
[box type=”bio”] What to Learn from this Article?[/box]
The study of clinical results in the treatment of articular calcaneum fractures should be done considering only the long-term clinical outcomes in order to choose the treatment..
Case Report | Volume 5 | Issue 3 | JOCR July-Sep 2015 | Page 57-59 | Fulvio Carluzzo, G.F. Longo. DOI: 10.13107/jocr.2250-0685.293.309
Authors: Fulvio Carluzzo[1], G.F. Longo[1]
[1] Department of Orthopaedics; Trauma center of Emergency Hospital “Cannizzaro”, Catania Italy.
Address of Correspondence
Dr. Fulvio Carluzzo,
S. Quasimodo street n 2, 95126 Catania, Italy.
E mail – carluzzofulvio@tiscali.it
Abstract
Introduction: The following is an original case report in the literature of a patient with post-traumatic bilateral calcaneum fracture, both type III of Sanders’ classification, that was treated, by the same surgeon, in the left foot with open reduction and internal fixation and in the right foot with closed reduction and application of an external fixator.
Case Report: Patient 43 y.o., male, high fall accident, with bilateral calcaneum fracture, both type III of Sanders’ classification. we have chosen to treat the left foot with ORIF (Fig. 3) and the right one with closed reduction and application of an external fixator. Patient was followed up radiologically with radiographs at 2, 12 and 24 months, and clinically at15 days, 1, 3, 6, 12, 18 and 24 months with the Maryland Foot Score, as suggested by Sanders et al.
Conclusion: In our patient, the one year clinical outcomes post-surgery was better in the foot treated with external fixation, regardless complex fracture and the not good status of soft tissue , due to open surgical treatment and hardwere inside. Long-term clinical follow-up given best outcomes in patients treated with ORIF, due to better reduction of subtalar joint facet and Böhler’s angle.
Keywords: articular calcaneum fractures, external fixator, plate and screws.
Introduction
The following is an original case report in the literature of a patient with post-traumatic bilateral calcaneum fracture, both type III of Sanders’ classification, that was treated, by the same surgeon, in the left foot with open reduction and internal fixation and in the right foot with closed reduction and application of an external fixator.
Case report
Patient 43 y.o., male, high fall accident, with bilateral calcaneum fracture, both type III of Sanders’ classification. (Fig. 1-2). Both legs were posed in anti declivous position and checked every day for two weeks. After this period the right foot showed a compromised conditions of the soft tissues with the presence of blisters but the left foot showed a recurrence of skin folds.  For this reason we have chosen to treat the left foot with ORIF (Fig. 3) and the right one with closed reduction and application of an external fixator (Fig. 4). Post-operatively, weight-bearing was not permitted for eight weeks for both legs. The fixator was removed after 10 weeks (Fig. 5-6).
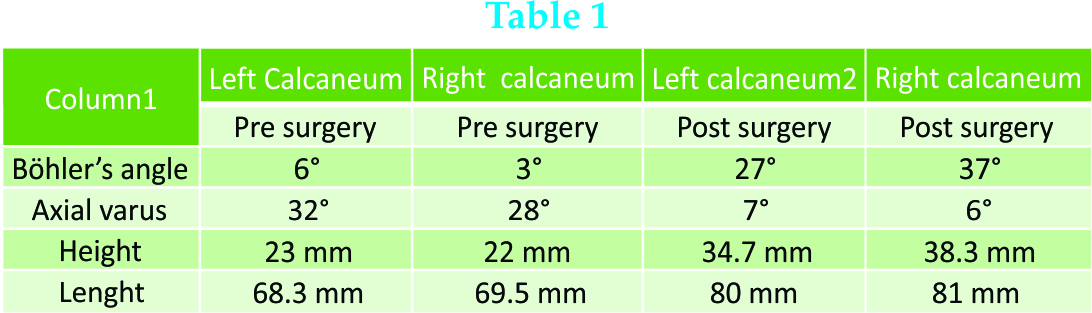
For this reason we have chosen to treat the left foot with ORIF (Fig. 3) and the right one with closed reduction and application of an external fixator (Fig. 4). Post-operatively, weight-bearing was not permitted for eight weeks for both legs. The fixator was removed after 10 weeks (Fig. 5-6).  Patient was followed up radiologically with radiographs at 2, 12 and 24 months, and clinically at15 days, 1, 3, 6, 12, 18 and 24 months with the Maryland Foot Score, as suggested by Sanders et al. [1]. In our case report we obteined a good reduction of the fractures with both surgical techniques with a restoration of physiological angles of both calcaneum. Böhler’s angle before surgery was 6° in the left one and 3° in the right side, after surgery it was 27° in the left foot and 37° right one. The axial varus angle before surgery in the left calcaneum was 32° and in the right calcaneum was 28°, afther surgery it was 7° in the left calcaneum and 6° in the right one. The height before surgery in the left one was 23 mm and in the right one was 22 mm, after surgery it was 34.7 mm in the left calcaneum and 38,3 in the right one. The lenght before surgery in the left one was 68.3 mm and in the right one was 69.5 mm, after surgery it was 80 mm in the left calcaneum and 81 in the right one (Tab 1). The clinical outcomes showed, until one year’s follow-up, better clinical results in the foot treated with external fixator, (Maryland Foot Score 83 p), then in the foot treated with ORIF (Maryland Foot Score72 p.) (Fig. 7-8-9).
