
[box type=”bio”] What to Learn from this Article?[/box]
Always consider musculoskeletal injury in post-ictal patients, particularly shoulder dislocation which may be missed if not screened for.
Case Report | Volume 5 | Issue 2 | JOCR April-June 2015 | Page 38-40| Andrew Wheelton, Daniel Dowen. DOI: 10.13107/jocr.2250-0685.269
Authors: Andrew Wheelton[1], Daniel Dowen[2]
[1] ST5 Trauma and Orthopaedics, North West Deanery. England.
[1] ST8 Trauma and Orthopaedics, Northern Deanery. England.
Address of Correspondence:
Dr Andrew Wheelton
28 Austin Drive, Manchester, England M20 6EG.
Email : andrewwheelton@doctors.org.uk
Abstract
Introduction: Bilateral anterior shoulder dislocation following a seizure has recently been demonstrated as being more common than previously believed with 44 cases in the literature. This case is unique as it was caused by a first time seizure and there was no associated fracture of the humerus.
Case Report: A previously fit and well 32 year old man presented to the Emergency Department following a convulsive episode. On initial assessment he was drowsy and the focus of investigation was the cause of the seizure, he was prepared for transfer to the medical ward. As he became more alert he complained of bilateral shoulder pain. Further clinical exam highlighted he had reduced range of movement in the shoulder joint bilaterally with a symmetrical clinical appearance of gleno-humeral dislocation. Radiographs confirmed bilateral anterior gleno-humeral dislocations which were reduced under sedation uneventfully.
Conclusion: Post ictal patients can be difficult to assess when drowsy. Although not all seizures require musculoskeletal examination attending medical staff should remain vigilant to the possibility of injury following seizure to afford prompt diagnosis and treatment.
Keywords: musculo-skeletal; fractures and dislocations; diagnosis; emergency department management.
Introduction
Bilateral shoulder dislocations are regarded as rare orthopaedic injuries. Recent literature review articles have demonstrated that this entity is not as uncommon as believed with 44 cases reported in international journals. This case has two features which make it unusual
Case report
A previously fit and well 32 year old man presented to the Emergency Department with an episode of convulsion. Whilst sat down at home he suddenly became unresponsive followed by a generalized convulsion of the upper body which terminated spontaneously. He remained on the chair throughout and sustained no trauma. A post-ictal period followed. On presentation he was drowsy but orientated with a GCS of 15. He was initially investigated for the cause of seizure and prepared for transfer to a medicine ward. As he became more alert he directed medical staff to his shoulder injuries which were almost missed. Further clinical exam highlighted he had reduced range of movement in the shoulder joint bilaterally with a symmetrical clinical appearance of gleno-humeral dislocation. There was no neurovascular deficit. Radiographs confirmed bilateral anterior dislocations and following sedation, both were reduced uneventfully using the Kocher technique.
Tests were performed to ascertain the cause of the seizure. Neuro-imaging including CT angiography and MRI scan of the brain revealed no abnormality. Blood tests including glucose were all normal and a sleep deprived EEG revealed no abnormality. It is likely that this was a first epileptic seizure. He was encouraged to mobilise both joints early. On follow up he has had no long term sequelae from the shoulder dislocations and has a good range of movement bilaterally.
Discussion
Recent literature review articles have demonstrated that bilateral anterior glenohumeral dislocation is not as rare as was once believed with Ballesteros demonstrating there are 44 cases in the literature [1]. Bilateral anterior dislocations have been described following trauma, seizure and electric shock [2,3] The mechanism during seizures predisposes to posterior dislocations with the external rotators of the humerus (infraspinatous and teres minor) being overpowered by the more powerful internal roatators (latissimus dorsi, pectoralis major and subscapularis) causing adduction and internal rotation strong enough to dislocate the humeral head posteriorly. 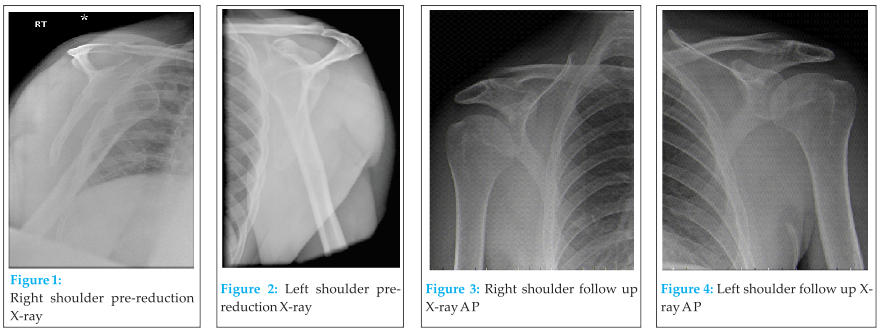 Subsequently trauma is a more common cause of bilateral anterior dislocation than seizure as reported by Galanakos et al, Dunlop and Siwach [1,2,3]. Many of the cases in the literature are also associated with fractures of the humerus and or glenoid [2]. Sreesobh suggested that only 3 cases of bilateral anterior dislocation have been reported without associated fractures, none of which were following seizure [4]. A further case described by Segal occurred in a patient who had sustained a previous dislocation of the left shoulder [5].
