
[box type=”bio”] What to Learn from this Article?[/box]
Although tuberculous tenosynovitis is more common etiology for swelling over wrist , gout must be among the differentials irrespective of hyperuricemic status.
Case Report | Volume 5 | Issue 2 | JOCR April-June 2015 | Page 66-68 | Ravi Kumar, VK Sahni, Siddharth Jauhar. DOI: 10.13107/jocr.2250-0685.278
Authors: Ravi Kumar[1], VK Sahni[1], Siddharth Jauhar[1]
[1] Department of Orthopaedics , Maharaja Agarsen Hospital , Delhi. India.
Address of Correspondence
Dr Ravi Kumar
203/5 – Pal Mohan Apartment , Club Road , Punjabi Baugh – West , New Delhi-110026. India.
Email: k2.drravi@gmail.com
Abstract
Introduction: Tophi can present as a first sign of hyperuricemia but literature has limited reports as far as flexor tendon contracture presenting as a first clinical sign of gout is concerned. We report a case of tophaceous gout with finger flexion contracture as its first sign.
Case Report: A 45 years old man presented in our out patient department with complaint of inability to extend middle finger of his left hand along with a mass growing over volar aspect of forearm for over few months . On physical examination a firm – hard mass around 2*2 cm was found over volar aspect of forearm just proximal to flexor retinaculam. MRI showed mass within tendon of FDS. Clinical suspicion of TB tenosynovitis, was kept as a first diagnosis followed by soft tissue neoplasm and subsequently surgical exploration was performed. A whitish chalky infiltration of tendon of FDS, synovial adhesion of other tendons along with median nerve embedded within hypertrophied synovium of flexor tendon noted. Patient underwent synovectomy and excision of tendon of FDS to middle finger Following histo-pathological evaluation a diagnosis of tophaceous gout was made with serum uric acid level being 8.6 mg/dl.
Conclusion: A review of the literature reveals that gouty arthritis of the wrist is rare in isolation. Gout at the wrist as the initial appearance of the condition occurs between 0.8 to 2% of all gout cases. Gout occurs when serum uric acid levels are persistently higher than 6.8mg/dl. Since tophaceous gout can be seen scarcely in well controlled hyper-uricaemic patient thus making preoperative diagnosis of intratendinous tophi even more strenuous.
Keywords: Contracture, tophaceous gout, flexor digitorum superficialis tendon, tendinous infiltration.
Introduction
Gout is an inflammatory arthritis caused by cellular deposition of monosodium urate crystal. Tophi are chalky, gritty accumulations of monosodium urate crystals that build up in soft tissue of an untreated gouty joint. The peak incidence of gout is between the ages of 30–50 with the prevalence increasing with age [1]. Gout is five times more common in men. Tophi can present as a first sign of hyperuricemia but literature has limited reports as far as flexor tendon tophaceous infiltration presenting as a first clinical sign of gout is concerned [2-4].
We report a rare case in which intratendinous tophaceous gout within the flexor digitorum superficialis (FDS) tendon could not be differentiated from tubercular tenosynovitis or neoplasm preoperatively more so as it was seen in a patient with no prior history suggestive of hyperuricemia.
Case report
A 45 years old man presented in our out patient department with complaint of inability to extend middle finger of his left hand along with a mass growing over volar aspect of forearm for over 2 months [Fig 1]. There was previous history of pain at wrist on finger movement which subsided gradually along with the decline in extension of middle finger. There was no associated history of fever, loss of weight or appetite, night sweats, malaise or fatigue. There was no history of trauma, pain in other joints of the body, morning stiffness of the back or hand joints, or continuous use of vibratory tools.
On physical examination a firm – hard mass around 2 * 2 cm was found over volar aspect of forearm just proximal to flexor retinaculam. It was non tender, non compressible, mobile at right angle to anatomical axis of forearm. Movement at wrist was normal with restriction of movement of middle finger in sagittal plane.
