
[box type=”bio”] What to Learn from this Article?[/box]
Non-traumatic myositis ossificans is a deceptive tumor which requires precarious work up for diagnosis and apt treatment at complete maturation of tumor.
Case Report | Volume 5 | Issue 3 | JOCR July-Sep 2015 | Page 15-17 | Yashwant J Mahale, Chaitanya S Vyawahare, Nandkishore V Dravid, Aditya Upase, Romil Rathi. DOI: 10.13107/jocr.2250-0685.296.
Authors: Yashwant J Mahale[1], Chaitanya S Vyawahare[1], Nandkishore V Dravid[2], Aditya Upase[3], Romil Rathi[4].
[1] Degree Sneh nagar, Dhule, Maharashtra, India- 424001.
[2] Department of Pathology, ACPMMC, Dhule. Maharashtra. India.
[3] Department of Orthopaedics, Chintamani hospital and Research Centre, Pune-Solapur National highway, Koregaon Mul, Pune. India.
[4] Department of Spine, Dinanath Mangeshkar Hospital, Kothrud, Pune. India.
Address of Correspondence
Dr. Chaitanya S. Vyawahare
FB-3 Indra Sarita Apartment, Balraj Road, Dhantoli, Nagpur, India- 440012.
E-mail: chaitanya.vyawahare@gmail.com
Abstract
Introduction: Myositis ossificans circumscripta is a benign non neoplastic ossifying tumor presenting with bone like osteoid tissue extraskelletaly amidst the muscle planes. This condition when not associated with trauma is very trivial and considering the way it mimics certain characteristics, it may be misunderstood as a malignant neoplasm, abscess or antibioma. The aetiology of this atraumatic condition is still indistinct and remains a question unsolved. We would like to report such a case with distinctly unusual presentation that occurred in our institute. Thereby help in understanding the characteristics of the tumor and associated problems in the diagnoses and treatment.
Case Report: We report a case of 18 year old male presenting with acute onset severe pain in right gluteal region and associated swelling with no history of trauma. All possible investigations including haematological work up, Radiographs, Ultrasonography, aspiration and Magnetic resonance imaging proved to be inconclusive. Open excision and histopathology revealed the condition as myositis ossificans.
Conclusion: Our report is aimed towards understanding the difficulty in diagnosing atraumatic myositis ossificans circumscripta and aid in understanding the possible aetiology of unusual presentation without history of trauma.
Keywords: Atraumatic myositis ossificans circumscripta, extra skeletal osteoid tissue, right gluteal region.
Introduction
Myositis ossificans circumscripta, is an extra-osseous non-neoplastic benign heterotropic ossification. It has been frequently found in muscles of upper and lower limb predominantly in bulky muscles like quadriceps and brachialis[1] Most of these cases are attributed to a prior unrecognized trivial trauma. In patients with definitely no history of trauma or massage, underlying systemic diseases like haemophilia causing haemmorhage which later ossify may be suspected. The real problem lies in concluding towards a definite diagnosis[2]. Even though with the advent of modern techniques such as X-ray, Magnetic Resonance imaging, Ultrasonography, aspiration cytology, it is very complex to differentiate it from malignancy[2] and infective pathology. Biopsy and excision of the tumour mass is often advocated for confirmation of diagnosis[3]. It is therefore the need of time to investigate and scrutinize the deceiving presentation and idiopathicity of this condition occurring without any trauma or underlying systemic illness. We report a case of myositis ossificans circumscripta, a calcified mass underneath the gluteal muscles of right side. Diagnosis was confirmed on open excision and biopsy.
Case Report
An 18 year old male, Muslim by religion, student by occupation, residing in rural region of North West Maharashtra presented in our institute with pain in the right hip region since 1 week. Pain was continuous type, acute in onset, throbbing in nature initially relieved on analgesics. There was history of fever on and off for one and half months, Pain was associated with swelling and induration. On physical examination, swelling was tender, non fluctuant, Trans illumination was negative, non-pitting. No bony mass was palpable due to bulk of gluteal muscles. Local temperature was slightly raised. Patient had selective restriction of movements and associated pain at hip joint with flexion possible up to 80 degrees and internal rotation restricted to 10 degrees. All other movements were normal. There was no previous history of trauma or massage. No history of systemic illness. No similar complaints in family or any hereditary trait. A general surgery opinion was sought, the surgeon opined of it being a deep seated abscess as the patient had history of fever, pain, induration, restricted movements with supportive MRI report. The patient underwent the following investigations.
