others initially deemed to be simple bone cysts later recurred as ABCs; and some showed features overlapping with chondroblastoma or GCT. These findings stress the importance of integrating imaging with metabolic assessments, pursuing repeat or open biopsies as needed, and using intraoperative frozen sections before definitive surgery. Comparable discrepancies appear in the literature [12]. From a treatment perspective, most patients in this series achieved success with intralesional polidocanol sclerotherapy or extended curettage (with or without adjuvant therapy and allogeneic bone grafting), limiting wide resection and reconstruction to specific cases such as distal ulnar lesions, the neck of the femur, or highly aggressive disease. Similarly, a series of 72 patients managed with percutaneous polidocanol injections reported a 97% cure rate [13]. This series demonstrated a low recurrence rate – no cases after wide resection and only one following curettage, indicating that thorough lesion excision, with precise diagnosis, yields lasting control even for atypical ABCs. While en bloc resection offers superior local control, it risks complications tied to surgical extent, such as bleeding, pain, and growth disturbances [14,15]. Such approaches often create bone defects requiring reconstruction, which proves challenging based on location. Flont et al. noted non-significantly higher recurrence rates with en bloc resection compared to curettage [14,16]. Administering denosumab for one aggressive, giant cell-rich lesion highlights the emerging utility of targeted biologics as adjuncts in difficult ABC cases. At the molecular level, ABCs have osteoclast-like multinucleated giant cells with elevated receptor activator nuclear factor receptor expression and stromal cells with high receptor activator nuclear factor-κB ligand (RANKL) levels. Denosumab, a monoclonal antibody against RANKL, is Food and Drug Administration-approved for GCT of bone (GCTB) in adults and skeletally mature adolescents when surgery is infeasible. Although not FDA-approved for ABCs, clinicians have reasonably applied it off-label in select cases, given the morphological overlap between GCTB and ABC [17]. Overall, these findings support a structured approach that integrates clinical suspicion, detailed imaging, metabolic profiling, and staged histopathological confirmation to differentiate ABC from its numerous mimics. Such an approach allows treatment to be tailored to site, size, and biological behaviour, thereby minimizing both under-treatment of potentially aggressive lesions and over-treatment of benign lesions that are assumed to be malignant.
An ABC with an unusual age distribution, rare anatomical locations, and non-typical radiological or histopathological features poses significant diagnostic and therapeutic challenges. A detailed metabolic assessment, careful radiological and pathological correlation with liberal use of either core biopsy or open biopsy and intraoperative frozen section, and site-specific management strategies are essential to achieve accurate diagnoses and favourable long-term prognostic outcomes in these complex cases.
Atypical ABCs challenge standard paradigms; however, multidisciplinary correlation and tailored pathology-driven management mitigate misdiagnosis risks and improve results.
References
- 1. Vergel De Dios AM, Bond JR, Shives TC, McLeod RA, Unni KK. Aneurysmal bone cyst. A clinicopathologic study of 238 cases. Cancer 1992;69:2921-31. [Google Scholar] [PubMed]
- 2. Park HY, Yang SK, Sheppard WL, Hegde V, Zoller SD, Nelson SD, et al. Current management of aneurysmal bone cysts. Curr Rev Musculoskelet Med 2016;9:435-44. [Google Scholar] [PubMed]
- 3. Mankin HJ, Hornicek FJ, Ortiz-Cruz E, Villafuerte J, Gebhardt MC. Aneurysmal bone cyst: A review of 150 patients. J Clin Oncol 2005;23:6756-62. [Google Scholar] [PubMed]
