
[box type=”bio”] What to Learn from this Article?[/box]
Presentation and Management of an uncommon case of atraumatic anterior neglected bilateral shoulder dislocation.
Case Report | Volume 5 | Issue 3 | JOCR July-Sep 2015 | Page 81-84 | Andrea Poggetti, Iacopo Castellini, Elisabetta Neri, Stefano Marchetti, Michele Lisanti. DOI: 10.13107/jocr.2250-0685.317.
Authors: Andrea Poggetti[1], Iacopo Castellini[1], Elisabetta Neri[1], Stefano Marchetti[1], Michele Lisanti[1]
[1] Department of Orthopaedics and Traumatology, University of Pisa, Italy.
Address of Correspondence
Dr. Iacopo Castellini,
Department of Orthopaedics and Traumatology, University of Pisa, via Paradisa 2, Pisa, 56121, Tuscany, Italy.
Email: iacopocastellini@yahoo.it
Abstract
Introduction: Neglected bilateral anterior shoulder dislocation is a very rare condition, often related to seizures or major trauma. Open reduction is recommended whenever Hill-Sachs lesion is >25% of the joint and the dislocation is elder than 3 weeks.
Case Report: We describe a case report of a 28-year-old man left handed Jehovah’s Witness laborer assessed 12 weeks after bilateral anterior shoulder dislocation. The patient was evaluated with clinical examination, and it was observed an asymptomatic intrarotation of both shoulders with a mild left circumflex nerve deficit. He was able to perform flexion and abduction of both arms up to 60° and 10° of extrarotation. Pre-operative constant scores were 49 in left and 55 in right shoulder, pre-operative disabilities of the arm, shoulder, and hand (DASH) scores were 57 in left and 53 in right shoulder, and visual analogue scales (VAS) was 2. Radiological examination were bilateral anteroposterior shoulder X-rays and computer tomography scan. The surgeon treated both shoulder (not simultaneously) by open reduction and Bristow-Latarjet coracoids transfer procedure. A 1 year after operations, left flexion was 180° while right was 160, bilateral abduction was 180. He was able to return to his pre-injury activities, the constant score was 89 left and 83 right, DASH score was 17 left and 13 right and VAS was 0.
Conclusion: Atraumatic bilateral neglected anterior shoulder dislocation can be treated with open Bristow-Latarjet procedure to provide a stable glenohumeral joint in laborer patient and permit a return to the pre-injury activities, to create a greater extension of the glenoid arc and to avoid future dislocation.
Keywords: Shoulder dislocation, bilateral, Latarjet procedure, shoulder injury.
Introduction
Bilateral anterior shoulder dislocation is rare, because almost always one extremity takes the brunt of the impact during trauma incidence [1,2]. Usually happen almost always secondary to major trauma (50%), affect mainly young men (70%) and it is associated with other injuries (greater tuberosity fractures in 15%, rotator cuff tears, neurological associated lesions) [3,4]. Muscle contractions due to neurological or psychiatric spasm or electrocution were identified like alternative cause. Neglected bilateral anterior shoulder dislocation is very rare condition, often related to seizures or major trauma. For anterior dislocation, open reconstructive options include infraspinatus tendon transfer, disimpaction grafting or allograft repair, Bankart repair and shoulder replacement. The goal of surgical treatment is repair of articular defects and maintenance of shoulder stability to allow an early rehabilitation.
