
[box type=”bio”] What to Learn from this Article?[/box]
Double Osteotomy With DHS Fixation For Shepherd’s Crook Deformity Of Femur In A Case Of Fibrous Dysplasia.
Case Report | Volume 5 | Issue 3 | JOCR July-Sep 2015 | Page 41-44 | Kandhari VK, Bava SS, Desai MM, Wade RN. DOI: 10.13107/jocr.2250-0685.304.
Authors: Kandhari VK[1], Bava SS[1], Desai MM[1], Wade RN[1]
[1] Department of Orthopaedics, Seth G. S. Medical College and K. E. M. Hospital. Mumbai. India
Address of Correspondence
Dr. Vikram K. Kandhari
Plot No. 5/ 5a, Pande Layout, Behind Gulmohor Hall, Khamla, Nagpur – 440025. India.
E mail – dr.vikramkandhari@gmail.com
Abstract
Introduction: Fibrous dysplasia is a rare benign disorder of the skeletal system characterized by fibro osseous proliferation with intervening areas of normal or immature bone in the intramedullary region. It can either be a monostotic (involves one bone) or a polyostotic (involves more than one bone) presentation and usually occurs equally in males and females. Deformities like scoliosis and shepherd’s crook deformity are frequently encountered in the polyostotic form. We report a rare managed case of bilateral non-union of the pathological fracture of femur neck with shepherd’s crook deformity of the proximal femur in a case of polyostotic fibrous dysplasia.
Case Report: A 16 years old female case of polyostotic fibrous dysplasia had bilateral Shepherd’s crook deformity of the proximal femur with bilateral non – union of pathological fracture of neck femur. We managed each side in one stage with two osteotomies. On the right side, first oblique osteotomy was done from just distal to the greater trochanter up to the level of the neck and the second; lateral closing wedge abduction osteotomy was done at the subtrochanteric level. 2 months later on the left side double lateral closing wedge abduction osteotomies were performed both at the subtrochanteric level. Fixation of both the sides was done using a 135° Dynamic Richard’s screw with a long side plate to span the osteotomy sites and the lesion.
Post – operatively we achieved a neck shaft angle of 135° on right side and 133° on the left side. Follow up imaging showed union at both the osteotomy sites bilaterally and also at the site of the pathological fracture of neck femur. Presently, at 18 months post – operatively, patient is walking full weight bearing without support and there are no signs of recurrence of lesions of fibrous dysplasia or the deformity.
Conclusion: Double osteotomy is an easy and effective method to correct the shepherd’s crook deformity and achieve correct mechanical alignment. Dynamic hip screw with long side plate is a versatile implant to tackle the proximal femur deformity. Double osteotomy corrects the deformity and tackles the associated problems like non – union of the pathological neck femur fracture in one stage.
Keywords: Fibrous dysplasia; Shepherd’s Crook Deformity; Non union transcervical neck femur fracture; Dynamic Hip Screw.
Introduction
The term “Fibrous Dysplasia” was given by Lichtenstein in 1938[1]. Fibrous dysplasia is a rare benign disorder of the skeletal system. It is the result of the failure of the remodeling of the primitive bone and the failure of the bone to realign in response to the mechanical stress. Also, the immature matrix does not mineralize normally. It is characterized by fibro osseous proliferation with intervening areas of normal or immature bone in the intramedullary region. The combination of lack of stress alignment and lack of mineralization leads to loss of the mechanical strength and development of pain, deformity and pathological fractures. It can either be a monostotic or a polyostotic presentation and usually occurs equally in males and females. It presents mostly in the first two decades of life with polyostotic form showing an earlier presentation. The clinical spectrum of the disease ranges from simple bone enlargement or bone pain to pathological fractures and deformities of bone. Endocrine dysfunction, abnormal pigmentation or precocious puberty in girls may or may not be associated. Almost any bone in the body can be involved but polyostotic form tends to involve the craniofacial bones, ribs and metaphysis or diaphysis of femur and tibia more commonly. Lesions tend to be present on one side of the body. Deformities like scoliosis and shepherd’s crook deformity are frequently encountered in the polyostotic form. The latter deformity is thought to be characteristic of the polyostotic form. It involves curvature in the proximal femur neck and proximal shaft resulting in coxa vara deformity. Many treatment options have been tried for fibrous dysplasia; ranging from simple curettage and bone grafting [2,3] to excision of the lesion and correction of associated deformity. Also, various bone graft substitutes have been tried for the purpose of bone grafting, but none have stood the test of time. The lesions persist either partially or completely inspite of the vigorous treatment and tend to recur [4,5]. However, the associated pathological fractures or the osteotomies done for the correction of the deformity have excellent union rates. So, many osteotomies like the Sofield type Sheekh Kebab osteotomy [6], originally described for osteogenesis imperfecta, have been tried for the correction of the diaphyseal deformities. But they cannot be used for the treatment of the Shepherd’s crook deformity, which is mainly a metaphyseal deformity. The goal of treatment of the shepherd’s crook deformity is to prevent the recurrence by achieving mechanical alignment of the proximal femur and then internally splinting it. Recurrence is common in the managed cases and is more commonly seen with simple curettage and bone grafting. The cases reported in the literature are mostly the unilateral cases with the either a single stage or two stage correction. We report a rare managed case of bilateral non-union of the pathological fracture of femur neck with shepherd’s crook deformity of the proximal femur in a case of polyostotic fibrous dysplasia. To our knowledge such a case has not been reported in the English literature.
