
Trapezium fractures presentation and treatment.
Dr. Gabriel Pina,
Department of Orthopaedics and Traumatology,
Centro Hospitalar Tondela-Viseu, Viseu Dão Lafões, Portugal.
E-mail: gabrielpina950hotmail.com
Introduction: Trapezium fracture is a rare entity whose treatment is controversial. The reported cases range from conservative treatment to surgical treatment with good reported results.
Case Report: This paper reports a clinical case of trapezium-metacarpal fracture-dislocation associated with trapezius fracture and Bennett fracture, surgically treated with excellent functional and radiological results. The patient underwent open reduction and internal fixation with two screws, excision of fragments, and reinsertion of the anterior oblique ligament. At the year of follow-up, the patient presented no mobility limitations and recovered grip strength.
Conclusion: This case study allows us to conclude that open reduction and internal fixation with screws of the dorsal trapezium ridge fractures with ligament repair of the anterior oblique ligament is a valid treatment with the reproduction of good clinical results.
Keywords: Hand surgery, internal fixation, trapezium fracture.
The trapezium is a carpal bone that integrates the trapezium-metacarpal joint, a joint that plays an essential role in the grip and grasping function [1]. Fracture of this bone is rare, accounting for about 0.4% of hand injuries and about 3% of carpal injuries [1, 2]. Most trapezium fractures are fractures with a vertical orientation at the dorsal edge or body [3]. This type of fracture may be associated with other associated injuries, namely, Bennett fracture, Rolando fracture, scaphoid fracture, other metacarpal fracture, distal radius fracture, and trapezium-metacarpal dislocations [4, 5, 6]. The injury mechanism is a high-energy trauma, and 50% of the reported cases are related to motorcycle falls [4, 7]. The treatment is controversial, since the literature on these lesions is scarce. The reported cases range from conservative treatment, closed reductions and Kirschner wire fixation, and open reductions and internal screw fixation, with good results reported in all these methods [8]. The aim of this paper is to report a case of trapezium-metacarpal fracture-dislocation associated with trapezium fracture and Bennett fracture, treated surgically with excellent functional and radiological results, as well as to review the literature on this pathology. The patient consent was obtained.
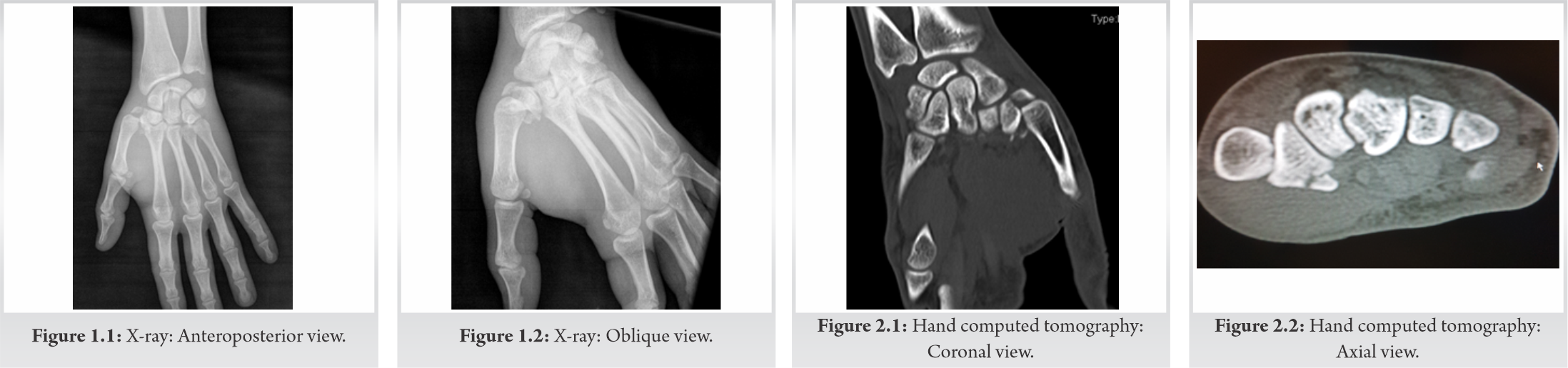
Male patient, right-handed student, 24 years old, admitted to the emergency department after a motorcycle accident with left thumb monotrauma. Clinically, presented edema, pain on palpation and mobilization, referred to the base of the thumb, without wounds, or associated neurovascular deficits. Radiographic study was performed (Fig. 1.1, 1.2), which revealed a fracture, with a deviation>2 mm, from the vertical dorsal trapezium edge fracture with more than 2mm deviation and a volar tubercle fracture without deviation, corresponding type IIb, and type III Walker fracture, respectively. A comminuted Bennett fracture with associated trapezium-metacarpal dislocation was also diagnosed. This lesion was then subjected to computed tomography (CT) evaluation (Fig. 2.1, 2.2) for a better characterization of the fracture pattern with regard to joint deviation, number and size of fragments, and their respective spatial orientation.