Investigations
The laboratory blood investigations were done with reports as Hb – 10.2, WBC – 11400, ESR – 30, Deranged PT – 17 sec, INR 1.4, control – 14 sec. Radiographs were taken, AP and Lateral views (Fig 1),(Fig 2) which were inconclusive. Ultrasonography (Fig 3) with 7.5Mhz linear probe revealed a hypoechoic solid mass with linear calcifications within, seen in gluteal muscle plane of size 65 x 42 cm. Aspiration was done with 18 gauge needle, aspirate was blood and sent for cytology, culture and sensitivity. Aspirate was reported as sterile, ruling out any infection or malignancy. Magnetic resonance imaging (Fig 4) showed evidence of large loculated collection in right gluteal region just posterior to greater trochanter of size 3.9 x 4.3 cm, collection was hyperintense on T1 and STIR images, hypointense on T2 images suggestive of an abscess.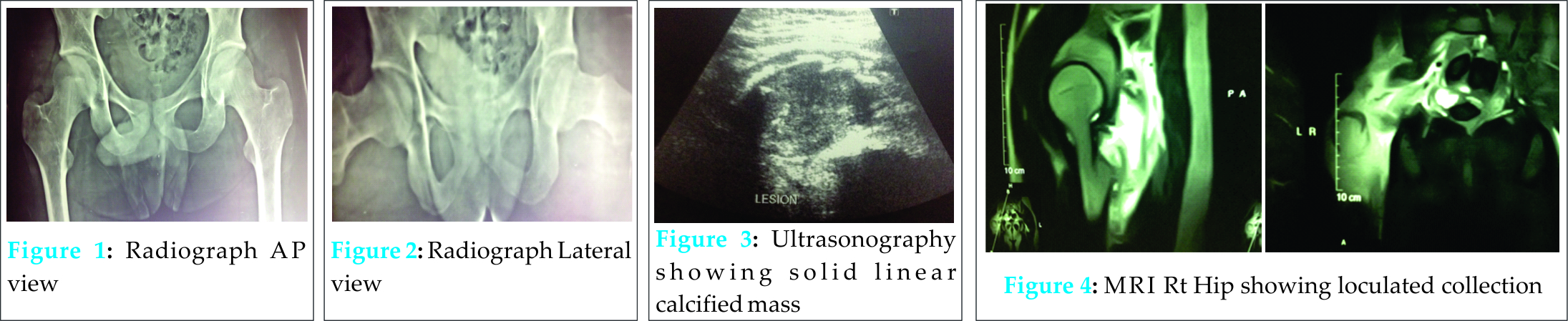
The patient was operated primarily assuming as abscess for incision and drainage. A mass of bony consistency was noticed between the gluteal muscles and external rotators (Fig. 5 & 6). The mass was excised and sent for histopathology.  On histopathological evaluation. Gross appearance (Fig. 7) showed non capsulated, irregular mass of size 6 x 5 x 3 cm, firm consistency, friable bony tissue with central area showing brownish haemorrhagic and necrotic areas. On microscopy, (Fig 8 & 9) (a) central zone showing congested capillary network showing plump endothelium surrounded by zonal proliferation of fibroblasts merging with peripheral bone forming osteoblastic elements and cartilage. (b) Peripheral area showing ill defined trabeculae lined by osteoblasts diagnostic for myositis ossificans.
On histopathological evaluation. Gross appearance (Fig. 7) showed non capsulated, irregular mass of size 6 x 5 x 3 cm, firm consistency, friable bony tissue with central area showing brownish haemorrhagic and necrotic areas. On microscopy, (Fig 8 & 9) (a) central zone showing congested capillary network showing plump endothelium surrounded by zonal proliferation of fibroblasts merging with peripheral bone forming osteoblastic elements and cartilage. (b) Peripheral area showing ill defined trabeculae lined by osteoblasts diagnostic for myositis ossificans.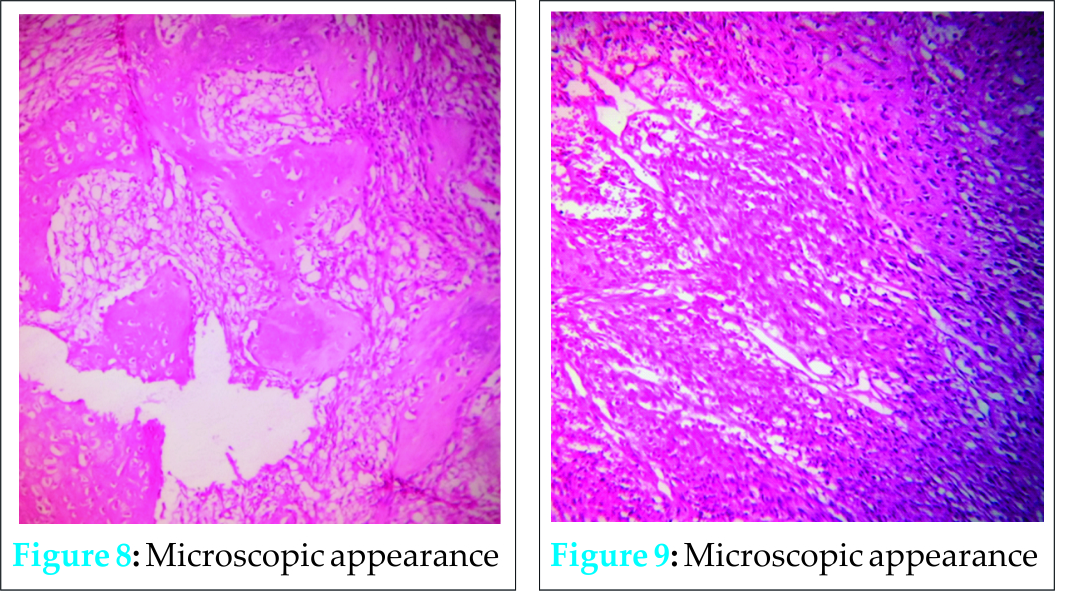
Discussion
Non traumatic myositis ossificans circumscripta is benign non neoplastic generation of bone tissue extra-osseously in muscle plane. It is more common in males and the peak incidence is in active population within second and third decade[4]. In non traumatic cases possible aetiologies may be high calcium and protein content diet of those consuming red meat, repeated microtrauma to gluteal region, post intramuscular injection, drug abuse. Myositis ossificans is dynamic. The clinical, imaging and cytological pictures keep of changing as the stages advance. A diagnosis in early stage is very difficult as it is tricky to differentiate between infective pathology, malignancy and myositis ossificans. With every stage, the clinical picture mimics one of the above mentioned conditions, and also various non invasive routinely preferred techniques like X-Ray, MRI are often inconclusive unless clinical co relation is strongly positive. Investigations Fine needle Aspiration cytology are also often confusing and non conclusive. These changes easily mislead towards advocating of inapt or untimely intervention. Confirmation of diagnosis is thus extremely important before proceeding to intervention[5] . MRI is always preferred modality of investigation as it gives a better picture in relation to its association with soft tissue involvement and its vascular parameters. For early stage lesions, T2-weighted