Case report
A 16 years old female patient presented to us with inability to walk on both lower limbs since last 3 months. Earlier the patient was able to walk with a limp and would sway to either side while walking. Three months back patient experienced sudden onset pain in her right groin region while walking and the patient was not able to bear weight on her right lower limb. Then patient was walking with support, bearing weight on her left lower limb. In about a week, patient experienced similar pain in her left groin and was not able to bear weight on either lower limb since then and was left bed ridden. Clinical findings were consistent with coxa vara deformity of bilateral hips with a possibility of bilateral non-union of pathological fracture of femur neck. There was no evidence of any endocrine disturbance, or altered pigmentation or precocious puberty. On imaging it was concluded that the patient suffered from polyostotic fibrous dysplasia with bilateral Shepherd’s crook deformity of the proximal femur with bilateral non – union of pathological fracture of neck femur (Fig 1). Imaging of the other bones showed evidence of the fibrous dysplastic lesions in the shaft of left tibia (Fig 2 and 3). Magnetic resonance scanning of the bilateral hip region showed the features consistent with fibrous dysplasia of the proximal femur shaft along with sub – capital fracture of femur neck without evidence of avascular necrosis of the femur head (Fig 4). All the blood and serum biochemical investigations of the patient like the hemoglobin, total and differential white cell counts, erythrocyte sedimentation rate, C – reactive protein, calcium, phosphorus, alkaline phosphatase levels and all the hormonal studies were within normal limits.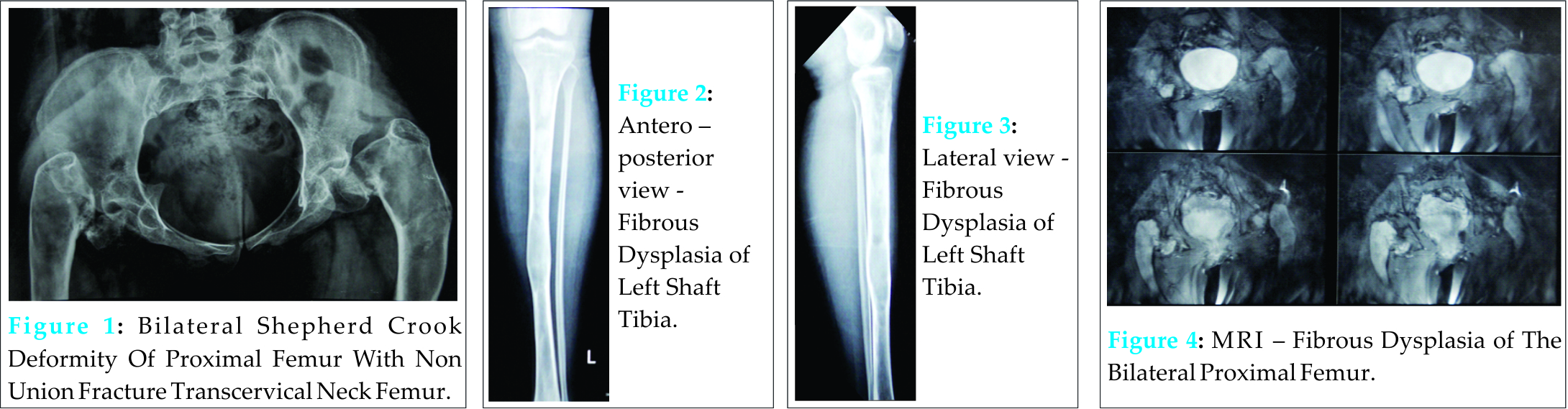
It was decided to do both correction of the deformity to realign the head, neck and shaft; and to achieve valgus at the neck – shaft region and a horizontal configuration neck fracture increasing the chances of union of pathological fracture of neck femur, in one stage, each side at a time. On the right side, first oblique osteotomy was done from just distal to the greater trochanter up to the level of the neck to separate the greater trochanter and the second, lateral closing wedge abduction osteotomy was done at the subtrochanteric level to achieve alignment of the shaft with the proximal femur. With traction neck was aligned to the head and fixed with a 135° Dynamic Richard’s screw with a long side plate. The high riding greater trochanter was aligned with the neck and held with a tension band wire from above and medial to the abductors to hold the greater trochanter aligned.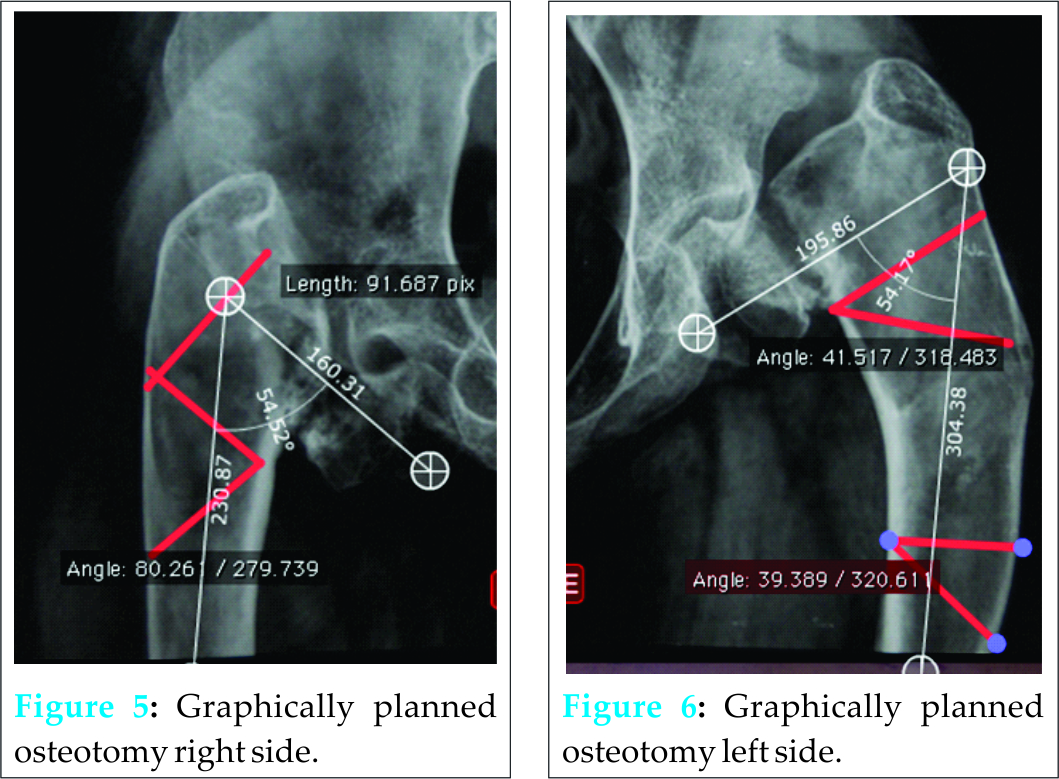