In the emergency department, dislocation closed reduction and temporary plaster cast immobilization were performed and surgical intervention was proposed. The patient underwent surgery 3 days after the trauma. A dorsal radial approach was used and identification and protection of the superficial radial nerve and radial artery branches were performed. Trapezium-metacarpal capsulotomy was performed. Anatomical trapezium fracture reduction was performed and fixed temporarily with Kirschner wire and definitively with two 1.5mm screws (Bone Care-Medartis). By the same approach, Bennett fracture fragments were excised and anterior oblique ligament was reinserted with 2.8mm mini-anchor (Twinfix). Finally, transarticular stabilization of the trapezium-metacarpal joint with Kirschner wire was performed to protect ligament repair. A cast immobilization was performed (Fig. 3).

Postoperatively, there were no complications. At 2 weeks postoperatively, the surgical wound was healed, and suture was removed as well as the cast immobilization. At 6 weeks, the Kirschner wire was removed and rehabilitation started. At follow-up, he presented no range of motion limitations, except slight loss of adduction. Full grip strength recovery was observed, corresponding to a final Quick-DASH score of 3.5 (0–100). The patient returned to his normal life activities without limitations (Fig. 4.1-4.3). Radiographically, no fracture loss of fixation, reduction, or articular instability was observed during follow-up. Fracture healing and joint congruence without signs of osteoarthritis were observed after 1 year of follow-up (Fig. 5.1, 5.2).

Most trapezium fractures are dorsal ridgeoriented vertical fractures, Walker type IIa and IIb fractures, or Walker type IV body fractures [8,9]. Walker, however, further described volar tubercle (type III) fractures, horizontally oriented (type I) and comminuted (type V) body fractures [9] (Fig. 6). As far as our case is concerned, this is a dorsal ridge fracture with a deviation >2 mm, therefore Walker type IIb, associated with a non-deviated volar tubercle fracture, Walker type III. This combined pattern is not described in the scientific literature. Trapezium fractures are already a rare entity [2], but their association with trapezium-metacarpal dislocation and Bennett’s fracture is even less frequent [4], which makes this case even more particular, given its pattern of injury. Regarding the mechanism of injury, there is no consensus on the exact mechanism. High-energy trauma with direct trauma at the first commissure or indirect axial loaded wrist trauma with radial deviation and hyperextension is mechanisms described and associated with comminuted and vertical fractures, respectively [8,10,11]. Motorcycle accidents have been associated throughout the literature as responsible for about 50% of cases of trapezium fracture [4]. This fact is associated with biomechanical studies, which related these fractures to direct trauma at the first commissure or indirect trauma, which allows correlating with the position of the hand on the motorcycle handlebar [12]. The rarity of this fracture makes its diagnosis more difficult, especially if the fracture is not deviated and if at least two orthogonal views, lateral and Robert view, are performed. The latter corresponds to the true base thumb anteroposterior (AP) view [13]. Sensitivity of plain radiographs may vary from 18% to 67%, depending on the number of views and image quality [11]. CT plays an essential role in the diagnosis of this type of fracture, when clinical suspicion associated with negative X-rays, as well as in the characterization of the number, size, deviation, and orientation of fracture fragments [14]. Treatment of such fractures continues without consensus. The rarity of the lesion is associated with a lack of literature, which makes the therapeutic orientation of these lesions variable. There is some consensus that fractures without deviation should be conservatively treated, with good reported results [8, 10, 15], and that fractures with a deviation >2 mm should be treated surgically [3, 4]. Less consensus exists on the type of surgical treatment to be performed. Reports of surgical treatment range from closed reduction and percutaneous fixation with Kirschner wires and open reduction and internal fixation with screws or Kirschner wires. These different types of treatment are all associated