
[box type=”bio”] What to Learn from this Article?[/box]
Compartment syndrome is an orthopaedic emergency, however even in cases with delayed presentation useful function can be preserved with adequate decompression.
Case Report | Volume 5 | Issue 2 | JOCR April-June 2015 | Page 75-77| Matt DA Fletcher. DOI: 10.13107/jocr.2250-0685.281
Authors: Matt DA Fletcher[1]
[1] Department of Orthopaedic, Dawson Creek Hospital, Dawson Creek BC Canada.
Address of Correspondence
Dr. Matt DA Fletcher,
Consultant Orthopaedic Surgeon, Dawson Creek Hospital, Dawson Creek, BC V1G 3W8, Canada.
E-mail: matt.fletcher@northernhealth.ca
Abstract
Introduction: Compartment syndrome of the arm is rare, and delay in diagnosis or treatment can be devastating. A case is reported of compartment syndrome of the whole arm occurring in a remote location and arrival at hospital 15 hours after injury with good results despite delayed treatment.
Case Report: A 26 year old male presented with a combined crush injury and compartment syndrome of the arm, with delay in presentation due to remote injury and delay in rescue. Late (>16 hours) fasciotomy was performed with retention of the upper arm, elbow and proximal forearm with good residual function.
Conclusion: Despite significant delay in treatment of compartment syndrome of the arm, useful function and tissue can be preserved with adequate decompression.
Keywords: Crush Injury, Compartment Syndrome, Fasciotomy.
Introduction
Compartment syndrome is a well-recognised complication of trauma, soft tissue injury and certain metabolic conditions[1,2]. It can occur within any myofascial compartment, but is commonly seen within the lower leg, and less frequently within the forearm[4]. Rarely it can affect the hand and foot. Case reports exist of compartment syndrome affecting the upper leg, upper arm, shoulder and pelvis [1,2,6].
Traditional teaching is that compartment syndrome should be recognized and treated with a high index of suspicion and that decompression should be carried out if there is any suggestion of the condition being present [3]. Over recent years, management protocols have been refined, and the gold standard is now to perform diagnostic compartmental pressure monitoring [7]. Delay in decompressing compartment syndrome has a devastating effect, and that in the presence of significant muscle loss the limb may be useless[8,9,10]. A case is presented of a compartment syndrome of the upper limb in association with a crush injury of the forearm whose presentation was significantly delayed due to injury occurring in a remote region with difficulty locating the patient by the emergency services.
Case report
A 26 year old oilfield worker was involved in a roll-over motor vehicle accident on a logging road, and was trapped within his vehicle following injury. His forearm was crushed by the dash, and he was trapped for 13 hours before he was located and extricated by the emergency services. On arrival at the regional unit 15 hours after injury, he was noted to have an intact airway and neck, regular breathing, and was haemodynamically stable. He was catheterised and noted to have myoglobinuria. There was evidence of a crush injury of the upper limb, with complete loss of all sensation and motor power distal to the shoulder. Peripheral pulses were intact. There were no ipsilateral bony injuries. An associated extracranial hematoma was noted.
Urgent CT was performed to rule out intracranial and intraabdominal injury and his cervical scan was cleared. Compartment pressures were measured and noted to be 94mmHg in the flexor compartment of the forearm, 48mmHg in the extensor compartment of the forearm, 40mmHg in both biceps and triceps compartments, and 24mmHg in the shoulder region. His plasma Creatinine Kinase was noted to be 59,000 units/l and Lactate Dehydrogenase 2000 units/l. Urinary diuresis and alkalinisation were commenced immediately.