2 months later on the left side double lateral closing wedge abduction osteotomies were performed both at the subtrochanteric level to achieve the valgus at the neck – proximal femur shaft junction and to align the distal shaft with the proximal femur. After full correction the head and neck were aligned and the vertical geometry of pathological fracture neck femur was converted into a more horizontal one increasing the chances of union of the fracture. Fixation was done using a 135° Dynamic Richard’s screw with a long side plate to span both the osteotomy sites. Post – operatively we achieved a neck shaft angle of 135° on right side and 133° on the left side (Fig 5). Patient was started on active and passive quadriceps strengthening exercises and after 6 weeks of immobilization toe touch weight bearing was started followed gradually by partial and complete weight bearing mobilization. Follow up imaging showed union at both the osteotomy sites bilaterally and also at the site of the pathological fracture of neck femur. Presently, at 18 months post – operatively (Fig 6), patient is walking full weight bearing without support and there are no signs of recurrence of lesions of fibrous dysplasia or the deformity.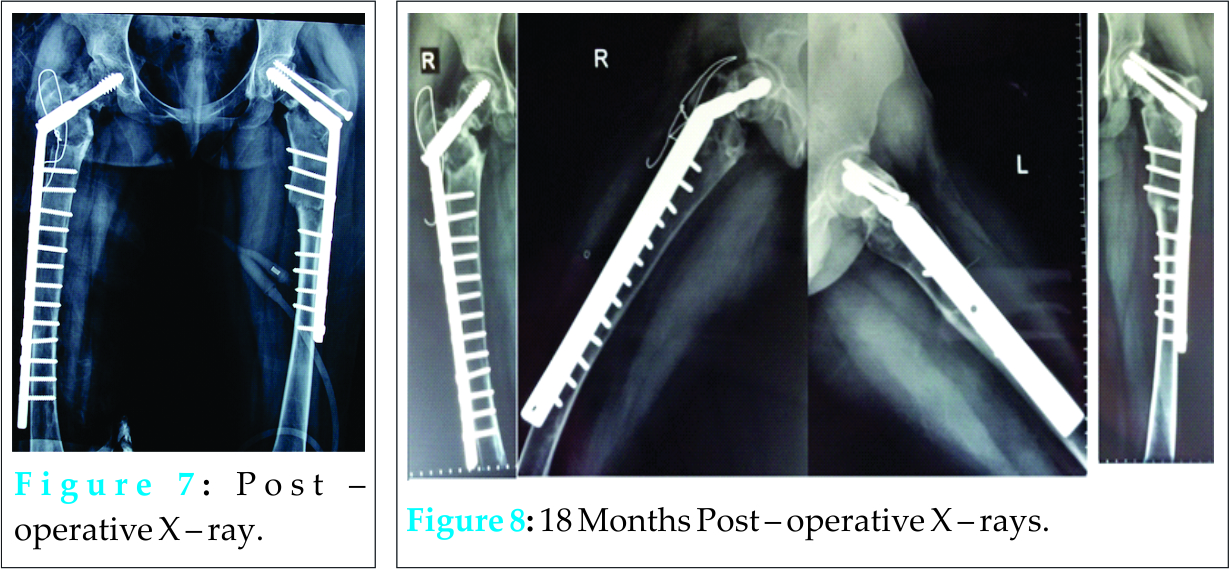
Discussion
Though pathologically fibrous dysplasia is described as a benign condition, clinically it is associated with a significant morbidity and decreased quality of life, especially with lesions of the lower limb; like in our patient. Our patient presented to us in her second decade of life with shepherd’s crook deformity of bilateral proximal femur. She continued to walk full weight bearing inspite of the deformity and developed bilateral fracture of the neck femur, due to excessive mechanical stress in the neck region and was unable to bear weight and walk. Early treatment and rehabilitation in such cases is essential to combat the morbidity and decreased quality of life in such patients. Every time Shepherd’s crook deformity manifests in a different way and at a different stage; thus a tailored approach should be adopted for treating them. This is the reason of having varied ways described of approaching this particular deformity. Irrespective of the customized approach