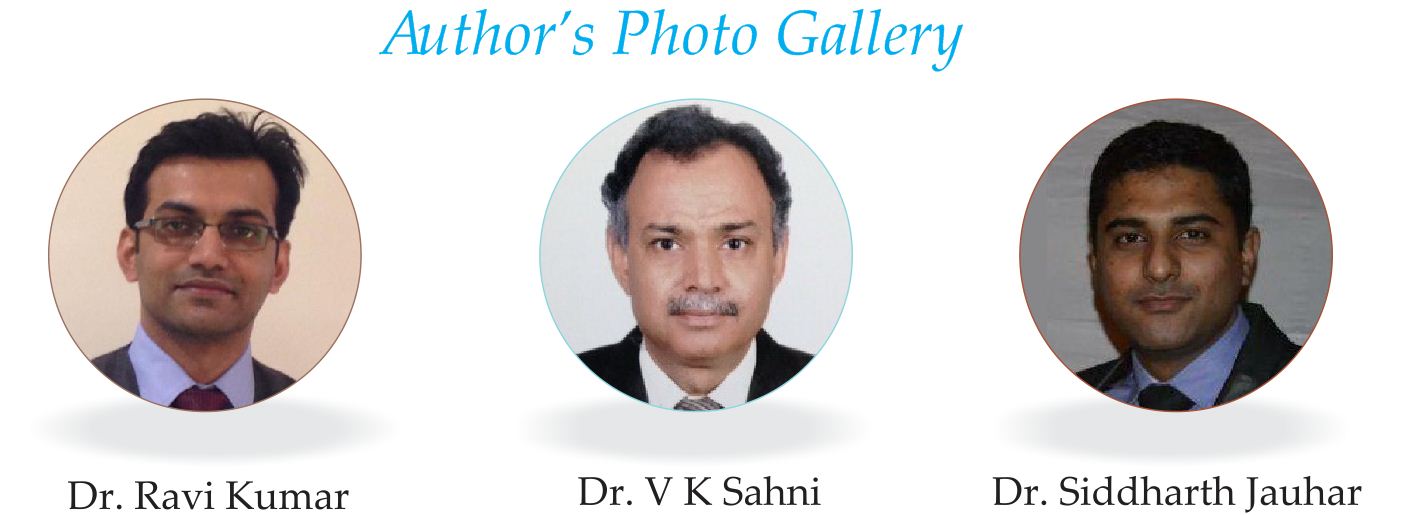
Laboratory findings showed all within normal limits except serum uric acid which was 8.6 mg/dl. And that brought a diagnosis of gouty tophi as among differentials. Findings on chest X-rays were normal. Right wrist joint X-ray showed no significant findings. Magnetic resonance imaging (MRI) showed that the mass was within the FDS which on axial T1 [Fig 2 ] appeared as heterogenous isointense lesion while on coronal T2 STIR [Fig 3]showed heterogenous mixed hypointense – hyperintense lesion. 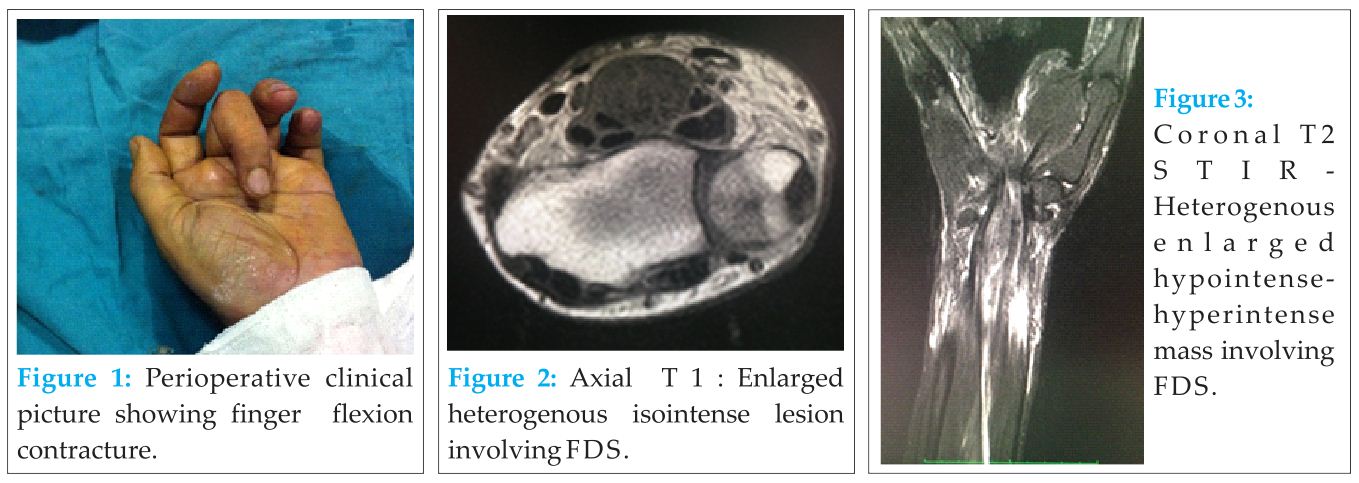 Clinical suspicion of Tubercular tenosynovitis, soft tissue neoplasm and tophaceous gout was made and subsequently surgical exploration was performed.