Case report
A 28-year-old male Jehovah’s Witness laborer, affected by iron-deficiency anemia, was evaluated in orthopedic office for restricted mobility and pain (during daily activities) in both shoulders from about 12 weeks. He did not report any trauma in past. There was no history of neurological disease, no drug use or alcohol intake. His family medical history was negative for connective tissue disease or musculoskeletal disorder. He reported that previously these inabilities were interpreted as paraspinal cervical muscle contracture and treated only with muscle relaxant drugs. At the time of evaluation, patient showed mild pain and inabilities in shoulders external rotation and abduction. Physical examination revealed: Bilateral normal internal rotation; bilateral 10° external rotation, abduction and flexion about 60° and axillary nerve numbness. Anteriorposterior X-ray images evidenced bilateral anterior shoulder dislocation and computer tomography-scan showed bilateral Hill-Sachs lesion (<25%) (Fig. 1). 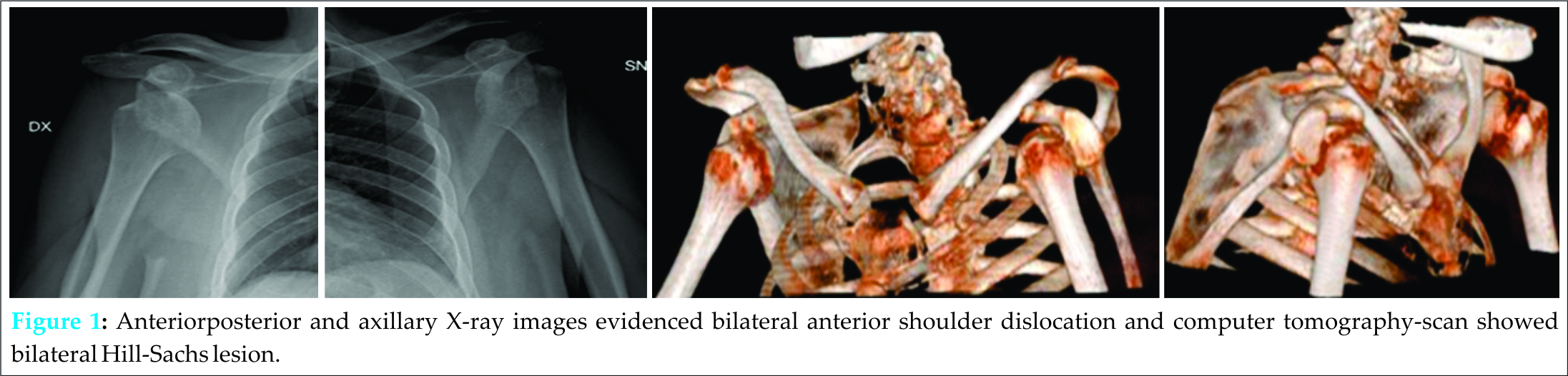 The surgeon suggested a step-by-step surgical treatment conscious about patient’s medical history and refusal of whatever blood transfusion for religious reasons. The first step was surgical treatment of dominant limb and then right side after 1 month. Surgical procedures were both performed under general anesthesia, beach chair position and fluoroscan aid. The deltopectoral approach was used and for both cases were evidenced a glenoid fossa deficiency with hypoplasia of scapular neck and glenoid. Bristow-Latarjet coracoid transfer procedure was performed to repair the anterior glenoid defect. Any posterior capsular release was performed. During surgeries, bleeding was controlled and intraoperative blood salvage was used to accommodate wishes of the patient to refuse homologous and autologous transfusions, as required his confession of faith. Through post-operatively management, shoulders were supported by a sling with 15° of abduction and maintained for 3 weeks. Passive and active movements of hand and elbow were early started. A 4 weeks later, clinical and radiographic evaluation were performed, and the patient was introduced to passive shoulder motion, while 2 weeks later he started an active controlled shoulder motion. He was followed for next 6 months by upper extremities therapist team. The 1 year after last operations, the patient was clinical and radiographical evaluated and he was able to perform left flexion up to 180° and 160 in right, bilateral abduction was 180 (Fig. 2). The constant score was 89 left and 83 right, disabilities of the arm, shoulder and hand (DASH) score was 17 left and 13 right and visual analogue scales were 0.