chosen for management of this deformity, it is of utmost importance to achieve the correct alignment and union. Many authors like, T. A. Nagda et al [9], Li W et al [10], Guille et al [7] and Tsuchiya et al [8] have described the various methods for correction of Shepherd’s crook deformity of the proximal femur. But the case we described was unique in the way that, it had associated non-union of pathological fracture of neck femur. Thus, in our case, it was essential to choose a dynamic implant contrary to the intramedullary implant used by T. A. Nagda et al [9]. In our experience, dynamic hip screw fixation provides a more versatile method of fixing the Shepherd’s crook deformity of proximal femur and enhances the chances of union of pathological fracture of neck femur, due to the dynamic collapse permitted by the implant. Our experience is consistent with the results of Li W et al [10] who concluded that, “valgus osteotomy in combination with DHS internal fixation is an easy and effective method for the treatment of fibrous dysplasia with shepherd’s crook deformity, as it can restore the neck-shaft angle and re-establish the mechanical alignment of the femur to improve function”. Also, a desired length of the side plate, depending on the extent of lesion helps to span the lesion completely and prevent recurrence. For the full correction of the deformity and to achieve the desired mechanical alignment, two osteotomies should be used one to correct the neck – shaft alignment and the other to achieve proximal femur – shaft alignment. Only the placement of the osteotomy will vary depending on the extent of the disease and the amount of deformity. Union of the osteotomy is usually not an issue, as once the mechanical alignment is achieved, union is usually achieved. Also, the double osteotomy helps to simultaneously tackle associated problems like non – union of the fracture neck femur while correcting the deformity, as in our case. Correction of the shepherd’s crook deformity in single stage maximizes rehabilitation and also decreases the operative morbidity experienced by patient. It is difficult to achieve single stage correction using an intramedullary implant, and in such cases dynamic hip screw fixation should be preferred. There are higher chances of double osteotomy fixed with intramedullary implant to fail and go in varus collapse [11], compared to the dynamic hip screw fixation. So, the latter is a preferred implant for fixation of double osteotomy.
