
[box type=”bio”] What to Learn from this Article?[/box]
Treatment of Osteofibrous Dysplasia by extraperiosteal excision and autologous fibular bone graft with bone graft substitute.
Case Report | Volume 5 | Issue 1 | JOCR Jan-March 2015 | Page 41-44 | Abraham VT, Marimuthu C, Subbaraj R, Rengarajan N. DOI: 10.13107/jocr.2250-0685.252
Authors: Abraham VT[1], Marimuthu C[1], Subbaraj R[1], Rengarajan N[1]
[1] Department of Orthopaedics, Mahatma Gandhi Medical College and Research Institute. Sri Balaji Vidyapeeth University, Pondicherry. India.
Address of Correspondence:
Dr. Vineet Thomas Abraham, Associate Professor, Department of Orthopaedics, Mahatma Gandhi Medical College and Research Institute, Sri Balaji Vidyapeeth University. Pondicherry. India. E-mail: abrahamvineet@hotmail.com
Abstract
Introduction: Osteofibrous Dysplasia is a rare benign self-limiting fibro-osseous lesion most commonly seen in the diaphysis of the tibia. Its incidence is reported to be 0.2% of all primary bone tumors. It occurs in the first two decades of life with a slight male preponderance. Surgical options include extra periosteal resection, autologous graft, limb lengthening procedures etc. There are no case reports mentioning the use of synthetic bone graft to fill the defect following extraperiosteal excision.
Case Report: A 13 year old girl presented with pain and swelling of the (R) leg since 2 months following a trivial injury at school. Examination revealed a 5×3cm tender swelling on the anteromedial aspect of the middle third tibia. Radiographs and MRI, revealed an eccentric expansile lytic lesion, which was multilocular and was present at the junction of the metaphysis and diaphysis on the antero -medial aspect of tibia. The cortex had ballooned out and there was a possibility of an impending fracture. Biopsy was done which revealed osteofibrous dysplasia. We did an extraperiosteal excision of the lesion. To fill the cavity we harvested 10 cm of the contralateral fibula and since there was still space in the cavity, we packed bone graft substitute (hydroxyapatite crystals) into the defect. The surgical management of osteofibrous dysplasia is controversial. Various methods of treatment of such cases have been described in literature. The use of synthetic graft is an option in these patients as it reduces morbidity; and in our case we had good graft incorporation with this method.
Conclusion: Extraperiosteal Excision of Osteofibrous dysplasia combined with autologous free fibular graft and bone graft substitute is a good surgical option to prevent recurrence and mange bone defects in this rare lesion.
Keywords: Osteofibrous Dysplasia, Autologous free fibular graft, Bone graft substitute.
Introduction
Osteofibrous Dysplasia is a rare benign self-limiting fibro osseous lesion most commonly seen in the diaphysis of the tibia. Its incidence is reported to be 0.2% of all primary bone tumors. It occurs in the first two decades of life with a slight male preponderance. The etiology of osteofibrous dysplasia, as well as the cell of origin, is unknown. Osteofibrous dysplasia has been postulated to arise from a fibrovascular abnormality. It should be differentiated from fibrous dysplasia and adamantinoma of long bone[1]. Due to high incidence (60-100%) of recurrence, any surgical procedure is recommended only after skeletal maturity. Surgical options include extra periosteal resection, autologous graft, limb lengthening procedures etc. We present a surgical technique which we believe has low recurrence rate.
Case report
A 13 year old girl presented with pain and swelling of the (R) leg since 2 months following a trivial injury at school. Pain was aggravated by running and standing for a long duration and was relieved with rest and medication. Swelling has increased over the past 2 months. Examination revealed a 5×3cm swelling on the anteromedial aspect of the middle third tibia. It was tender, non mobile and hard in consistency. Radiographs- revealed an eccentric expansile lytic lesion, which was multilocular and was present at the junction of the metaphysis and diaphysis on the antero -medial aspect of tibia. The cortex had ballooned out and there was a possibility of an impending fracture (Fig1).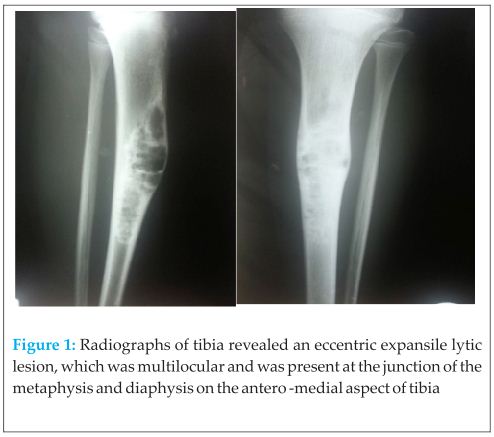 Blood Investigations reported hemogobin to be 9.3 g% and alkaline phosphatase to be 453U/L, Serum calcium was 8.0 mg/dl and Phosphorous was 5.2mg/dl.