with excellent results throughout the literature [1, 2, 3, 4, 15, 16, 17, 18, 19, 20, 21]. Also described in the treatment of comminuted fractures, is the use of external fixation and button fixation, whose biomechanical objective is to maintain trapezius height while healing. Good clinical results are reported with both techniques [5, 22]. The purpose of closed reduction and percutaneous fixation with Kirschner wires is to fix and prevent reduction loss, as well as to promote axial discharge of the first metacarpal onto the trapezium in a mini-invasive manner. On the other hand, it requires the complementary use of cast immobilization [8, 17]. After fracture reduction and stabilization, joint stability needs to be assessed, which may be compromised by associated ligament injuries that may require repair [23]. In our case, the trapezium fracture was reduced and fixed with 2 screws, 1.5 mm. In addition to the trapezium fracture, a comminuted Bennett fracture with trapezium-metacarpal dorsal dislocation was associated, whose instability was associated with loss of stabilization promoted by the anterior oblique ligament. It was reinserted with 2.8 mm mini-anchor, with recovery of joint stability and excellent clinical reproduction. Panigrahi et al. reported a Walker type I fracture without deviation, treated with a cast, without final clinical limitations [15], similarly to Kose et al. [8] and Van Schiland De Smet [10] who also used conservative treatment on non-deviated fractures with good results. On the other hand, Jones et al. reported in three clinical cases the effect of non-anatomically reducing these fractures. Two cases were submitted to conservative treatment and showed significant loss of grip strength, as well as a high residual stiffness [24]. Kohyama et al. reported three cases of trapezium fracture, one Walker type V case treated with open reduction and Kirschner wire fixation, and two cases Walker type IV treated, with two screws with excellent results [20]. De Nigris et al. [17] obtained an excellent result in a case undergoing closed reduction and fixation with Kirschner wire. In a similar case, Ramoutar et al. after closed reduction and Kirschner wire fixation also reported an excellent result, as Suthersan and Chan who after open reduction and fixation with three screws and one transarticular Kirschner wire also obtained excellent results, although with slight abduction stiffness [2]. Martins et al. also achieved excellent clinical outcome with open reduction and fixation with a screw in a type IIA fracture. Shenouda et al. [5] and Pehlivan et al. [22] obtained excellent clinical results in their respective cases of comminuted trapezius fracture using a button system between the 1st and 2nd metacarpals and the use of an external fixator. Weisler et al. described a case of type IV fracture, percutaneously treated with a screw and arthroscopic fracture reduction support, with excellent end result [6]. McGuigan and Culptreated 11 cases of trapezius fracture surgically, ranging from closed reduction and fixation with Kirschner wires to open reduction and screw fixation in vertical split or comminuted fractures. Nine out of 11 patients were very pleased with the result (Table 1). There was no relationship between the end result and the type of fracture or the type of surgical treatment. They also observed that about 50% of the cases evolved to trapezium-metacarpal osteoarthritis despite a good joint reduction. It concludes that residual instabilities associated with ligament injuries could produce chronic instability with consequent evolution to arthritis [4]. In our case, trapezium-metacarpal joint instability was present in its major form, the dislocation. Its associated lesion was a Bennett fracture, leading to the loss of stabilizing function promoted by the anterior oblique ligament, major stabilizer of the trapezium-metacarpal [13]. Ligament reinsertion associated with joint stabilization with Kirschner wire allowed restoring ligament stability. At 1 year of follow-up, there was no evolution to arthritis.
This case study allows us to conclude that open reduction and internal fixation with screws of trapezium fractures is a valid treatment, with good results, allowing to combine the advantage of anatomical reduction and ligament repair.
Surgical treatment of displaced trapezium fracture is associated with excellent functional results.