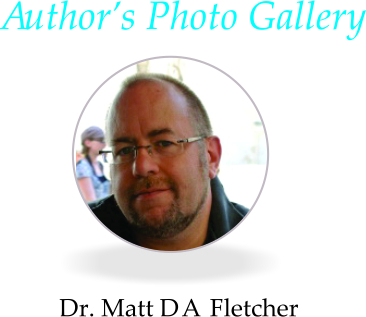
He was taken to theatre after compartment pressures were performed for fasciotomy of the upper limb. Long incisions were made over the volar aspect and extensor aspects of the forearm. Within the flexor compartment of the forearm, the muscle was non-reactive and clinically ischaemic. Within the extensor compartment of the forearm, a similar picture of pinpoint haemorrhage, ischaemia and lack of reactivity to electrical stimulation was noted. In the biceps compartment, there was pallor of biceps brachii, with mild reactivity, and ischaemia of brachialis. The medial neurovascular bundle was grossly swollen with tight fascia. This was released. The extensor compartment of the upper arm showed bleeding into the tissues and minimal reactivity to electricity. All compartments were fully released.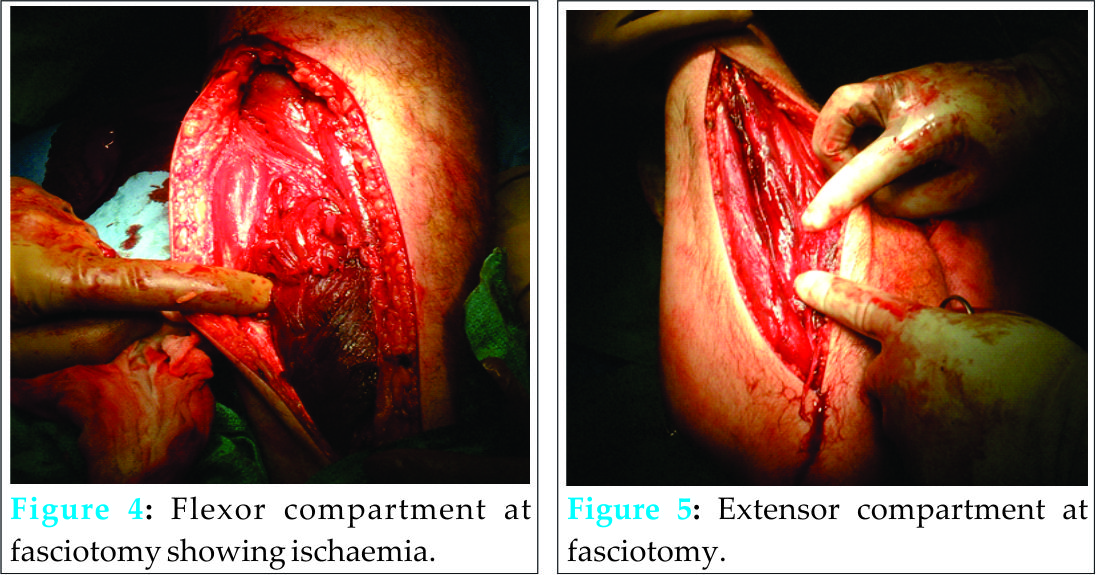
Plans were made for repeat inspection of the arm 48 hours following surgery for debridement. However, renal function deteriorated rapidly with plasma creatinine rising to 600 despite falling CK levels. This was attributed to acute tubular necrosis following the rhabdomyolysis. He was transferred out to the supraregional centre for dialysis. On wound inspection at the renal unit, he was noted to have necrotic tissue within the forearm with sparing of the proximal aspects of the compartment, with viable upper arm muscles. He underwent elective below elbow amputation with a preserved elbow joint and distal stump. Final information received from the tertiary centre six weeks following presentation indicated that upper arm and elbow function was rehabilitating and had some useful function.
Discussion
Compartment syndrome usually presents within six hours of an injury or surgery. Rarely, onset can be delayed, up to six weeks after index injury[4]. The pathophysiology of compartment syndrome is well understood. Diagnosis has historically been on clinical grounds, but current recommendations are to perform compartment pressure monitoring, either by proprietary monitors (Stryker, UK), or by simple techniques[7]. The clinical diagnosis in an unconscious patient has been shown to lack accuracy [8], and due to the medicolegal implications of unnecessary fasciotomy, if immediately available, rapid compartment pressure monitoring is recommended [8]. The treatment of compartment syndrome is urgent fasciotomy[5]. The muscle necrosis occurring as a result of compartment syndrome is typically considered to be complete at six hours from onset, delay in fasciotomy is associated with massive necrosis and progression to amputation or ischaemic contracture [2,3,10,11].
In this case, despite significant delay, primary fasciotomy was performed and muscle in all compartments of the upper limb deemed ischaemic. However, given the widespread muscle injury, initial amputation was not performed and the wound reinspected. Whilst this revealed significant areas of irreversible necrosis, the majority of the musculature in the upper arm was viable, and the patient retained the greater part of the arm, undergoing only below elbow amputation.
