
[box type=”bio”] What to Learn from this Article?[/box]
Lateral subtalar joint subluxation is rare but can be easily missed in the presence of other local injuries.
Case Report | Volume 5 | Issue 1 | JOCR Jan-March 2015 | Page 5-7 | TJ Colegate-Stone, SE James, SR Koka. DOI: 10.13107/jocr.2250-0685.214
Authors: TJ Colegate-Stone[1], SE James[1], SR Koka[1]
[1] Department of Orthopaedic & Trauma Surgery, Eastbourne District General Hospital Kings Drive. Eastbourne. BN21 2UD, UK.
Address of Correspondence:
Dr. Toby J Colegate-Stone, Stone 21 Cedars Road, Barnes, London – SW130HP. United Kingdom. Email: tobycolegatestone@yahoo.com
Abstract
Introduction: The referral of a lateral malleolus fracture is one of the commonest orthopaedic trauma presentations. Failure to fully assess the patient and radiography can lead to missing associated injuries in the hindfoot.
Case Report: We describe an unusual hindfoot injury with an atypical combination of lateral subtalar dislocation and calcaneal fracture with associated lateral malleolus fracture that was initially not appreciated by the referring emergency department. This case is of particular interest as subtalar dislocation is a rare injury and lateral subtalar dislocation is even rarer.
Conclusion: Failure to fully assess such injuries and manage non-operatively leads to early degenerative tibia-talar, hindfoot and midfoot changes and a difficult situation for the surgeon to salvage. We advocate early CT scan and open reduction with fixation for such cases.
Keywords: Ankle Fracture, Lateral Subtalar Joint Dislocation, Calcaneal Fracture.
Introduction
The referral of a lateral malleolus fracture is one of the commonest orthopaedic trauma presentations. However failure to fully assess the patient and initial radiography can lead to unappreciated associated injuries in the hindfoot being missed. This may lead to a subsequent delay in diagnosis and appropriate management.
1. We describe an unusual hindfoot injury with an atypical combination of lateral subtalar dislocation and calcaneal fracture with associated lateral malleolus fracture. This case is of particular interest as subtalar dislocation is a rare injury and lateral subtalar dislocation is even rarer.
Case report
A previously active and independent 74 years old man fell from a loft ladder approximately five foot onto his left foot. He was wearing shoes at the time. He was referred from the Accident and Emergency department with a closed neurovascularly intact “ankle fracture” for review (see Fig 1).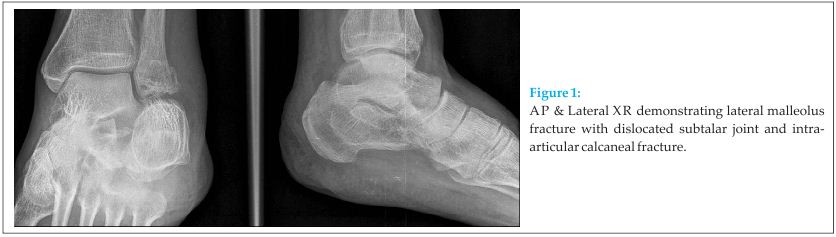
Past medical history was of well controlled hypertension. On examination the hindfoot was grossly swollen and widened with an abnormal lateral border. After referral and evaluation by the on-call Orthopaedic trauma team a CT scan demonstrated the full osseous injury pattern. There was a comminuted intra-articular calcaneal fracture (Sanders IIIC) with a laterally dislocated subtalar joint which had impacted onto the comminuted distal fibula (see Fig 2).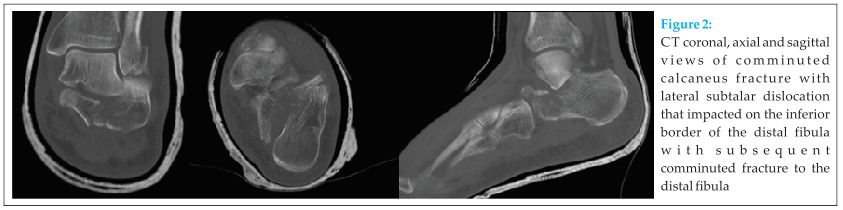
Operative Management
Attempted closed reduction of the subtalar joint in theatre was unsuccessful. Open reduction was achieved via an extended lateral approach. The laterally dislocated subtalar joint was reduced through hinging the lateral calcaneal fragment off the talus. The main body of the calcaneal fragment was reduced and fixed onto the sustentaculum fragment with a lag type screw and a standard calcaneal plate was then attached to hold and neutralise the calcaneal construct. Intra and post operative XR confirmed accurate and stable reduction of the subtalar joint (see Fig 3). 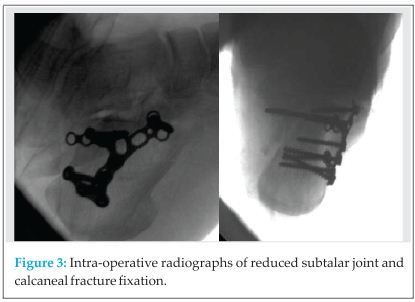 The lateral malleolus fracture was managed conservatively in cast.
