
[box type=”bio”] What to Learn from this Article?[/box]
If clinico-radio logical features s/o giant cell tumor are present, then neither location nor skeletal immaturity rules out the diagnosis. Diagnosis should be solely depend on Histopathological examination.
Case Report | Volume 5 | Issue 2 | JOCR April-June 2015 | Page:28-31 | Maulik T Patel, Maunil R Nayak. DOI: 10.13107/jocr.2250-0685.266
Authors: Maulik T Patel[1], Maunil R Nayak[2]
[1] Department of Orthopaedics, Meenakshi Mission Hospital and Research Centre, Madurai, Tamilnadu. India.
[2] Department of Orthopaedics, C.U.SHAH Medical College, Surendra Nagar. India.
Address of Correspondence:
Dr Maulik Patel,
Department of Orthopaedics Meenakshi Mission Hospital and Research Centre, Lake Area, Melur Road, Madurai- 625017, Tamilnadu, India.
E-mail: drmaulikpatel137@gmail.com
Abstract
Introduction: Giant cell tumor is a locally aggressive benign tumor. Giant cell tumor of bone is characteristically found in skeletally mature patient at the end of long bones in the epiphyseal region or epiphysio-metaphyseal region. Giant cell tumor is very rare in skeletally immature patient. But we are presenting a very rare case of giant cell tumor in skeletally immature patient in diaphyseal region which is very uncommon location for giant cell tumor. From this case we concluded that irrespective of the location and skeletal maturity, a giant cell tumor should be diagnosed based on its histology because classical clinical- radiological features are not always present. Index case strengthens this view.
Keywords: Giant cell tumor, skeletal maturity, diaphyseal location.
Introduction
Giant cell tumor is a locally aggressive benign tumor. Jaffe and Lichtenstein first proposed classification and definition of giant cell lesions. [1]. Occurrence of GCT is relatively high and 20% of all benign bone tumors and 5% of all tumors are giant cell tumors. GCT mostly occurs in the age group of 20 to 40 years. [2-4]. Females are more commonly involved in GCT with male-female ratio being 1:3 to 1:5. Rate of growth of GCT enhances in pregnancy [5]. Occurrence of GCT before skeletal maturity is rare [2, 6, 7]. Common sites for GCT are distal femur, the proximal tibia, the distal radius and the sacrum [2-4].GCT usually occurs at the epiphyses of long bones. The involvement of the metaphysis or diaphysis without epiphyseal extension is rare [1]. Sometimes in GCT, metaphysis involvement seen before epiphysis involvement [8, 9]. There are very few reported cases of diaphyseal GCT. [10-14].This is a very rare case of diaphyseal GCT in a skeletally immature patient. Recurrence rate of GCT is 25–50% but malignant transformation is less than 5%. [15-17].
Case report
A 15 years old girl came to our hospital with a complaint of pain and swelling over her left hand with history of fall. She also complained of occasional pain over lower third and inner aspect of her forearm. While we were managing the patient for hand injury we took x-ray of hand with wrist and forearm suggesting of fracture of fifth metacarpal. X ray also showed findings of expansile lytic lesion with multiple septas in diaphyseal region of left ulna. Examination of forearm revealed a mild diffuse swelling over the lower third and inner aspect of her left forearm. The overlying skin was normal. No signs of inflammation were visible. On palpation, there was tenderness over the swelling. The swelling was soft in consistency with a feeling of ‘egg shell crackling’. Movement at all the joints was full in range and was painless. There was no neurovascular deficit. Clinically diagnosis came out to be either Aneurysmal bone cyst or Simple bone cyst. We decided to take FNAC. The report of FNAC was suggestive of Giant cell tumor. For confirmation of diagnosis, we took open incisional biopsy which came out to be giant cell tumor. Diagnosis of giant cell tumor was confirmed as we sent specimen at two different histo-pathology laboratory, both suggestive of GCT. Then after proper counseling of patient and relatives, we decided to excise whole tumor and reconstruct it with a fibular graft. We expose entire tumor with standard ulna surgical approach. We had removed tumor with 1 cm clinically normal looking bone both side. We had also sent intra operative frozen section for safe margin. Report came as negative. The bone gap after excision of tumor in ulna was about 8 cm. We took cortical bone graft from ipsilateral fibula of respective size. We took cancellous bone graft from ipsilateral proximal tibia. Implantation of fibula at recipient site after appropriate freshening of margins, fixation of fibula in between the two ends of ulna with intramedullary ulna nail from proximal to distal. Then we put cancellous bone graft at both ends which were taken from ipsilateral proximal tibia & then closure was done in layers. The tumor was reddish brown, ovoid in shape and soft in consistency. Frozen section was done to know the extent. It extended from the diaphyseal area of the distal ulna to the distal third. It was removed cleanly. After doing Histology examination diagnosis of giant cell tumor was confirmed. After discharge, first 6 month patient was followed every 2 monthly. After six month, next visit every 6 monthly up to 2 years. Complete fibula incorporation at the end of one year. Next follow ups were uneventful.