The surgeon suggested a step-by-step surgical treatment conscious about patient’s medical history and refusal of whatever blood transfusion for religious reasons. The first step was surgical treatment of dominant limb and then right side after 1 month. Surgical procedures were both performed under general anesthesia, beach chair position and fluoroscan aid. The deltopectoral approach was used and for both cases were evidenced a glenoid fossa deficiency with hypoplasia of scapular neck and glenoid. Bristow-Latarjet coracoid transfer procedure was performed to repair the anterior glenoid defect. Any posterior capsular release was performed. During surgeries, bleeding was controlled and intraoperative blood salvage was used to accommodate wishes of the patient to refuse homologous and autologous transfusions, as required his confession of faith. Through post-operatively management, shoulders were supported by a sling with 15° of abduction and maintained for 3 weeks. Passive and active movements of hand and elbow were early started. A 4 weeks later, clinical and radiographic evaluation were performed, and the patient was introduced to passive shoulder motion, while 2 weeks later he started an active controlled shoulder motion. He was followed for next 6 months by upper extremities therapist team. The 1 year after last operations, the patient was clinical and radiographical evaluated and he was able to perform left flexion up to 180° and 160 in right, bilateral abduction was 180 (Fig. 2). The constant score was 89 left and 83 right, disabilities of the arm, shoulder and hand (DASH) score was 17 left and 13 right and visual analogue scales were 0.
Discussion
This case report showed an atraumatic bilateral shoulder dislocation due to an undetermined mechanism. As expressed by other authors, this type of lesion can be present in 4% of all shoulder dislocation, even if the most of cases were related to medical conditions including myasthenia gravis, cerebral palsy and scapular myopathy [5]. Neglected anterior shoulder dislocation is an exceptional condition whose treatment has not guidelines mutually agreed. In our opinion, treatment of this type of lesion depends on many factors: Time of dislocation, age of patient, functional limitation, success of reduction, presence and amount of the Hill-Sachs lesion and glenoid fossa defect and surgeon’s experience. Conservative treatment should be considered in patient without shoulder pain or low functional demands and in case of surgical or anesthesiological contraindications. However, in young, active, high demands patients, conservative choice without stabilization should be not the proper procedure due to possible concurrent Hill-Sachs lesion, to possible concurrent glenoid defect and resulting high risk of instability. Solomon et al. [6] suggested closed reduction only up to 6 weeks post-injury due to high risk of iatrogenic fracture or neurovascular damage. Open reduction is the recommended procedure with Hill-Sachs lesion more than 25% of articular surface and after 3 weeks [7]. For anterior dislocation, open reconstructive options include infraspinatus tendon transfer, disimpaction grafting or allograft repair, Bankart repair and shoulder replacement. The goal of surgical treatment is repair of articular defects and maintenance of shoulder stability to allow an early rehabilitation [8]. Many surgical solutions were proposed like Eden-Hybinette, arthroscopical Bristow-Latarjet procedure but recently, Longo et al. showed how Eden-Hybinette procedure has clinical outcomes very similar to the Bristow-Latarjet with a higher rate of post-operative osteoarthritis and recurrence [9]. Authors treated the young patient with an open Bristow-Latarjet procedure primarily to repair the old dislocation and remedy the glenoid fossa defect. Hill-Sachs lesions were not treated during surgery because involved <25% and intraoperatively glenohumeral joint was stable after reduction. Author’s opinion is to refer surgical treatment of Hill-Sachs lesion in case of lesion involving over 25% of articular surface to maintain glenohumeral stability by open remplissage with the infraspinatus tendon (in this technique the head defect was filled with the infraspinatus tendon, by tying the sutures from the anchor, so bringing the tendon down to the defect) [10] or shoulder arthroplasty if the lesion is over 50% of humeral head. Currently, however, literature reports only few studies about results of operative treatment of chronic anterior shoulder dislocation with arthroplasty and this type of surgery should be considered in selected cases: Elderly patients; intraoperatively instability due to severe humeral head cortical depression and/or glenoid defect and degenerative arthropathy. Gavriilidis recommended this surgical procedure with large head defects and experienced good mid-term results with benefits for a range of motion, pain and patient satisfaction [11]. This case report showed that anterior shoulder dislocation could also occur without a trauma mechanism due to glenoid fossa dysplasia. Despite ethical and religious positions of patient about blood transfusions, open Bristow-Latarjet procedure may be performed with recovery of good upper extremity function (constant score and DASH score), low of recurrence and good clinical outcomes.