Blood Investigations reported hemogobin to be 9.3 g% and alkaline phosphatase to be 453U/L, Serum calcium was 8.0 mg/dl and Phosphorous was 5.2mg/dl.
First a biopsy from the lesion was done and greyish white bits of tissue were sent for histopathology. Biopsy reported bony trabeculae interspersed with fibrous tissue, some bony trabeculae showed curvilinear arrangement with osteoblastic rimming confirming the diagnosis of Osteofibrous dysplasia.
After about a month, since the patient still had pain, we planned to do a extraperiosteal excision of the lesion with autologous fibular graft (Fig 2a). Through an anteromedial approach we exposed the lesion, we did an extraperiosteal excision of the lesion (Fig 2b). To fill the cavity we harvested 10 cm of the contra lateral fibula and since there was still space in the cavity, we packed bone graft substitute (hydroxyapatite crystals) into the defect (Fig. 2c). We wanted to avoid harvesting iliac crest bone graft and increasing the morbidity. Post operatively the wound healed and good radiographic filling of the cavity was seen (Fig 2d). 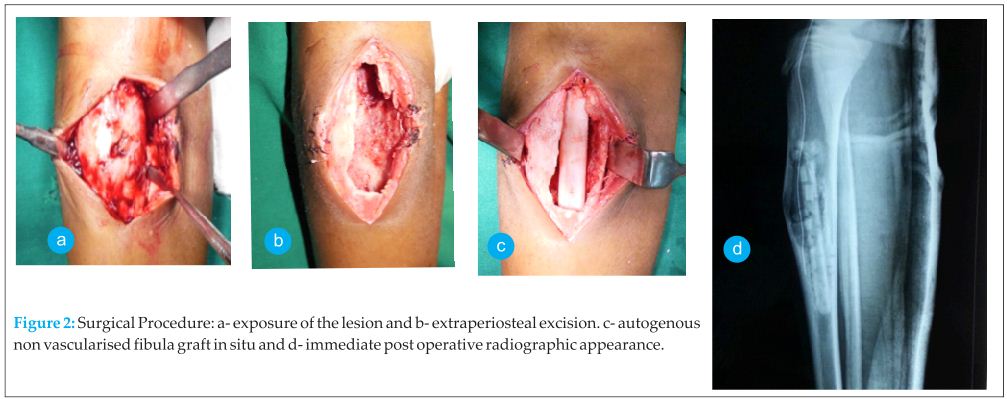
Patient was kept non-weight bearing for a month and then started on partial weight bearing mobilization. Two years follow up radiograph showed good healing with no recurrence (Fig 3) and patient was symptom free.
Discussion
Osteofibrous dysplasia (OFD) is a rare benign fibro-osseous lesion, the patient usually presents with swelling of the leg with or without pain, or with anterior bowing. Some authors mention it as a precursor to adamantinoma [2,3] while other authors conclude that it is a variant of fibrous dysplasia[4]. Campanacci in 1976 named this lesion as “osteofibrous dysplasia of the tibia and fibula “in reference to its anatomic location, developmental origin, and histologic resemblance to fibrous dysplasia”[1]. Sakamoto et al. found that GSα mutation at the Arg201 was seen in fibrous dysplasia but this did not occur in Osteofibrous dysplasia, and they concluded that this could be useful for distinguishing between the two lesions [5].
Radiologically the lesion usually involves the anterior cortex and may cause anterior bowing of the tibia [6,7]. It usually manifests as an intracortical lytic lesion, which is generally well marginated and is often surrounded by a zone of sclerosis [6,7]. Also multiple lucencies may be present within the cortex, with intervening sclerotic areas. Our patient also had involvement of anterior cortex of the tibia with mild bowing, there were areas of multiple lucencies with intervening sclerotic areas (Fig 1).
Histologically OFD is characterized by a loose, often storiform fibrous background containing spicules of woven bony trabeculae that are lined by a layer of osteoblasts[ 8,9,10,11]. This histologic appearance is quite similar to that of fibrous dysplasia but fibrous dysplasia typically lacks the distinctive osteoblastic rimming of the bony trabeculae. Also OFD has a zonal architecture, in which more immature woven bony trabeculae are located centrally; however, as we move to the periphery of the lesion, the trabeculae become more numerous, larger, and more mature and lamellar [8,9,10]. A biopsy is very important to establish the diagnosis and differentiate it from early adamantinoma[5].
The surgical management of osteofibrous dysplasia is controversial. Various methods of treatment of such cases have been described in literature. The different options of treatment include, observation without surgical intervention, bracing to prevent fracture and minimize deformity, surgical option which includes en bloc resection, extraperiosteal resection and filling the defect with autogenous fibular graft, vascularized fibular graft or iliac crest bone graft. The high recurrence rate makes this benign tumor difficult to treat. Most authors advocate excision of the tumor after skeletal maturity as it reduces the chance of recurrence.