Discussion
Giant cell tumor occurs mostly in age group of 20-40 years. The peak incidence of GCT occurs in 2nd- 3rd decades of life. Giant cell tumors are much less common in skeletally immature patient and incidence is 5.7% [2,6,7]. Male female ratio of GCT is 1:3 to 1:5 suggesting that GCT is more common in female than male [5]. Giant cell tumors are mostly solitary, and multicentre in 1-2%. Giant cell tumors are present mostly in the epiphyseal or epi-metaphyseal end of the long bones. Doubt arises if the epiphysis is not involved in a case of GCT. The radiographic findings are helpful but cannot be confirmatory. Histological examination is still the gold standard for diagnosis. It is very difficult for a pathologist to distinguish metaphyseal and diaphyseal GCT from other lesions.
Differential Diagnosis:
(1) Unicameral bone cysts (UBC): Also known as simple bone cysts. These lesions consist of a fluid filled cavity lined by a thin membrane. They are found in the metaphysis of long bones, with the most common site being the proximal humerus, followed by the proximal femur followed by other long bone [18,19]. These are some differentiating points of UBC from GCT. UBC’s are found most commonly in children between the ages of 5 to 20 years old [18,19] whereas GCT peak in 2nd and 3rd decade. UBC is male predominance whereas GCT female predominance. Radiologically lesion appears as a well defined osteolytic area with a thin sclerotic margin. A fragment of cortex that has fallen into a dependent position inside the cyst is known as the “fallen leaf” or “fallen fragment” sign [20]. It is very difficult to differentiate it from giant cell tumor only by radiography. For that Histopathological confirmation is necessary. Microscopically, the UBC has a membrane made up of a layer of flattened cuboidal cells that resemble endothelium. The cyst fluid resembles synovial fluid.
(2) Aneurysmal bone cyst: Aneurysmal bone cyst is eccentric and it is typically seen in the metaphysial area, not extending into the epiphysis [19].In a typical case of aneurysmal bone cyst radiograph shows rarefaction of the bone and ballooning of the bony cortex giving a blow-out appearance of part of the contour of the affected bone area [21]. Giant-cell tumors produce rarefaction of the bone, the overlying cortex being expanded and thinned. Whenever GCT involves metaphysis beyond epiphysis, the differential diagnosis should include aneurysmal bone cyst and judgment has to rely principally on Histopathological examination [22].
3) Giant cell-rich osteosarcoma: It is extremely rare variant of osteosarcoma, and its incidence was reported to make up 3% of all osteosarcoma cases [23]. The typical radiographic patterns of giant cell-rich osteosarcoma are as follows: An ill-defined margin surrounds a predominantly lytic lesion of the diaphysis or metaphysis of the femur or tibia of a young patient with a soft-tissue mass and weak periosteal reaction [23]. Three important radiographic differential points for GCT like variants of osteosarcoma from true GCT: (1) Metaphyseal or diaphyseal centring versus epiphyseal centring, (2) Codman’s triangle (3) Radiographic intralesional fluffs [24]. Histologically there are two differentiating histological points between giant cell-rich osteosarcoma and true GCT. One difference is anaplasia of some stromal cells and the other is osseous tumour tissue production [24].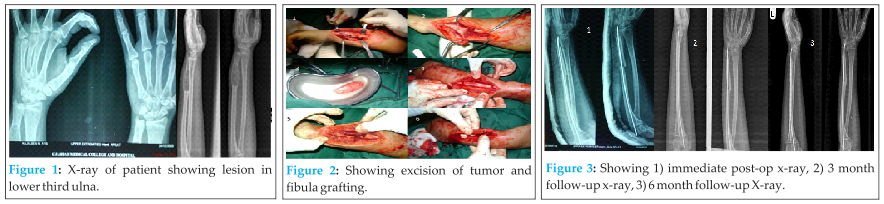
4) Fibrous cortical defect: It is a benign fibrous small cortical lesion in the metaphysis of long bone [25]. The lesion is directly under the periosteum with a thin rim of bone separating it from the medullary canal and appears as a well-defined lucent cortical defect on x-ray. These lesions are developmental defects in which parts of bone that normally ossify are instead filled with fibrous tissue. They commonly affect the metaphysis, and the most commonly affected sites are, in order, the distal femur, distal tibia, and proximal tibia [26]. Histologically lesion is composed of fibrous tissue arranged in a whirling pattern, multinucleated giant cells, and often histiocytes with large amounts of clear cytoplasmic material, so called “foam” cells.
