
[box type=”bio”] What to Learn from this Article?[/box]
Presentation and Management of a rare case of floating clavicle.
Case Report | Volume 5 | Issue 2 | JOCR April-June 2015 | Page 12-14 | Alexandra Sopu, Connor Green, Diarmuid Molony. DOI: 10.13107/jocr.2250-0685.261
Authors: Alexandra Sopu[1], Connor Green[1], Diarmuid Molony[1]
[1]Department of Trauma & Orthopaedics, University Hospital Waterford. Ireland.
Address of Correspondence
Dr. Alexandra Sopu,
University Hospital Waterford, Dunmore Road, Waterford, Ireland. Ireland. E-mail: alexandra.sopu@yahoo.com
Abstract
Introduction: Shoulder injuries after high velocity trauma are common. Clavicle is affected in almost half of these cases. Even so, bipolar dislocation of the clavicle is an unusual injury and seldom reported in the literature. Conservative management is used for almost all the cases and only selected cases will undergo surgical treatment.
Case Report: A 52 year old right electrician presented to the emergency department following a fall from a push bicycle. Plain radiographs identified a left first metacarpal (MC) fracture and a bipolar fracture of his right clavicle. Following Fracture Clinic review, significant deformity of the medial clavicle was noted and a CT scan showed anterior dislocation of the medial fragment. Given the degree of deformity and this functional requirement we felt that operative treatment was most appropriate for his unstable medial clavicle fracture dislocation.
Conclusion: Surgical treatment of floating clavicle has an important role in the management of fit and active patients. It is important to identify the mechanism of injury and deforming forces in fractures and only after this to plan to neutralise these where appropriate.
Keywords: bipolar clavicle dislocation; surgical management; floating clavicle; internal fixation.
Introduction
Shoulder injuries after high velocity trauma have been well documented in the literature. Clavicle fractures form 44% of shoulder injuries [1]. Fracture dislocation of medial clavicle with simultaneous fracture of the lateral end or bipolar fracture dislocation of the clavicle is also known as floating clavicle and it is a seldom reported but significant injury [2,3,4].
We report the presentation, treatment and outcome of unilateral floating clavicle in a 52 year old man following a fall from a push bike.
Taking into consideration the type of injury and functional requirement we felt that operative treatment was most appropriate for his medial clavicle fracture dislocation.
As in all injuries it is important to identify the mechanism of injury and deforming forces in fractures and to neutralise these where appropriate. Our solution to treat the medial fracture operatively and continue conservative treatment of the lateral side bears out this rational.
Case report
A 52 year old right hand dominant electrician presented to the emergency department following a fall from a push bicycle. He was assessed according to ATLS protocol and sent for imaging. Plain radiographs identified a left first metacarpal (MC) fracture and a bipolar fracture of his right clavicle (Fig. 1,2). He was initially immobilized in a thumb spica cast for the 1st MC fracture and treated in a broad arm sling for the right clavicle fracture.
Following Fracture Clinic review, significant deformity of the medial clavicle was noted. A CT scan of the right clavicle was performed which showed anterior dislocation of the medial fragment (Fig. 3,4). We proceeded to open exploration and fixation of the medial fragment using a direct approach over the medial aspect of the right clavicle. The fracture was reduced and fixed with a small fragment contoured T plate. Ligamentous complex was found to be stable after fracture reduction and intra articular cartilage was intact thus anatomical stable reduction of the medial fracture dislocation was achieved (Fig. 5,6).
The lateral clavicle fracture was not treated surgically. The patient was placed in a shoulder sling with supervised range of motion exercises without loading for 6 weeks under the physiotherapist’s supervision (pendulum exercises followed by passive glenohumeral motion, static strengthening exercises avoiding abduction of the shoulder. Following satisfactory clinical and radiological evaluation active range of motion was commenced with loading allowed after 10 weeks. Both medial and lateral clavicle fractures underwent clinical and radiological union. The patient returned to work after 4 months, with no residual pain or range of motion deficit. (radiographs at 5 months follow-up, Fig. 7,8).
Discussion
Due to its rarity, there is no consensus in the literature regarding the best method of treatment for floating clavicle.
A review of the existing literature would suggest using age and activity demands as criteria in deciding the approach to treatment. Young and active patients tend to be managed surgically (open or closed reduction and fixation using plate and screws or wires) whereas elderly ones were managed conservatively.
In the absence of neurovascular deficit most authors advocate conservative treatment, surgical treatment (treating each injury as independent) being reserved for selected patients [5,6,7].
A literature review using Scopus with “clavicle” AND “bipolar” terms retrieved 35 results of which 27 were relevant to the topic discussed here. Publications in languages other than English were not excluded in order to minimise the bias.