Patient was followed up radiologically with radiographs at 2, 12 and 24 months, and clinically at15 days, 1, 3, 6, 12, 18 and 24 months with the Maryland Foot Score, as suggested by Sanders et al. [1]. In our case report we obteined a good reduction of the fractures with both surgical techniques with a restoration of physiological angles of both calcaneum. Böhler’s angle before surgery was 6° in the left one and 3° in the right side, after surgery it was 27° in the left foot and 37° right one. The axial varus angle before surgery in the left calcaneum was 32° and in the right calcaneum was 28°, afther surgery it was 7° in the left calcaneum and 6° in the right one. The height before surgery in the left one was 23 mm and in the right one was 22 mm, after surgery it was 34.7 mm in the left calcaneum and 38,3 in the right one. The lenght before surgery in the left one was 68.3 mm and in the right one was 69.5 mm, after surgery it was 80 mm in the left calcaneum and 81 in the right one (Tab 1). The clinical outcomes showed, until one year’s follow-up, better clinical results in the foot treated with external fixator, (Maryland Foot Score 83 p), then in the foot treated with ORIF (Maryland Foot Score72 p.) (Fig. 7-8-9). After one year the outcomes resulted good (Maryland Foot Score 87 p.) in the foot treated with ORIF and fair (Maryland Foot Score 69 p.) in foot treated with external fixation.
After one year the outcomes resulted good (Maryland Foot Score 87 p.) in the foot treated with ORIF and fair (Maryland Foot Score 69 p.) in foot treated with external fixation.
Discussion
Calcaneum fractures involving the joints are disabling injuries which can jeopardise work and day-to-day activities. Such injuries represent more than 2% of all fractures, and 65% to 70% of them have displacement of the articular surfaces [2]. Despite several comparative studies the optimal management of intra-articular calcaneal fractures is controversial. [3]. There are a number of reasons for this; 1) difficulty in obtaining reduction using conservative methods, often leading to pain, hind-foot deformity, impingement and disturbed gait; 2) difficulty of reduction and fixation, even with an open surgical approach; 3) the high risk of major complications related to open surgery: up to a 16% incidence of wound complications and a 20% incidence of infection in closed fractures, increasing to 33% in open injuries. The risk of nerve injury is 1.6% . The main goal of treatment for displaced fractures of the calcaneum should be the restoration of the three-dimensional structure, with emphasis on correct alignment in the coronal and axial planes and the height of the calcaneum body, [4-5] rather than anatomical reconstruction of the congruency of the subtalar articular fragments . [6] Open reduction and stable internal fixation is usually advocated for intra-articular fractures with relevant joint displacement (>1 mm), and in extra-articular fractures compromising the soft tissues, it should allow early motion to restore function. External fixation with closed or percutaneous reduction, following a pre-operative CT scan, is a minimally-invasive technique that can obtain reduction and stable fixation of most displaced articular fractures while greatly reducing the risks of open surgery. The clinical results appear to be comparable to those observed following open reduction and internal fixation [7]. Anatomical restoration of the subtalar joint facet is very difficult to achieve, particularly with percutaneous reduction and external fixation using two single pins to stabilise the articular fragments. Some degree of stiffness and degenerative arthritis of the subtalar joint following a displaced articular fracture is usually unavoidable whatever the chosen treatment [8] owing to severe damage to the articular cartilage which almost always sustains high-energy axial load [9]. Neither the subtalar mobility nor the clinical outcome seem to be significantly affected by obtaining congruency of the subtalar facet when compared with the results reported with open forms of treatment which specifically aim to reduce the articular fragments anatomically, but correlate more with the results following early post-operative mobilization and the restoration of Böhler’s angle, according to Paul et al.