With the battery of investigation modalities like radiological and histological examination, we have ruled out other all possible differential diagnosis and diagnosis of giant cell tumor was stamped in our patient. The patient’s age, the location of the lesion, its radiographic appearance and the gross appearances are the most important criteria for diagnosis of a bone tumor. However, the final diagnosis depends on the tumor’s histological appearance only [10]. As Jaffe has mentioned ‘A bone lesion may be uncharacteristic in all other respects, but if it exhibits the cytological pattern of a giant cell tumor, it should be recognized as a GCT [27].
Treatment:
There are various treatment modalities for giant cell tumor described in literatures. Various treatment options are: Intralesional Curettage, Intralesional Curettage and bone grafting, Intralesional Curettage and insertion of polymethylmethacrylate (PMMA), Primary resection, Radiation therapy, Embolization of the feeding vessels. But there is always controversy for which is the best treatment due to variable recurrence rate with different modalities. Bitoh s et al, suggest that the treatment of choice is complete surgical excision which if achieved, can be curative [28].
Intralesional curettage and bone grafting is a limb-sparing option that is associated with good functional and oncologic outcomes. However, simple curettage with or without bone graft has high recurrence. The high risk of recurrence led several surgeons to replace bone graft packing of the lesion with PMMA packing. The heat given off by the hardening PMMA is thought to lead to thermal necrosis of the remaining tumor cells in the curetted cavity [29,30]. The PMMA technique, compared with bone grafting, offers the advantages of lack of donor-site morbidity, an unlimited supply, immediate structural stability, low cost, and ease of use [31].The disadvantages of using cement include difficulty in removing it when revision is needed and the possibility that subchondral cement may predispose the joint to early degenerative osteoarthritis [32,33]. The latter is a theory that remains to be proven [34]. Several authors have added the technique of high-speed burring of the cavity after simple intralesional curettage. The high-speed burr not only adds a thermal component to eradication of the tumor but also allows more thorough removal of the tumor. High-speed burring of the cavity then may be followed by a chemical or physical adjuvant and packing of the lesion with PMMA or a bone graft [35].
Adjuvant therapies, such as phenol, liquid nitrogen, or H2 O2 and argon beam coagulation, all have advantages and disadvantages of its own [36]. However, they all offer a method for eradication of microscopic disease.
Radiotherapy in modest doses (35 Gy in 15 fractions or equivalent) is a safe and effective option for primary and recurrent giant cell tumours of bone. It should be used if surgery would result in significant functional morbidity [37]. However, use of cryotherapy and antiangiogenic therapy with interferon Alfa-2a also has been advocated in cases of recurrent giant cell tumour [38].
Giant cells are known to express RANKL (receptor activator of nuclear factor κB ligand). This RANKL is responsible for the aggressive osteolytic nature of the tumor. Denosumab is a fully human monoclonal antibody that targets and binds with high affinity and specificity to RANKL. Several large phase III studies have shown that denosumab is more effective in reducing skeletal morbidity arising aggressive osteolytic nature of the tumor. In the near future, denosumab may offer a treatment option for unresectable GCT or an alternative to surgical procedures that would result in severe morbidity. But safety and long-term follow up for denosumab yet to be defined [39].
In our case complete resection was possible and reconstruction also was possible with fibular graft [28]. There was no recurrence in our case with good functional results after 2 years of follow up. [Figure4 & 5- 2 years follow up radiographs and clinical photos].
Conclusion
After doing literature and online search we concluded that, there are seven reported cases of GCT occurring in diaphysis of long bones [40] and rare in skeletally immature patient [41]. We concluded that patient’s age, the location of the lesion, radiographic appearance and the gross appearances are crucial to unravel the mystery of any bony lesion. However, the final diagnosis should depend on the tumor’s Histopathological appearance only [10].