images show a heterogeneous localized mass with high signal intensity in the central area. As the lesion matures, the peripheral ossification becomes denser, and the T2-weighted MRI shows a hyperintense area with surrounding hypointense rim. On T1-weighted images, the lesion is isointense to the muscle and can be identified by mass effect but it may demonstrate rim enhancement in the acute phase after contrast administration[1]. Histopathology is the mainstay of confirmatory diagnosis. The method of taking a biopsy specimen is very important. The specimen sample should contain three layers precisely as central, middle and peripheral zone. Myositis typically exhibits a zonal picture with central zone showing variably sized congested capillary network showing plump endothelium surrounded by zonal proliferation of fibroblasts merging with peripheral areas of bone forming osteoblastic elements and cartilage. Individual fibroblasts show ill defined tapering processes with eosinophilic cytoplasm and oval nuclei. Stroma shows myxoid, collagenous vascular and oedematous areas with infiltration of sparse chronic inflammatory cells. Peripheral areas show ill defined trabeculae lined by osteoblasts. Absence of mitotic figures and cytologic atypia with no reverse zoning phenomenon differentiate it from extra osseous osteosarcoma[6]. In early stages when the myositis is not matured, Conservative treatment with indomethacin and aspirin drug, acetic acid iontophoresis, magnesium therapy, and etidronate disodium have also been reported to be effective. The most common treatment of MOC is a surgical excision when it is completely matured.
Conclusion
Non traumatic Myositis ossificans circumscripta is a rare trivial disease with unusual and confusing presentation. It is generally found in bulky muscle planes with predominance in younger active population. In early stages it mimics a malignant neoplasm or a deep seated abscess and misguides the plan of treatment. Therefore Clinical presentation, Investigations, imaging techniques and histopathology should be co related for a definite diagnosis and apt treatment.
Clinical Message
The occurrence of myositis ossificans circumscripta without trauma is rare. It is very difficult to diagnose with its everchanging clinical and imaging picture. Thorough history, clinical examination and precise imaging along with histopathology are to be co related for a diagnosis and apt treatment.
Reference
1. Wang X.L., Malghem J., Parizel P.M., et al; Myositis ossificans circumscripta; JBR–BTR, 2003, 86: 278-285.
2. Aneiros-Fernandez J, Caba-Molina M, Arias-Santiago S, et al; Myositis ossificans circumscripta without history of trauma.; J Clin Med Res. 2010 May 19;2(3):142-4.
3. Saussez S, Blaivie C, Lemort M, et al; Non-traumatic myositis ossificans in the paraspinal muscles; Eur Arch Otorhinolaryngol. 2006 Apr;263(4):331-5. Epub 2005 Aug 24.
4. Arends JE, Drillenburg P, van der Woude HJ, et al.; Non-traumatic myositis ossificans circumscripta in the teres major muscle; Ned Tijdschr Geneeskd. 2003 Apr 19;147(16):768-71.
5. Nuovo MA, Norman A, Chumas J, et al; Myositis ossificans with atypical clinical, radiographic, or pathologic findings: a review of 23 cases.; Skeletal Radiol. 1992;21(2):87-101
6. Lagier R, Cox JN; Pseudomalignant myositis ossificans. A pathological study of eight cases; Hum Pathol. 1975 Nov;6(6):653-65.
| How to Cite This Article: Mahale YJ, Vyawahare CS, Dravid NV, Upase A, Rathi R. A Rare Case Of Non Traumatic Myositis Ossificans Circumscripta. Journal of Orthopaedic Case Reports 2015 July – Sep;5(3): 15-17. Available from: https://www.jocr.co.in/wp/2015/07/10/2250-0685-296-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


