
[box type=”bio”] What to Learn from this Article?[/box]
In spite of some inherent weakness this publication will add to popularize one disease process (BPOP) which is believed to be rare. I consider this is not the situation. Possibly this is because of the ignorance by most of the clinician and pathologist too. Paucity of mention in text books makes the PG students unaware about the condition in D/D of osteochondroma.
Case Report | Volume 5 | Issue 4 | JOCR Oct-Dec 2015 | Page 3-6 | Jitendra Nath Pal, Maitreyee Kar, Sunit Hazra, Anindya Basu. DOI: 10.13107/jocr.2250-0685.331 .
Authors: Jitendra Nath Pal[1], Maitreyee Kar[2], Sunit Hazra[3], Anindya Basu[3].
[1] Department of Orthopaedics, Murshidabad Medical College, Station Road, Berhampore, District – Murshidabad, Pin – 742101. India.
[2] Department of Anatomy, North Bengal Medical College, Sushrutnagar, District – Darjeeling. India.
[3] Department of Orthopaedics, R G Kar Medical College, 1, Khudiram Sarani, Kolkata – 700004. India.
Address of Correspondence
Dr. Jitendra Nath Pal,
F – 505, Maitri apartment, 255, N S C Bose Road, Kolkata – 700047. India. E mail – jitendranathpal@gmail.com
Abstract
Introduction: Solitary exostosis is common at the metaphysis of long bones, and rarely may it develop in the lower pole of the patella. Usually it stops growing after skeletal maturity unless complicated. When the growth continues after skeletal maturity, other rare possibilities need to be considered such as bizarre parosteal osteochondromatous proliferation (BPOP). Though solitary exostosis is common at the metaphysis of long bones, very rarely it also develops in lower pole of the patella. Usually they stop growing after skeletal maturity unless complicated. When it starts after skeletal maturity and continues to grow, other rare possibilities like bizarre parosteal osteochondromatousp roliferation (BPOP) are to be thought of.
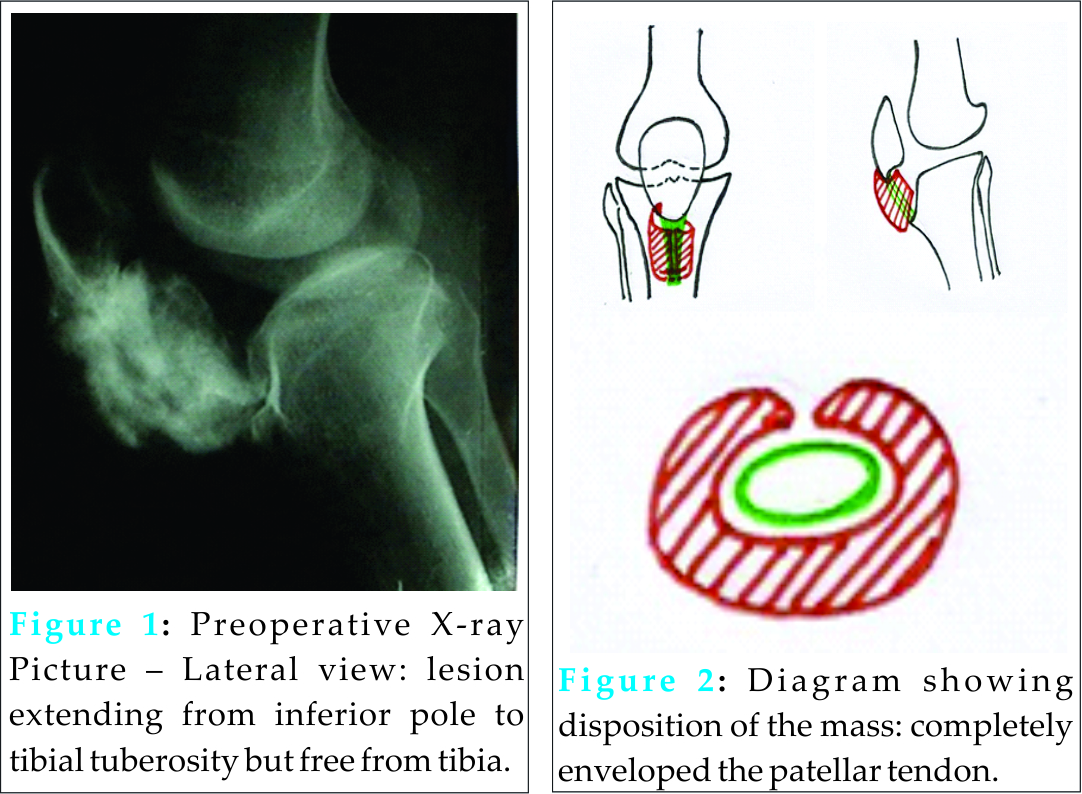
Case Report: 21 years male student presented with anterior midline painless progressive swelling over right knee joint of one year duration which was hard, non-tender, fixed to patella but mobile with patella. X ray showed midline heterogeneously radio-opaque swelling attached to inferolateral aspect of the anterior surface of patella. Patellar out line is fully maintained except the narrow site of tumour attachment. After exposing through midline incision, the swelling was found to incorporate the patellar tendon completely and an anterior vertical midline cleavage was found. The mass was deliberately detached along the cleavage and from intact patellar tendon. Almost full range of knee movement is obtained in operation table. Immediate post operative 10° quadriceps lag was corrected with quadriceps setting exercises in two weeks time. Histopathological examination demonstrated thin layer of cartilage cover, irregular lamellar bone in deeper zone and spindle cells between them without cytoplasmic atypia. Plenty of cartilage cells in different stages of maturation are seen without column formation. Marrow elements are absent. Periosteum could not be demonstrated and there was no other evidence of malignancy. Features simulate ‘bizarre parosteal osteochondromatous proliferation’. There is no recurrence in five years of follow up.