Clinical Message
The patient’s age, the location of the lesion, its roentgen graphic appearance, and the gross and microscopic appearances are the most important criteria for diagnosis of a bone tumor. However, the final diagnosis depends on the tumor’s histological appearance only [10]. As Jaffe has mentioned ‘A bone lesion may be uncharacteristic in all other respects, but if it exhibits the cytological pattern of a giant cell tumor, it should be recognized as a GCT’ [18].
References
1. Jaffe HL, Lichtenstien L, Portis RB: Giant cell tumor of bone. Its pathologic appearance, grading, supposed variants and treatment. Arch Pathol1940, 30:993-1031.
2. Unni KK: Dahlin’s bone tumors: general aspect and data on 11087 cases. 5th edition. Philadelphia: Lippincott-Raven; 1998.
3. Huvos AG: Bone tumors: diagnosis, treatment and prognosis. 2nd edition. Philadelphia: WB Saunders Co; 1991.
4. Bridge JA, Neff JR, Mouron BJ: Giant cell tumor of bone: chromosomal analysis of 48 specimens and review of the literature. Cancer Genet Cytogenet1992, 58:2-13.
5. Bulstrode C, Bukwalter J, Carr A, Marsh L, Fairbank J, Wilson-Mac- Donald J, Bowden G: Oxford Textbook of OrthopaedicsandTrauma. 1st edition. 2002, 1:162.
6. Campanacci M: Giant cell tumor. In Bone and soft-tissue tumors Edited by: Gaggi A. Bologna, Italy: Springer Verlag; 1990:117-53.
7. Picci P, Manfrini M, Zucchi V, Gherlinzoni F, Rock M, Bertoni F, Neff JR: Giant cell tumor of bone in skeletally immature patients.J Bone Joint Surg Am 1983, 65:486-90.
8. Hoeffel JC, Galloy MA, Grignon Y, Chastagner P, Floquet J, Mainard L, Kadiri R: Giant-cell tumor of bone in children and adolescents.RevRbum1996, 63(9):618-23.
9. Shih HN, Hsu RW, Sim FH: Excision curettage and allografting of giant cell tumours. World J Surg 1998, 22:432-7.
10. Wilkerson JA, Cracchiolo A 3rd: Giant-cell tumor of the tibial diaphysis. J Bone Joint Surg Am 1969, 51:1205-9.
11. Visscher DW, Alexander RW, Dempsey TR: Case Report 472: Heretical giant cell tumor in the diaphysis of ulna of a 7 month old boy. Skeletal Radiol1988, 17(4):285-8.
12. Fain JS, Unni KK, Beabout JW, Rock MG: Nonepiphyseal giant cell tumor of the long bones. Clinical, radiologic, and pathologic study. Cancer 71(11):3514-9. 1993 Jun 1;
13. Sanjay BK, Raj GA, Vishwakarma GK: En bloc excision and reconstruction with a fibular autograft of giant-cell tumour of the metacarpal – a case report. J Hand Surg [Br] 1989, 14(2):226-8.
14. Schajowicz F: Tumors and tumor like lesions of bone and joints. New York: Springer-Verlag; 1981:205-39.
15. Trieb K, Bitzan P, Dominkus M, Kotz R: Giant-cell tumors of long bone. J Bone Joint Surg Am 2000, 82:1360-1.
16. Boriani S, Sudanese A, Baldani N, Picci P: Sarcomatous degeneration of giant cell tumors. Ital J OrthopTraumatol1986, 12(2):191-9.
17. Gitelis S, Wang J, Quast M, Schajowicz F, Templeton A: Recurrence of a giant-cell tumor with malignant transformation to a fibrosarcoma twenty-five years after primary treatment. J Bone Joint Surg Am 1990, 71:757-61.
18. Lokiec F, Ezra E, Khermosh O, Wientroub S. Simple bone cysts treated by percutaneous autologous marrow grafting. A preliminary report. J Bone Joint Surg Br. Nov 1996;78(6):934-7.
19. Lokiec F, Wientroub S. Simple bone cyst: etiology, classification, pathology, and treatment modalities. J Pediatr Orthop B. Oct 1998;7(4):262-73
20. Reynolds J. The “fallen fragment sign” in the diagnosis of unicameral bone cysts. Radiology. Apr 1969;92(5):949-53
21. Boubbou M, Atarraf K, Chater L, Afifi A, Tizniti S. Aneurysmal bone cyst primary – about eight pediatric cases: radiological aspects and review of the literature. Pan Afr Med J. Jul 28 2013;15:111.