- 4. Grahneis F, Klein A, Baur-Melnyk A, Knösel T, Birkenmaier C, Jansson V, et al. Aneurysmal bone cyst: A review of 65 patients. J Bone Oncol 2019;18:100255. [Google Scholar] [PubMed]
- 5. Van Geloven TP, Van Den Boom AL, Schaap GR, Jutte PC, Bramer JA. The treatment of aneurysmal bone cysts. EFORT Open Rev 2022;7:892-904. [Google Scholar] [PubMed]
- 6. Reddy KI, Sinnaeve F, Gaston CL, Grimer RJ, Carter SR, Tillman RM, et al. Aneurysmal bone cysts: A review of 150 patients. Bone Joint J 2014;96-B:1141-6. [Google Scholar] [PubMed]
- 7. Mittal S, Kalia V, Dhamija E, Rastogi S, Kumar R, Singh P, et al. Solid variant of aneurysmal bone cyst presenting as a giant cervical mass. Surg Neurol Int 2016;7 Suppl 36:S873-7. [Google Scholar] [PubMed]
- 8. Rajak A, Pathak A, Swami A, Varma A. Is an intralesional approach a sufficient treatment for solid variants of aneurysmal bone cysts? J Surg Med 2020;4:784-9. [Google Scholar] [PubMed]
- 9. Jadhav AB, Bansal M, Suryawanshi KH, Dube A. Management of proximal femur aneurysmal bone cyst with 10-year follow-up: A case report. J Orthop Case Rep 2024;14:1-5. [Google Scholar] [PubMed]
- 10. Ntalos D, Priemel M, Schlickewei C, Thiesen DM, Rueger JM, Spiro AS. Therapeutic management of a substantial pelvic aneurysmatic bone cyst including the off-label use of denosumab in a 35-year-old female patient. Case Rep Orthop 2017;2017:9125493. [Google Scholar] [PubMed]
- 11. Jain M, Pradhan SS, Khan S, Tripathy S, Lubaib KP, Raj KS. Aneurysmal bone cyst of the distal ulna in an elderly lady. J Orthop Case Rep 2024;14:79-83. [Google Scholar] [PubMed]
- 12. Khan JA, Saleh T, Shafqat A, Albalkhi I, Saleh W. Unusual presentation of an aneurysmal bone cyst: A case report and literature review. Radiol Case Rep 2023;18:1320-3. [Google Scholar] [PubMed]
- 13. Rastogi S, Varshney MK, Trikha V, Khan SA, Choudhury B, Safaya R. Treatment of aneurysmal bone cysts with percutaneous sclerotherapy using polidocanol. A review of 72 cases with long-term follow-up. J Bone Joint Surg Br 2006;88:1212-6. [Google Scholar] [PubMed]
- 14. Tsagozis P, Brosjö O. Current strategies for the treatment of aneurysmal bone cysts. Orthop Rev (Pavia) 2015;7:6182. [Google Scholar] [PubMed]
- 15. Farsetti P, Tudisco C, Rosa M, Pentimalli G, Ippolito E. Aneurysmal bone cyst. Long-term follow-up of 20 cases. Arch Orthop Trauma Surg 1990;109:221-3. [Google Scholar] [PubMed]
- 16. Flont P, Kolacinska-Flont M, Niedzielski K. A comparison of cyst wall curettage and en bloc excision in the treatment of aneurysmal bone cysts. World J Surg Oncol 2013;11:109. [Google Scholar] [PubMed]
- 17. Imre A, Zoltán S, Miklós S. Current indications for denosumab in benign bone tumours. EFORT Open Rev 2023;8:895-905. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Aneurysmal Bone Cyst of Talus: Case Report of a Rare Presentation
January 1, 2026 Aneurysmal Bone Cyst of Talus: Case Report of a Rare Presentation July 1, 2025 Twenty-Four-Year Follow-up of Successful Total Hip Arthroplasty for Recurrent Proximal Femoral Aneurysmal Bone Cyst with a Pathologic Fracture Following Extended Curettage and Bone Grafting: A Case Report
July 1, 2025 Twenty-Four-Year Follow-up of Successful Total Hip Arthroplasty for Recurrent Proximal Femoral Aneurysmal Bone Cyst with a Pathologic Fracture Following Extended Curettage and Bone Grafting: A Case Report January 10, 2021 A Rare Case of Aneurysmal Bone Cyst – Navicular Bone Treated by Intralesional Sclerotherapy Agent Polidocanol
January 10, 2021 A Rare Case of Aneurysmal Bone Cyst – Navicular Bone Treated by Intralesional Sclerotherapy Agent Polidocanol July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report
July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report