A comprehensive review of the published literature on the various treatment options used by different authors is shown in Table 1.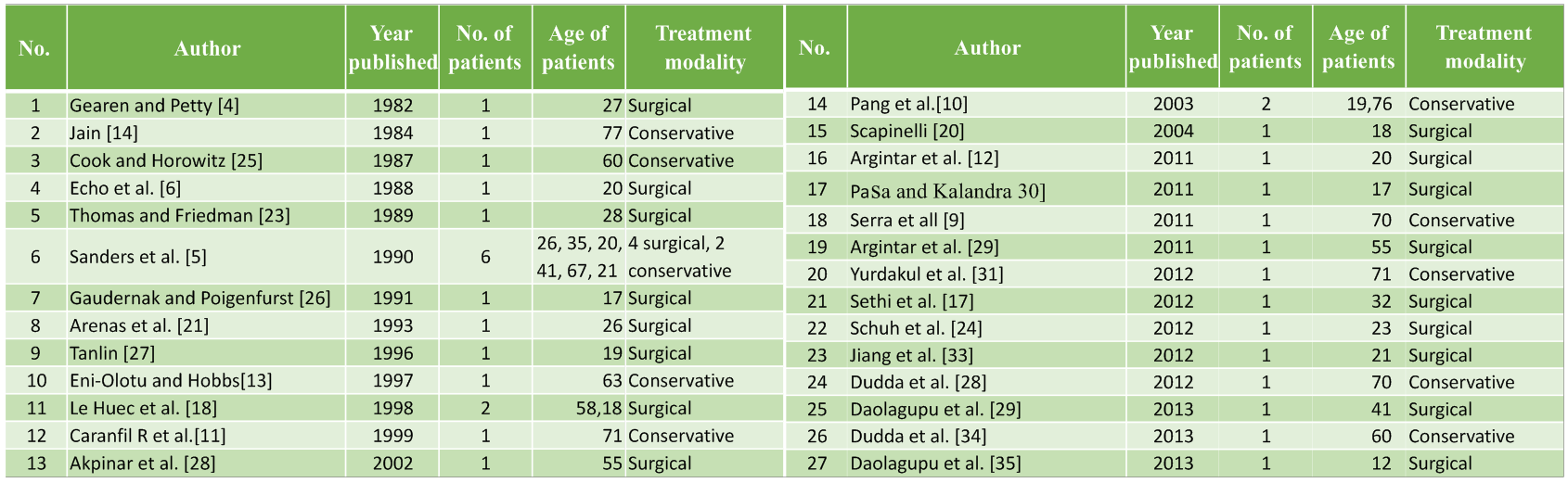
In this case the patient required good overhead strength and would require loading his shoulder in the elevated position which would lead to increased loading at the sternoclavicular joint. The obliquity of the medial fracture with its position medial to the clavicular origin of sternocleidomastoid resulted in its instability and necessitated fixation in this case.
Given the level of this patient’s functional requirement we felt that operative treatment was most appropriate for his medial clavicle fracture dislocation.
Lateral clavicle fractures are typically due to a direct impact injury with anteroinferior rotation of the humeroscapular complex similar to the injury sustained in acromioclavicular (AC) joint disruptions.
In this pattern the AC joint remains intact but the coracoclavicular (CC) ligaments are disrupted with the clavicle fracture leading to an inferior to superior medial to lateral oblique fracture and superior displacement of the medial clavicle fragment. Failure to reconstruct the CC ligaments or to support them while they heal leads to a lack of stability at the fracture site and non-union which is recognised as being common in lateral third clavicle fractures [8] .
In the floating clavicle described in this case, the lateral clavicle fracture has a superior medial to inferior lateral obliquity without displacement of the medial clavicle fragment, the reverse of more commonly seen isolated lateral third clavicle fractures. We interpret this as a shear fracture of the lateral clavicle without disruption of the CC ligaments: a stable injury. As a result conservative treatment was appropriate.
Conclusion
As in all injuries it is important to identify the mechanism of injury and deforming forces in fractures and to neutralise these where appropriate. In our case the fracture pattern of the lateral aspect was shown to be stable by properly examining the radiological images available and documenting the intact coracoclavicular ligament thus having a high potential for healing in the presence of non-displaced fragments. The decision to surgically treat the medial fracture was taken because of the patient’s demanding daily activities that could be satisfied by adopting conservative management.
Clinical Message
Extranodal lymphoma is a rare entity that can mimic a wide range of more common conditions . It is important to have a high index of suspicion when assessing a mass and differential diagnosis should always include lymphoma.
References
1. Mirzayan, Itamura J.M. Shoulder and Elbow Trauma, Raffy, Thieme Medical Publishers, New York, NY, 2004, 213 pp. 147
2. Porral A. Observation of a double dislocation of the right clavicle (in French). J Univ Hebd Med Chir Prat. 1831; 2: 78-82
3. Beckman T. A case of simultaneous luxation of both end of the clavicle. Acta Chir Scand. 1924;56:156–163.
4. Gearen PF, Petty W. Panclavicular dislocation. Report of a case. J Bone Joint Surg Am. 1982;64:454–455
5. Sanders JO, Lyons FA, Rockwood CA Jr. Management of dislocations of both ends of the clavicle. J Bone Joint Surg Am. 1990;72:399–402.