The surgical procedure of fasciotomy is not technically demanding. It requires full release of all fascial envelopes in the affected extremity. In a remote location with operating capabilities early decompression by a less experienced surgeon is preferable to late decompression by a sub-specialist. The diagnosis of compartment syndrome should be considered in any individual with a fracture or crush injury to a part of the body containing muscle encapsulated in fascia, and who presents with pain out of keeping with the soft tissue injury, loss of nerve function or peripheral pulses, which is a very late sign and poor prognosticator of outcome [2,12]. Compartment pressure monitoring should be performed [7].
This case suggests muscle recovery following compartment syndrome may be greater than previously recognized [10,11], and whilst emergent fasciotomy remains treatment of choice for early diagnosis, even in the presence of a significant delay, an expectant attitude to muscle recovery should be considered, and emergent amputation only performed in the presence of frank necrosis. Williams et al [13] confirmed the benefit of fasciotomy even after 12 hours in achieving limb salvage, however Finkelstein [14] in a series of 5 patients with compartment syndromes of greater than 35 hours ischaemia reported 4 amputations and one death.
Rhabdomyolysis occurs in crush injuries, and the release of established compartment syndrome combined with crush injury may precipitate acute renal failure [10,11]. Careful monitoring of renal function is critical to ensure that the need for haemofiltration is not neglected.
Conclusion
Compartment syndrome of the upper arm is an emergency. Despite delay in reaching medical care, late decompression can be associated with the retention of some useful function, and the long held maxim that after six hours necrosis is complete may not be entirely true. Forequarter amputation or shoulder disarticulation are disfiguring injuries, preserving viability and even partial function is beneficial to the patient in terms of body image and clothing.
Clinical
Compartment syndrome of the upper arm is rare, and should be considered clinically in the presence of a crush injury. Even delayed management can be successful in preserving useful function.
References
1. Botte MJ, Gelberman RH. Acute Compartment syndrome of the forearm. Hand Clin 1998;14(3):391-403.
2. Kikta MJ, Meyer JP, et al. Crush injury due to limb compression. Arch Surg 1987;122(9):1078-81.
3. Hamlin C. Compartment syndrome in the upper extremity. Emerg Med Clin North Am. 1985; 3(2):283-91.
4. Fletcher MDA, Spicer D, Warren PJ. Delayed Presentation of Compartment Syndrome following Gastrocnemius Tear. Acta Orthopaedica Belgica 2001;67(2): 190-2.
5. Leguit P Jr. Compartment syndrome of the upper arm. Neth J Surg. 1982; 34(3):123-6.
6.Diminick M. Shapiro G, Cornell C. Acute compartment syndrome of the triceps and deltoid. J Orthop Trauma 1999;13(3):2250-7.
7. McQueen M. Acute Compartment Syndrome. Acta Chir Beg. 1998;98(4):166-70.
8. Ulmer T. The clinical diagnosis of compartment syndrome of the lower leg: are clinical findings predictive of the disorder? J Orthop Trauma. 2002 Sep;16(8):572-7. Review.
9. McQueen MM, Court-Brown CM. Compartment monitoring in tibial fractures. The pressure threshold for decompression. J Bone Joint Surg Br. 1996 Jan;78(1):99-104.
10. Mubarak S, Owen CA. Compartment syndrome and its relation to the crush syndrome: A spectrum of disease. A review of 11 cases of prolonged limb compression. Clin Orthop Relat Res. 1975;(113):81-9.
11. Von Schroeder HP, Botte MJ. Crush syndrome of the upper limb. Hand Clin 1998;14(3):451-6.
12. Shaw CJ, Spencer JD. Late management of Compartment syndromes. Injury 1995;26(9):633-5.
13. Williams AB, Luchette FA, Papaconstantinou HT, Lim E, Hurst JM, Johannigman JA, Davis K Jr. The effect of early versus late fasciotomy in the management of extremity trauma. Surgery. 1997 Oct;122(4):861-6.
14. Finkelstein JA, Hunter GA, Hu RW. Lower limb compartment syndrome: course after delayed fasciotomy. J Trauma. 1996 Mar;40(3):342-4.
| How to Cite This Article: Matt DA Fletcher. Decompression of Neglected Compartment Syndrome of the Arm. Journal of Orthopaedic Case Reports 2015 April-June;5(2): 75-77. Available from: https://www.jocr.co.in/wp/2015/04/20/2250-0685-281-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