Thus, double osteotomy with dynamic hip screw fixation is a versatile, effective, easier and a practical approach to correct the morbid Shepherd’s crook deformity of proximal femur. It is also effective to tackle the associated problems in the region of proximal femur; like, non – union of pathological fracture of neck femur. And finally, it permits faster treatment and rehabilitation, which is the prime requirement of the patients with shepherd’s crook deformity.
Conclusion
Double osteotomy is an easy and effective method to correct the shepherd’s crook deformity and achieve correct mechanical alignment of the proximal femur in patients with fibrous dysplasia. Dynamic hip screw is a versatile and preferred implant to tackle the proximal femur deformity in cases of fibrous dysplasia. Using a long side plate with the dynamic hip screw helps to span the lesion and prevent the recurrence of the deformity. Customized approach should be adopted to tackle the proximal femur Shepherd’s crook deformity in cases of fibrous dysplasia. Single stage surgery is preferred correct the shepherd’s crook deformity, in cases of fibrous dysplasia, to maximize rehabilitation and minimize morbidity. Double osteotomy not only corrects the deformity but also tackles the associated problems like non – union of the pathological neck femur fracture.
Clinical Message
Double osteotomy with dynamic hip screw fixation is a versatile, effective, easier and a practical approach to correct the morbid Shepherd’s crook deformity of the proximal femur in patients with fibrous dysplasia. It is also effective tackle the associated problems in the region of proximal femur; like, non – union of pathological fracture of neck femur.
Reference
1. Lichtenstein L. Polyostotic fibrous dysplasia. (1938) Arch Surg 36:874.
2. Enneking WF, Gearen PF; Fibrous dysplasia of the femoral neck, treatment with cortical bone grafting; JBJS Am 1986;68;1415.
3. Stephenson RD, London FD, Hankin FM et al; Fibrous dysplasia, an analysis of options of treatment; JBJS Am; 1987;59A:400.
4. Stewart MJ, Gilmer WS, Edmonson AS (1962) Fibrous dysplasia of bone. J Bone Joint Surg [Br] 44-B:302–318.
5. Harris WH, Dudley HR Jr, Barry RJ (1962) The natural history of fibrous dysplasia. An orthopaedic, pathological, and roentgenographic study. J Bone Joint Surg Am 44-A:207–233.
6. Sofield HA, Page MA, Mead NC. Multiple osteotomies and metal-rod fixation for osteogenesis imperfecta. J Bone Joint Surg. 1952;34A:500-2.
7. Guille JT, Kumar SJ, MacEwen GD (1998) Fibrous dysplasia of the proximal part of the femur. J Bone Joint Surg 80-A(5):648–658
8. Tsuchiya H, Tomita K, Matsumoto T, Watanabe S (1995) Shepherd’s crook deformity with an intracapsular femoral neck fracture in fibrous dysplasia. Clin Orthop Relat Res 310:160–164
9. TV Nagda, H Singh, M Kandoi, A Samant, BR Patel. Two stage reconstruction for the Shepherd’s crook deformity in a case of polyostotic fibrous dysplasia. Journal of Postgraduate Medicine: Year: 1997, Volume:43, Issue:3, Page:83-4.
10. Li W, Huang X, Ye Z, Yang D, Tao H, Lin N, Yang Z. Valgus osteotomy in combination with dynamic hip screw fixation for fibrous dysplasia with shepherd’s crook deformity. Arch Orthop Trauma Surg. 2013 Feb;133 (2):147-52.
11. O’Sullivan M, Zacharin M (2002) Intramedullary rodding and bisphosphonate treatment of polyostotic fibrous dysplasia associated with the McCune-Albright syndrome. J Pediatr Orthop 22(2):255–260.
| How to Cite This Article: Kandhari VK, Bava SS, Desai MM, Wade RN. Single Stage Treatment of Non – Union of Transcervical Neck Femur Fracture with Shepherd Crook Deformity of Proximal Femur in A Case of Fibrous Dysplasia using Dynamic Hip Screw Fixation. Journal of Orthopaedic Case Reports 2015 July – Sep;5(3): 41-44. Available from: https://www.jocr.co.in/wp/2015/07/10/2250-0685-304-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