Conclusion
In our patient, the one year clinical outcomes post-surgery was better in the foot treated with external fixation, regardless complex fracture and the not good status of soft tissue , due to open surgical treatment and hardwere inside. Long-term clinical follow-up given best outcomes in patients treated with ORIF, due to better reduction of subtalar joint facet and Böhler’s angle.
Clinical Message
The author recommends to reserve external fixation, for treatment of articular calcaneum fractures, in patients where the serious condition of the soft tissue contraindicate the use of ORIF for the high risk of complications.
Reference
1. Sanders R, Fortin P, DiPasquale T, Walling A. Operative treatment in 120 displaced intraarticular calcaneal fractures: results using a prognostic computed tomography scan classification. Clin Orthop 1993;290:87–95.
2. Sanders R, Hansen ST Jr, McReynolds IS. Trauma to the calcaneus and its tendon: fractures of the calcaneous. In: Jahss MH, ed. Disorders of the foot and ankle. Second ed. Philadelphia etc: W. B. Saunders Co., 1991:2326–54.
3. Randle JA, Kreder HJ, Stephen D, et al. Should calcaneal fractures be treated surgically?: a meta-analysis. Clin Orthop 2000;377:217–27.
4. Eastwood DM, Langkamer VG, Atkins RM. Intra-articular fractures of the calcaneum. Part II: open reduction and internal fixation by the extended lateral transcalcaneal approach. J Bone Joint Surg [Br] 1993;75-B:189–95.
5. Paul M, Peter R, Hoffmeyer P. Fractures of the calcaneum: a review of 70 patients. J Bone Joint Surg [Br] 2004;86-B:1142–5.
6. Nogarin L, Magnan B, Bragantini A, et al. Trattamento a cielo chiuso degli affossamenti talamici con mini-fissatori esterni. In: Mori F, Gianni S, Traina GC, Massari L, eds. Fratture del calcagno. Progressi in Medicina e Chirurgia del Piede. Vol 3. Bologna: Aulo Gaggi Editore 1994:153–9.
7. Sanders R, Fortin P, DiPasquale T, Walling A. Operative treatment in 120 displaced intraarticular calcaneal fractures: results using a prognostic computed tomography scan classification. Clin Orthop 1993;290:87–95.
8. Sanders R. Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg [Am] 2000;82-A:225–50.
9. Borelli J Jr, Torzilli P, Grigiene R, Helfet DL. Effect of impact load on articular cartilage: development of an intra-articular fracture model. J Orthop Trauma 1997;11:319–26.
10. Paul M, Peter R, Hoffmeyer P. Fractures of the calcaneum: a review of 70 patients. J Bone Joint Surg [Br] 2004;86-B:1142–5.
| How to Cite This Article: Carluzzo f, Longo GF . External Fixation Vs Orif in the Treatment of Bilateral Calcaneum Fracture . Journal of Orthopaedic Case Reports 2015 July – Sep;5(3): 57-59 . Available from: https://www.jocr.co.in/wp/2015/07/10/2250-0685-309-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