Clinical suspicion of Tubercular tenosynovitis, soft tissue neoplasm and tophaceous gout was made and subsequently surgical exploration was performed.
The patient was operated under brachial block. An incision along the flexor crease, extending further proximally while maintaining the longitudinal orientation taken. On longitudinal slit of thickened tendon sheath chalky white liquid emanated. On futher exploration there was whitish chalky infiltration of tendon of FDS [Fig 4], synovial adhesion of other tendons along with median nerve embedded within hypertrophied synovium of flexor tendons. Since the mass was noted well proximal to flexor retinaculam that probably could be the reason for flexor contracture and sparing of median nerve. Patient underwent synovectomy and tenotomy of FDS to middle finger because of heavy intratendinous infiltration of the tophus along with destruction of the tendinous tissue.
Histopathological evaluation of the chalky white substance showed fibroconnective tissue showing hyalinized areas with evidence of saponification surrounded by palisades of foreign body type giant cells and chronic inflammatory cells. Needle like crystals are also seen [Fig 5]. All findings were consistent with the diagnosis of tophaceous gout. The postoperative course was uneventful with no remarkable functional deficit from the removal of the superficialis endon to the middle finger [Fig 6] .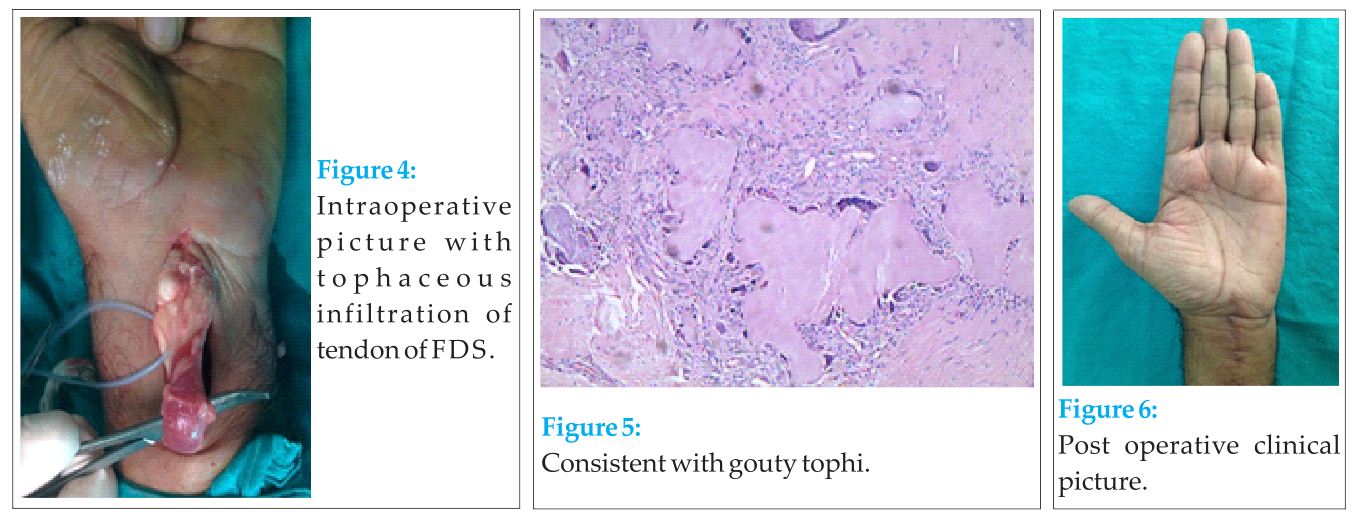
Discussion
Gout at the wrist as the initial appearance of the condition occurs between 0.8 to 2% of all gout cases. Gout patients who are not treated have a 19–30% chance of developing gout in the wrist during their lifetime [5]. Gouty tophi presenting as mass are uncommon and often mistaken for a neoplasm. These nodules may not be recognized as tophi because the clinical diagnosis of gout in many instances is not straightforward. In the past reports, all intratendinous infiltrations of tophaceous gout occurred at the wrist and existed with carpal tunnel syndrome. We present an uncommon and unusual case of gout in the flexor tendon of forearm which occurred in isolation in a patient with no prior medical history of the recorded disease. Measurement of serum uric acid level in chronic tophaceous gout may or may not be conclusive of hyperuricemia as some patients with diabetes or even alcoholics can have normal to lower levels [ 6,7 ]
Although FNAC prior to definitive intervention would have helped us to achieve the diagnosis preoperatively but rather we had gone for definitive intervention but in no way over riding the role of FNAC as the procedure of choice to achieve definitive diagnosis [8 ]. Surgical intervention like tenotomy or tenosynovectomy are required to debulk tophaceous deposits , improve smooth gliding of tendon and decompress nerves but primarily medical management to treat gout remains the gold standard . Short-term outcomes are consistently good [9,10] but the risk of rupture [ 11 ] or recurrency remain if medical control is not achieved.