References
- 1.Ramoutar DN, Katevu C, Titchener AG, Patel A. Trapezium fracture a common technique to fix a rare injury: A case report. Cases J 2009;2:8304. [Google Scholar]
- 2.Suthersan M, Chan S. Isolated comminuted fracture of the trapezium: A case report and review of the literature. Internet J Orthop Surg 2011;18:1-4. [Google Scholar]
- 3.Lee SK. Carpal injuries. Fractures of the carpal bones. In: Wolfe SW, Pederson W, Kozin S, Cohen M, editors. Green’s Operative Hand Surgery. 7th ed. Philadelphia, USA:Elsevier; 2017. p. 626. [Google Scholar]
- 4.McGuigan FX, Culp RW. Surgical treatment of intra-articular fractures of the trapezium. J Hand Surg Am 2002;27:697. [Google Scholar]
- 5.Shenouda ME, Mohan A, Sarkhel T. Using a tightRope® to treat a complex fracture of the trapezium. Ann R Coll Surg Engl 2014;96:e36-8. [Google Scholar]
- 6.Weisler E, Chloros G, Kuzma G. Arthroscopy in the treatment of fracture of the trapezium. Arthroscopy 2007;23:1248.e1-4. [Google Scholar]
- 7.Meng L, Zhang Y, Lu Y. Three-dimensional finite element analysis of mini-external fixation and Kirschner wire internal fixation in Bennett fracture treatment. Orthop Traumatol Surg Res 2013;99:21-9. [Google Scholar]
- 8.Kose O, Keskinbora M, Guler F. Carpometacarpal dislocation of the thumb associated with fracture of the trapezium. J Orthop Traumatol 2015;16:161-5. [Google Scholar]
- 9.Walker JL, Greene TL, Lunseth PA. Fractures of the body of the trapezium. J Orthop Trauma 1988;2:22-8. [Google Scholar]
- 10.Van Schil P, De Smet C. Simultaneous fracture of carpal scaphoid and trapezium. Br J Hand Surg 1986;11:112-4. [Google Scholar]
- 11.Balci A, Basara I, Çekdemir EY, Tetik F, Aktaş G, Acarer A, et al. Wrist fractures: Sensitivity of radiography, prevalenceand patterns in MCDT. Emerg Radiol 2015;22:251-6. [Google Scholar]
- 12.Pointu J, Schwenck JP, Destree G, Séjourné P. Fractures of the trapezium. Mechanisms. Anatomo-pathology and therapeutic indications. Rev Chir Orthop Reparatrice Appar Mot 1988;74:454-65. [Google Scholar]
- 13.Cannon DL. Wrist disorders. In: Campbell’s Operative Orthopaedics. 12th ed., Vol. 4. Amsterdam, Netherlands: Elsevier; 2016. p. 3383-476. [Google Scholar]
- 14.Horch R. A new method for treating isolated fractures of the os trapezium. Arch Orthop Trauma Surg 1998;117:180-2. [Google Scholar]
- 15.Panigrahi R, Biswal MR, Palo N, Panigrahi N. Isolated coronal fracture of trapezium a case report with review of literature. J Orthop Case Rep 2015;5:29-31. [Google Scholar]
- 16.Garneti N, Tuson CE. Sagittally split fracture of trapezium associated with subluxed carpo-metacarpal joint of thumb. Injury 2004;35:1172-5. [Google Scholar]
- 17.De Nigris G, Falzarano G, et al. A rare case of isolated trapezium fracture in motorcycle polytrauma patient in emergency department. J Acute Dis 2016;5:252-4. [Google Scholar]
- 18.Cordrey LJ, Ferrer-Torrells M. Management of fractures of the greater multangular. J Bone Joint Surg 1960;42A:1111-8. [Google Scholar]
- 19.Foster RJ, Hastings H., II Treatment of Bennett, Rolando and vertical intraarticular trapezial fractures. Clin Orthop. 1987;214:121–129. [Google Scholar]
- 20.Kohyama S, Tanaka T, Ikumi A, Totoki Y, Okuno K, Ochiai N. Trapezium fracture associated with thumb carpometacarpal joint dislocation: A report of three cases and literature review. Case Rep Orthop 2018;2018:2408708. [Google Scholar]
- 21.Martins I, Vasques A, Pereira F, Brito F, Sousa R. Open reduction and fixation of trapezium fracture. MOJ Orthop Rheumatol 2017;9:00356. [Google Scholar]
- 22.Pehlivan O, Cilli F, Mahirogullari M, Ozyurek S. Management of combined open fractures of thumb metacarpal and trapezium (surgical tip). Hand 2007;2:48-50. [Google Scholar]
- 23.Brunelli G, Monini L, Brunelli F. Stabilisation of the trapezio-metacarpal joint. J Hand Surg Br 1989;14:209-12. [Google Scholar]
- 24.Jones WA, Ghorbal MS. Fractures of the trapezium. A report on three cases. J Hand Surg 1985;10B:227-30. [Google Scholar]