The lateral malleolus fracture was managed conservatively in cast.
Post-operatively he was placed in a below knee cast non-weight bearing for 6 weeks.
The last review at eight weeks he was walking with an almost intact pain free range of movement to the tibio-talar joint and a pain free but stiff subtalar range of movement of approximately 20% of normal (see Fig 4).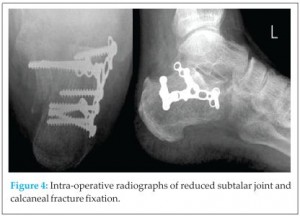
Discussion
Calcaneal fractures represent 60% of all tarsal injuries and 2% of all fractures [1]. This case is unusual due to the associated lateral subtalar dislocation.
Subtalar dislocation is most commonly medial (72-85%), with the foot and calcaneus displaced medially [2, 7]. Lateral subtalar dislocation accounts for 10-15% with reciprocal positioning to medial dislocation. Anterior and posterior dislocation has also been previously reported, however all dislocations are inevitably associated with osteochondral fractures [2, 7]. The strong calcaneonavicular ligament resists deformation so consequentially the weaker talocalcaneal and talonavicular are disrupted. Approximately 15-20% of lateral subtalar dislocations cannot be reduced closed secondary to ligamentous impingement, bony or associated fracture blocks or interposed tibialis posterior tendon [3, 4].
1. The suggested mechanism of injury for this patient is that on impact the primary calcaneal fracture line splits the calcaneus into two parts (anteromedial and posterolateral) [5]. The development of a secondary calcaneal fracture line separates the lateral fragment from the body fragment converting the calcaneus to a three part fracture with either a depression or Tongue type pattern [1, 6]. Significant lateral displacement of the lateral fragment occurs such that it impacts onto the distal end of the lateral malleolus which in turn fractures [6]. The calcaneum fragment then recoils but is unable to reduce as it is wedged against the lateral talar edge.
Conclusion
We suggest that if the full extent of this injury pattern is not fully appreciated and the patient is managed non-operatively it will lead to a widened hindfoot with subsequent early degenerative change to tibia-talar, hindfoot and midfoot joints. This leads to a difficult situation for the surgeon to salvage. We advocate early CT scan and open reduction and internal fixation for such cases.
Clinical Message
The combination of ankle fracture with lateral subtalar dislocation and associated calcaneal fracture is rare and can be subtle on initial plain radiographs. However the consequences of missing these allied injuries leads to a poor prognosis. It is essential to perform more detailed imaging if suspected allowing prompt definitive surgical planning and management to be undertaken.
References
1. Eastwood DM, Gregg PJ, Atkins RM. Intra-articular fractures of the calcaneum. Part I: Pathological anatomy and classification. J Bone Joint Surg Br. 1993;75(2):183-8.
2. Jerome JT. Antero-lateral subtalar dislocation. Foot Ankle Surg. 2008;14(1):36-9.
3. Leitner B. Obstacles to reduction in subtalar dislocations. J Bone Joint Surg Am. 1954;36(A:2):299-306.
4. Heppenstall RB, Farahvar H, Balderston R, Lotke P. Evaluation and management of subtalar dislocations. J Trauma. 1980;20(6):494-7.
5. Palmer I, Widen A. The bone block method for recurrent dislocation of the shoulder joint. J Bone Joint Surg Br. 1948;30B(1):53-8
6. Eastwood DM, Maxwell-Armstrong CA, Atkins RM. Fracture of the lateral malleolus with talar tilt: primarily a calcaneal fracture not an ankle injury. Injury. 1993;24(2):109-12.
7. Hoexum F, Heetveld MJ. Subtalar dislocation: two cases requiring surgery and a literature review of the last 25 years. Arch Orthop Trauma Surg. 2014;134(9):1237-49.
| How to Cite This Article: Colegate TJ, SE James, SR Koka. Beware the Emergency Ankle Fracture Referral: An Unusual Case of Lateral Subtalar Joint Dislocation Secondary to Calcaneal Fracture with associated Lateral Malleolus Fracture. Journal of Orthopaedic Case Reports 2015 Jan-March;5(1): 5-7. Available from: https://www.jocr.co.in/wp/2015/01/28/2250-0685-242-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