22. H. verbiest, Utrecht, The journal of bone and joint surgery. Giant cell tumors and aneurysmal bone cysts of spine page no 701, vol 47, nov 1965
23. Bathurst, N. and Sanerkin, N.: Osteoclast-rich osteosarcoma. BiR, 59, 667-673 (1986).
24. Mirra, J.M.: Bone tumors: clinical, radiologic and pathologic correlations. pp.326-331 (1989)
25. Betsy M, Kupersmith LM, Springfield DS. Metaphyseal fibrous defects. J Am Acad Orthop Surg. Mar-Apr 2004;12(2):89-95.
26. Jaffe HL, Lichtenstein L. Solitary unicameral bone cyst with emphasis on the roentgen picture, the pathologic appearance and the pathogenesis. Arch Surg. 1942;44:1004-25.
27. Jaffe HL: Giant-cell tumour (osteoclastoma) of bone: its pathologic delimitation and the inherent clinical implications. Ann Roy CollSurgEngl1953, 13(6):343-55.
28. Bitoh S, Takimoto N, Nakagawa H, Namba J, Sakaki S, Gohma T. Giant cell tumor of the skull. Surg Neurol. 1978;9:185e188
29. Leeson MC, Lippitt SB. Thermal aspects of the use of polymethylmethacrylate in large metaphyseal defects in bone. A clinical review and laboratory study. Clin Orthop. Oct 1993;(295):239-45
30. Mjoberg B, Pettersson H, Rosenqvist R. Bone cement, thermal injury and the radiolucent zone. Acta Orthop Scand. Dec 1984;55(6):597-600.
31. Tunn PU, Schlag PM. Giant cell tumor of bone. An evaluation of 87 patients. Z Orthop Ihre Grenzgeb. 2003;141:690-8
32. Campanacci M, Capanna R, Fabbri N, et al. Curettage of giant cell tumor of bone. Reconstruction with subchondral grafts and cement. Chir Organi Mov. 1990;75(1 Suppl):212-3
33 Persson BM, Wouters HW. Curettage and acrylic cementation in surgery of giant cell tumors of bone. Clin Orthop. 1976;00(120):125-33.
34. Wilkins RM, Okada Y, Sim FH, et al. Methyl methacrylate replacement of subchondral bone: a biomechanical, biochemical, and morphologic analysis. In: Enneking WF, et al. Limb Salvage in Musculoskeletal Oncology. New York, NY:. Churchill Livingstone;1987: 479-86.
35. Blackley HR, Wunder JS, Davis AM, et al. Treatment of giant-cell tumors of long bones with curettage and bone- grafting. J Bone Joint Surg Am. Jun 1999;81(6):811-20.
36. Balke M, Schremper L, Gebert C, Ahrens H, Streitbuerger A, Koehler G, et al. Giant cell tumor of bone: treatment and outcome of 214 cases. J Cancer Res Clin Oncol. Sep 2008;134(9):969-78
37. Malona Shawn, O’Sullivan Vrian, Bell Robert, Forniser Victor, Davis Aileen. Long term follow up of efficacy and safety of megavoltage radiotherapy in high risk giant cell tumors of bone. Int J Radiat Oncol Biol Phys. 1995; Oct 15;33(3).
38. Dickerman Joseph D. Antiangiogenic therapy of recurrent giant cell tumor of the mandible with interferon Alfa 2a. Pediatrics. 1999;103(6):1282e1283.
39. Ajay Puri and Manish Agarwal. Treatment of giant cell tumor of bone: Current concepts Indian J Orthop. 2007 Apr-Jun; 41(2): 101–108.
40. Sandeep Shrivastava, Shishir P Nawghare, Yogesh Kolwadkar and Pradeep Singh,Giant cell tumour in the diaphysis of radius – a report, Cases Journal 2008, 1:106 doi:10.1186/1757-1626-1-106.
41. Surojit Mondal1, Aniket Chowdhury2 and Goutam Bandyopadhyay3, International Journal of Basic and Applied Medical Sciences ISSN: 2277-2103 (Online) An Online International Journal Available at http://www.cibtech.org/jms.htm 2013 Vol. 3 (1) January-April, pp.220-224.
| How to Cite This Article: Patel MT, Nayak MR. Unusual Presentation of Giant Cell Tumor in Skeletally Immature Patient in Diaphysis of Ulna. Journal of Orthopaedic Case Reports 2015 April-June;5(2):28-31. Available from: https://www.jocr.co.in/wp/2015/04/20/2250-0685-266-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