Conclusion
Atraumatic bilateral neglected anterior shoulder dislocation can be treated with an open Bristow-Latarjet procedure to provide a stable glenohumeral joint in laborer patient. This open surgical procedure is reliable, secure and burdened with fewer complications over time, especially even in special cases (Jehovah’s witness) to create a greater extension of the glenoid arc and to avoid future dislocation.
Clinical Message
Though very rare, atraumatic bilateral neglected anterior shoulder dislocation does occur and may present to orthopedic evaluation. It should be accurately diagnosed and studied and its treatment depends on many factors.
Reference
1. O’connor-Read L, Bloch B, Brownlow H. A missed orthopaedic injury following a seizure: A case report. J Med Case Rep 2007;1:20.
2. Lasanianos N, Mouzopoulos G. An undiagnosed bilateral anterior shoulder dislocation after a seizure: A case report. Cases J 2008;1(1):342.
3. Balesteros R, Benavente P, Bonsfills N, Chacón M, García-Lazáro FJ. Bilateral anterior dislocation of the shoulder: Review of seventy cases and proposal of a new etiological-mechanical classification. J Emerg Med 2013;44(1):2669-2679.
4. Schulz TJ, Jacobs B, Patterson RL Jr. Unrecognized dislocations of the shoulder. J Trauma 1969;9:1009-1023.
5. Brown RJ. Bilateral dislocation of the shoulders. Injury 1984;15:267-273.
6. Solomon L, Warwick D, Nayagam S, editors. Injuries of the shoulder, upper arm and elbow. In: Apleys System of Orthopaedics and Fractures. London: Arnold; 2001. p. 587-589.
7. Iannotti JP, Williams GR. Patologie Della Spalla. Diagnosi e trattamento. 2nd ed. Philadelphia, Roma: Lippincott Williams and Wilkins, Verduci; 2009.
8. Gerber C. Chronic, locked, anterior and posterior dislocations. In: Warner JP, Iannotti JP, Flatow EL, editors. Complex and Revision Problems in Shoulder Surgery. 2nd ed. Philadelphia: Lippincott Williams and Wilkins; 2005. p. 89-103.
9. Longo UG, Loppini M, Rizzello G, Ciuffreda M, Maffulli N, Denaro V. Latarjet, Bristow, and Eden-Hybinette procedures for anterior shoulder dislocation: Systematic review and quantitative synthesis of the literature. Arthroscopy 2014;30(9):1184-1211.
10. Abdelhady AM. Neglected anterior shoulder dislocation: Open remplissage of the Hill-Sachs lesion with the infraspinatus tendon. Acta Orthop Belg 2010;76(2):162-165.
11. Gavriilidis I, Magosch P, Lichtenberg S, Habermeyer P, Kircher J. Chronic locked posterior shoulder dislocation with severe head involvement. Int Orthop 2010;34(1):79-84.
| How to Cite This Article: Poggetti A, Castellini I, Neri E, Marchetti S, Lisanti M. Atraumatic Bilateral Neglected Anterior Shoulder Dislocation: Case Report of a Jehovah’s Witness 28-Year-Old Male Affected by Iron-Deficiency Anemia and Treated with Bilateral Latarjet Procedure. Journal of Orthopaedic Case Reports 2015 July – Sep;5(3): 81-83 . Available from: https://www.jocr.co.in/wp/2015/07/01/2250-0685-317-fulltext/ |

[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