Campanacci et al.[1] studied 35 patients with this disease and have advocated surgery in patients with extensive disease, but it should be delayed as much as possible. They had good results with surgery even in patients with recurrence. Lee et al.[12] studied 16 patients with osteofibrous dysplasia and have advocated a more aggressive approach for this lesion. 5 patients underwent sharkbite extraperiosteal excision, 6 patients with larger lesions underwent segmental excision and fibula autograft. 4 patients underwent external fixation and bone transport. One patient underwent proximal tibial replacement. He recommended extraperiosteal resection in all cases of osteofibrous dysplasia.
In our patient we did an extraperiosteal shark bite excision of the tumor. Following the excision we had a large defect, so we packed the defect with contralateral autologous free fibular graft. We wanted to avoid harvesting graft from the iliac crest, so we used bone graft substitute to completely fill the defect. Now at 2 year follow up the graft has incorporated well, (Fig.11) the child has no pain and there is no evidence of recurrence. She is attending school and is able to do all her daily activities.
Autologous fibular graft, along with bone graft substitute is a good alternative in treating this benign lesion to fill up the defect that arises after extraperiosteal excision in large lesions. On doing a literature search we could not find any article using synthetic bone grafts along with autologous fibular graft as a mode of treatment of this lesion.
Conclusion
Extraperiosteal Excision of Osteofibrous dysplasia combined with autologous free fibular graft and bone graft substitute is a good surgical option to mange bone defects in this rare lesion. We believe this will reduce the chances of recurrence, however a larger series of cases will be needed to prove this, which would be difficult in this rare disorder.
Clinical Message
Osteofibrous Dysplasia is a rare fibroosseous lesion. A biopsy must be done to differentiate it from adamantinoma and fibrous dysplasia. After skeletal maturity extraperiosteal excision of the tumor combined with autologous fibular graft and bone graft substitute may be done to prevent recurrence.
References
1. Campanacci M, Laus M Osteofibrous dysplasia of the tibia and fibula J Bone Joint Surg Am, 1981 Mar 01;63(3):367-375
2. Kuruvilla G, Steiner GC Osteofibrous dysplasia-like adamantinoma of bone: A report of five cases with immunohistochemical and ultrastructural studies. Human Pathology;1998 29(8):809-814.
3. Springfield DS, Rosenberg AE, Mankin HJ, Mindell ER. Relationship between osteofibrous dysplasia and adamantinoma. Clin Orthop Relat Res. 1994 Dec;(309):234-44
4. Park YK, Unni MK, Mcleod RA, Pritchard DJ. Osteofibrous dysplasia:clinicopathologic study of 80 cases. Human Pathology 1994; 24(12):1339-1347.
5. Sakamoto A, Oda Y, Iwamoto Y, Tsuneyoshi M. A Comparative Study of Fibrous Dysplasia and Osteofibrous Dysplasia with Regard to GSα Mutation at the Arg201 Codon. J Mol Diagn. May 2000; 2(2): 67–72.
6. Kahn LB: Adamantinoma, osteofibrous dysplasia and differentiated adamantinoma. Skeletal Radiol 2003;32(5):245-258.
7. Levine SM, Lambiase RE, Petchprapa CN: Cortical lesions of the tibia:Characteristic appearances at conventional radiography. Radiographics 2003;23(1):157-177.
8. Gleason BC, Liegl-Atzwanger B,Kozakewich HP, et al: Osteofibrous dysplasia and adamantinoma in children and adolescents: A clinicopathologic reappraisal. Am J Surg Pathol 2008;32(3):363-376
9. Most MJ, Sim FH, Inwards Cy. Osteofibrous Dysplasia and Adamantinoma. J Am Acad Orthop Surg 2010;18:358-366.
10. Ishida T, Iijima T, Kikuchi F, et al: A clinicopathological and immunohistochemical study of osteofibrous dysplasia differentiated adamantinoma, and adamantinoma of long bones. Skeletal Radiol 1992;21(8):493-502.
11. Sweet DE, Vinh TN, Devaney K: Cortical osteofibrous dysplasia of long bone and its relationship to adamantinoma: A clinicopathologic study of 30 cases. Am J Surg Pathol1992;16(3):282-290.
12. Lee RS, Weitzel S, Eastwood DM, Monsell F, Pringle J, Cannon SR, Briggs TWR Osteofibrous dysplasia of the tibia. Is there a need for a radical surgical approach? J Bone Joint Surg Br, 2006;88-B(5) :658-664.
| How to Cite This Article: Abraham VT, Marimuthu C, Subbaraj R, Rengarajan N. Osteofibrous Dysplasia managed with Extraperiosteal excision, Autologous free fibular graft and bone graft substitute. Journal of Orthopaedic Case Reports 2015 Jan-March;5(1): 41-44. Available from: https://www.jocr.co.in/wp/2015/01/28/2250-0685-252-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