Subsequently trauma is a more common cause of bilateral anterior dislocation than seizure as reported by Galanakos et al, Dunlop and Siwach [1,2,3]. Many of the cases in the literature are also associated with fractures of the humerus and or glenoid [2]. Sreesobh suggested that only 3 cases of bilateral anterior dislocation have been reported without associated fractures, none of which were following seizure [4]. A further case described by Segal occurred in a patient who had sustained a previous dislocation of the left shoulder [5]. 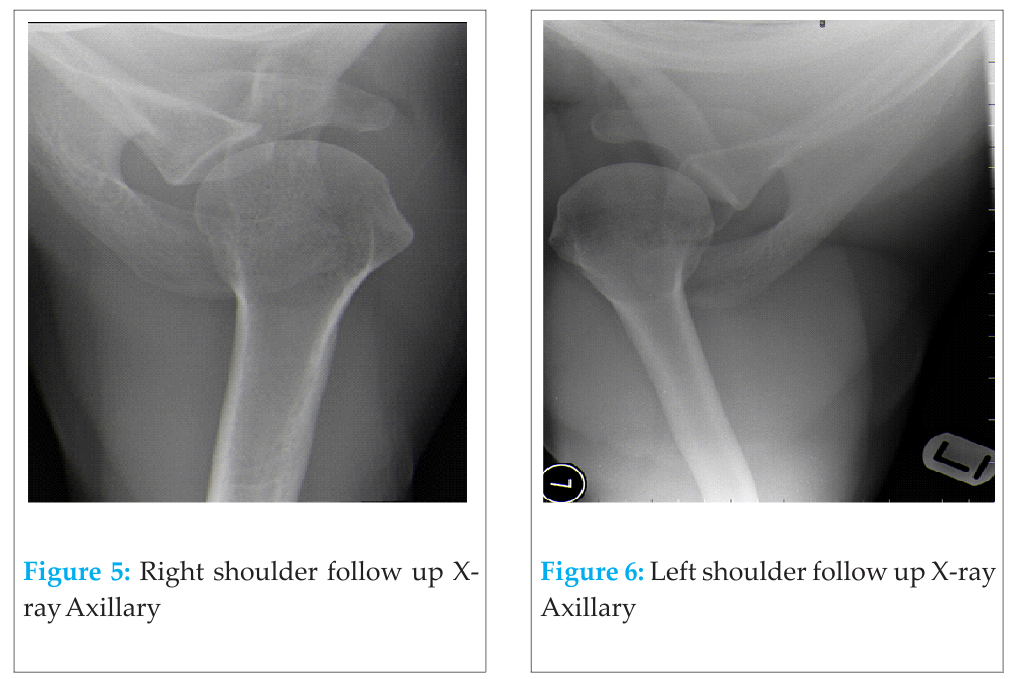 This case is unusual being an anterior glenohumeral dislocation, in previously uninjured shoulders, following a presumed first epileptic seizure. To the best of the author’s knowledge this is the only case reported within the literature.
This case is unusual being an anterior glenohumeral dislocation, in previously uninjured shoulders, following a presumed first epileptic seizure. To the best of the author’s knowledge this is the only case reported within the literature.