6. 6.Echo BS, Donati RB, Powell CE. Bipolar clavicular dislocation treated surgically. A case report. J Bone Joint Surg Am. 1988;70:1251–1253
7. Macdonald PB, Lapointe P. Acromioclavicular and sternoclavicular joint injuries. Orthop Clin North Am. 2008 Oct;39(4):535-45
8. Robinson CM, Akhtar MA, Jenkins PJ, Sharpe T, Ray A, Olabi B Open reduction and endobutton fixation of displaced fractures of the lateral end of the clavicle in younger patients J Bone Joint Surg Br. 2010 Jun;92(6):811-6.
9. Serra JT, Tomas J, Batalla L, Pedemonte J, Pacha D, Molero V, Carrera L. Traumatic floating clavicle: a case report. J Orthop Trauma. 2011 Oct;25(10):e98-9.
10. Pang KP, Yung SW, Lee TS, Pang CE. Bipolar clavicular injury. Med J Malaysia. 2003 Oct;58(4):621-4.
11. Caranfil R. Bipolar luxation of the clavicle. A case report. Acta Orthop Belg. 1999 Mar;65(1):102-4
12. Argintar E, Holzman M, Gunther S. Bipolar clavicular dislocation. Orthopedics. 2011;34(7):e316–e319.
13. Eni-Olotu DO, Hobbs NJ. Floating clavicle—simultaneous dislocation of both ends of the clavicle. Injury. 1997;28(4):319–320.
14. Jain AS. Traumatic floating clavicle. A case report. Journal of Bone and Joint Surgery B. 1984;66(4):560–561.
15. Sethi K, Newman SDS, Bhattacharya R. An unusual case of bipolar segmental clavicle fracture. Orthopedic Reviews. 2012;4(3, article e26)
16. Le Huec JC, Mc Bride JT, Liquois F, Lesprit E, Le Rebeller A. Bipolar lesion of the clavicle: report of two cases. European Journal of Orthopaedic Surgery and Traumatology. 1998;8(2):85–87.
17. Scapinelli R. Bipolar dislocation of the clavicle: 3D CT imaging and delayed surgical correction of a case. Archives of Orthopaedic and Trauma Surgery. 2004;124(6):421–424.
18. Arenas AJ, Pampliega T, Iglesias J. Surgical management of bipolar clavicular dislocation. Acta Orthopaedica Belgica. 1993;59(2):202–205.
19. Choo CY, HW CY, Nordin A. Traumatic floating clavicle: a case report. Malaysian Orthopaedic Journal. 6(3):57–59.
20. Thomas CB, Jr., Friedman RJ. Ipsilateral sternoclavicular dislocation and clavicle fracture. Journal of Orthopaedic Trauma. 1989;3(4):355–357.
21. Schuh A, Thonse CN, Schmickal T, Kleine L. The operative treatment of bipolar clavicular dislocation: a case report. Journal of Orthopaedic Case Reports. 2012;2(2):21–23.
22. Cook F, Horowitz M. Bipolar clavicular dislocation. Report of a case. Journal of Bone and Joint Surgery A. 1987;69(1):145–147.
23. Gaudernak T, Poigenfurst J. Simultaneous dislocation-fracture on both ends of the clavicle. Unfallchirurgie. 1991;17(6):362–364.
24. Tanlin Y. Ipsilateral sternoclavicular joint dislocation and clavicle fracture. Journal of Orthopaedic Trauma. 1996;10(7):506–507.
25. Akpinar S, Hersekli MA, Demirörs H, Tandoğan RN. Fracture of the medial third of the clavicle and dislocation of the acromioclavicular joint. Artroplasti Artroskopik Cerrahi. 2002;13(1):41–44.
26. Argintar E, Holzman M, Gunther S. Bipolar clavicular dislocation. Orthopedics. 2011;34(7):e316–e319.
27. Paša L, Kalandra S. Dislocation of the clavicle: case report. Acta Chirurgiae Orthopaedicae et Traumatologiae Cechoslovaca. 2011;78(2):165–168.
28. Yurdakul E, Salt Ö, Uzun E, Doğar F, Güney A, Durukan P. Traumatic floating clavicle. The American Journal of Emergency Medicine. 2012;30(9):2097.e3–2097.e5.
29. Jiang W, Gao SG, Li YS, Lei GH. Bipolar dislocation of the clavicle. Indian Journal of Orthopaedics. 2012;46(6):721–724.
30. Dudda M, Kruppa C, Schildhauer TA. Post-traumatic bipolar dislocation of the clavicle—is operative treatment reasonable? Unfallchirurg. 2012;116(2):176–179.
31. Daolagupu AK, Gogoi PJ, Mudiganty S. A rare case of segmental clavicle fracture in an adolescent. Case Reports in Orthopedics. 2013;2013:2 pages.248159
| How to Cite This Article: Sopu A, Green C, Molony D. Traumatic floating clavicle- A case report. Journal of Orthopaedic Case Reports 2015 April-June;5(2): 12-14 . Available from: https://www.jocr.co.in/wp/2015/04/20/2250-0685-261-fulltext-2/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