Conclusion
A review of the literature reveals that gouty arthritis of the wrist is rare in isolation. Gout at the wrist as the initial appearance of the condition occurs between 0.8 to 2% of all gout cases. Gout occurs when serum uric acid levels are persistently higher than 6.8mg/dl. Since tophaceous gout can be seen scarcely in well controlled hyper-uricaemic patient thus making preoperative diagnosis of intratendinous tophi even more strenuous.
Clinical
In Indian subcontinent tubercular tenosynovitis should be the first diagnosis followed by neoplasm and tophaceous gout. Tophaceous gout must be among the differentials even in absence of history of hyperuricemia.
References
1. Monu JUV, Pope TL: Gout: a clinical and radiologic review. RadiologicClinics of North America 2004, 42:169-184.
2. Mackford BJ, Kincaid RJ, Mackay I. Carpal tunnel syndrome secondary to intratendinous infiltration by tophaceous gout. Scand J Plast Reconstr Surg Hand Surg. 2003;37:186–7.
3. Pai CH, Tseng CH. Acute carpal tunnel syndrome caused by tophaceous gout. J Hand Surg. 1993;18A:667–9.
4. Weinzweig J, Fletcher JW, Linburg RM. Flexor tendonitis and median nerve compression caused by gout in a patient with rheumatoid arthritis. Plast Reconstr Surg. 2000;106:1570–2.
5. Raimbeau G, Fouque PA, Cesari B, Le Bourg M, Saint-Cast Y: Arthropathie goutteuse du poignet a propos de cinq cas. Chirurgie de la Main 2001, 20:325-31.
6. Sah SP, Rani S, Mahto R. Fine needle aspiration of gouty tophi: a report of two cases. Acta Cytol 2002:46:784-5.
7. Rege J, Shet T, Naik L. Fine needle aspiration of tophi for crystal identification in problematic cases of gout. A report of two cases. Acta Cytol 2000;44:433-6.
8. Liu K, Moffatt EJ, Hudson ER, Layfield LJ. Gouty tophus presenting at a soft tissue mass diagnosed by fineneedle aspiration: a case report. Diagn Cytopathol. 1996; 15:246–9.
9. Moore JR, Weiland AJ. Gouty tenosynovitis in the hand. J Hand Surg Am. 1985; 10(2):291–295.
10. Rand B, McBride TJ, Dias RG. Combined triggering at the wrist and severe carpal tunnel syndrome caused by gouty infiltration of a flexor tendon. J Hand Surg Eur Vol. 2010; 35(3):240– 242. doi:10.1177/1753193409357374 .
11. Meyer zu Reckendorf G, Lupascu D. Flexor tendons involvement in gout. A case report and review of literature [published online ahead of print May 15, 2010] [in French]. Chir Main. 2010; 29:199–202. doi:10.1016/j.main.2010.04.004 .
| How to Cite This Article: Kumar R, Sahni VK, Jauhar S.Finger Flexion Contracture: First Manifestation of Gout. Journal of Orthopaedic Case Reports 2015 April-June;5(2): 66-68. Available from:https://www.jocr.co.in/wp/2015/04/20/2250-0685-278-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