Conclusion
Bilateral asymmetric dislocation of shoulders resulting from seizure although rare is more common than perceived. When present they represent one of the true orthopaedic emergency conditions requiring prompt diagnosis and treatment. Early reduction of the shoulders is essential to relieve pain and to prevent long term complications like avascular necrosis of the humeral head.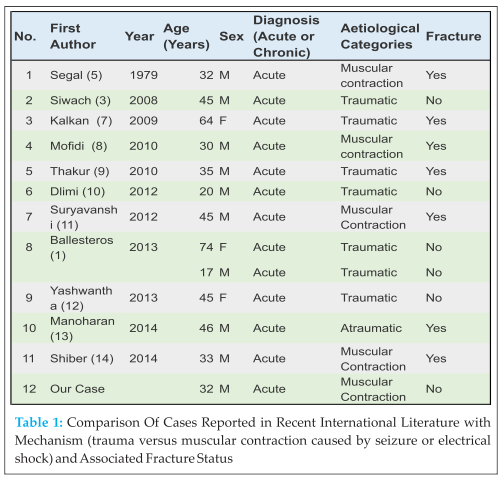
Clinical
Post ictal patients are drowsy and are often unable to give coherent histories. This can make diagnosis difficult.Attending medical staff should remain vigilant to the possibility of injury following seizure.
References
1. Ballesteros R, Benavente P, Bonsfills N, Chacon M, Garcia-Lazaro F (2013) Bilateral anterior dislocation of the shoulder: review of seventy cases and proposal of a new etiological-mechanical classification. Journal Of Emergency Medicine 44(1): 269-79.
2. Galanakos S (2008) Bilateral anterior glenohumeral dislocation – a case report and review of the literature. Acta Orthopaedica et traumatologica Hellinica 59(4): 252-256.
3. Siwach R, Singh R, Rohilla, Sangwan S (2008) Bilateral anterior dislocation of the shoulder—A case report and review of the literature. Injury Extra 39(12); 394-397.
4. Sreesobh K, Chako B (2005) An unusual Case Of Bilateral Anterior Dislocation Of Shoulder. Journal Of Orthopaedics 2(4) e6.
5. Segal D, Yablon IG, Lynch JJ, Jones RP 91979) Acute bilateral anterior dislocation of shoulder following grand-mal convulsion. Ann Emerg Med 18(5); 589-591.
6. Dunlop CC (2002) Bilateral anterior shoulder dislocation- a case report and review of the literature. Acta Ortop Belg 68(2): 168-170.
7. Kalkan T, Demirkale I, Ocguder A, Unlu S, Bozkurt M (2009) Bilateral anterior shoulder dislocation in two cases due to housework accidents. Acta Orthop Traumatol Turc 43:260–38.
8. Mofidi M, Kianmehr N, Farsi D, Yazdanpanah R, Majidinezhad S, Asadi P (2010) .
An unusual case of bilateral anterior shoulder and mandible dislocations. Am J Emerg Med 28:745.
9. Thakur A, Gupta R, Kotwal V, Arora D (2010) A rare case of bilateral anterior dislocation of the shoulder. Journal of Clinical and Diagnostic Research 4:3567–9.
10. Dlimi F et al (2012) Bilateral anterior dislocation of the shoulders at the start of a backstroke competition. Journal of Orthopaedics and Traumatology : Official Journal of the Italian Society of Orthopaedics and Traumatology, 13(1): 47–49.
11. Ashish Suryavanshi, Amber Mittal, Snehak Dongre, Neeti Kashyap (2012) Bilateral anterior dislocation of shoulder with symmetrical greater tuberosity fracture following seizure. Journal of Orthopaedic Case Reports 1(1):28-31
12. Yashwantha KC, Nalini KB, Maini Lalit, Nagaraj P (2013) Bilateral traumatic anterior dislocation of shoulder, a rare entity. Journal of Orthopaedic Case Reports 3(1):23-25.
13. Manoharan G, Singh R, Ahmed B, Kathuria V (2014) Acute spontaneous atraumatic bilateral anterior dislocation of the shoulder joint with Hill-Sachs lesions: first reported case and review of literature. BMJ Case Rep 1757-790X
14. Shiber JR, Diaz JA, Bohsali KI (2014) Bilateral Anterior Shoulder Dislocations due to Seizure. Trop Med Surg 2:160.
| How to Cite This Article: Wheelton A, Dowen D. A Case of Bilateral Anterior Gleno-humeral Dislocation Following First Time Seizure. Journal of Orthopaedic Case Reports 2015 April-June;5(2): 38-40. Available from: https://www.jocr.co.in/wp/2015/04/20/2250-0685-269-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