Conclusion: When exostosis like lesions arise from unusual site and at an unusual age group, other rare conditions need to be investigated. Though the final diagnosis of BPOP is obtained after careful histo-pathological examination, the clinico-radiological findings are also relevant. As literature search indicates, this is possibly second incidence where BPOP arised from sesamoid bone and first from patella.
Keywords: Patella; Bizarre parostealosteochondromatous proliferation; BPOP; Osteochondroma.
Introduction
Exostosis is a common benign tumour resulting from growth aberration particularly in metaphyseal region of long bones. Infrequently it arisesfrom short and flat bones like scapula, clavicle, pelvis, rib, carpals and metacarpals, metatarsals etc [1]. Very rarely it arises from patella in its lower pole [1 to 7]. Usually it stops growing with skeletal maturity unless complicated with srcomatous change. Hereditary multiple exostosis (HME) are a result of mutation of EXT gene which results in low pericellular production of heparan sulphate (HS) or it’s over metabolism thus preventing normal maturation of growth plate [9,10]. Bizarre parostealosteochondromatous proliferation (BPOP) is a rare condition that usually involves metacarpals and metatarsals, though one incidence of involvement of sesamoid bone of foot has been found in literature [8]. This case is being reported because of its rarity, evidence of continued growth even after skeletal maturity and its extent to envelopment of the adjacent patellar tendon. Differencial diagnosisis also discussed. Decision making whether to sacrifice the patellar tendon is also an issue.
Case report
21 years male student presented at a rural tertiary care centre in March 2004 with anterior midline progressive swelling over right knee joint of one year duration. It started with a small hard nodule near inferior pole of right patella just lateral to the midline without any pain or constitutional symptom. During one year it progressed to the level of tibial tuberosity. It was attached to the patella but remained free from tibial tuberosity. Patellar tendon could not be palpated separately. Side to side movement of the swelling along with the patella was possible. 50% flexion was restricted where as rotations retained to its fuller extent. It was not associated with trauma.
X- ray showed midline heterogeneously radio-opaque swelling attached to inferolateral aspect of surface of patella. Patellar out line is fully maintained except the narrow site of tumour attachment. No evidence of cortical erosion, periosteal reaction or elevation. Cleavage between patella and swelling is well appreciated in the under surface [Fig 1].
Incision biopsy was planned.
Through longitudinal midline incision, the mass was exposed and found a small site of attachment to the anterolateral aspect of the lower pole of patella. The patellar tendon could not be identified, as it was completely wrapped by the swelling with an anterior vertical midline cleavage [Fig 2]. Initially it was planned to excise the mass along with patellar tendon and its reconstruction. Before doing so one half of the mass was deliberately detached along the cleavage when the patellar tendon could be visible. So the entire mass was excised without damaging patellar tendon. The mass was not adherent to the tendon. It was little attenuated but integrity of the tendon was found satisfactory. Almost full range of movement could be obtained on operating table. Wound was then closed in layers leaving a closed suction drain which was removed after 48 hours.
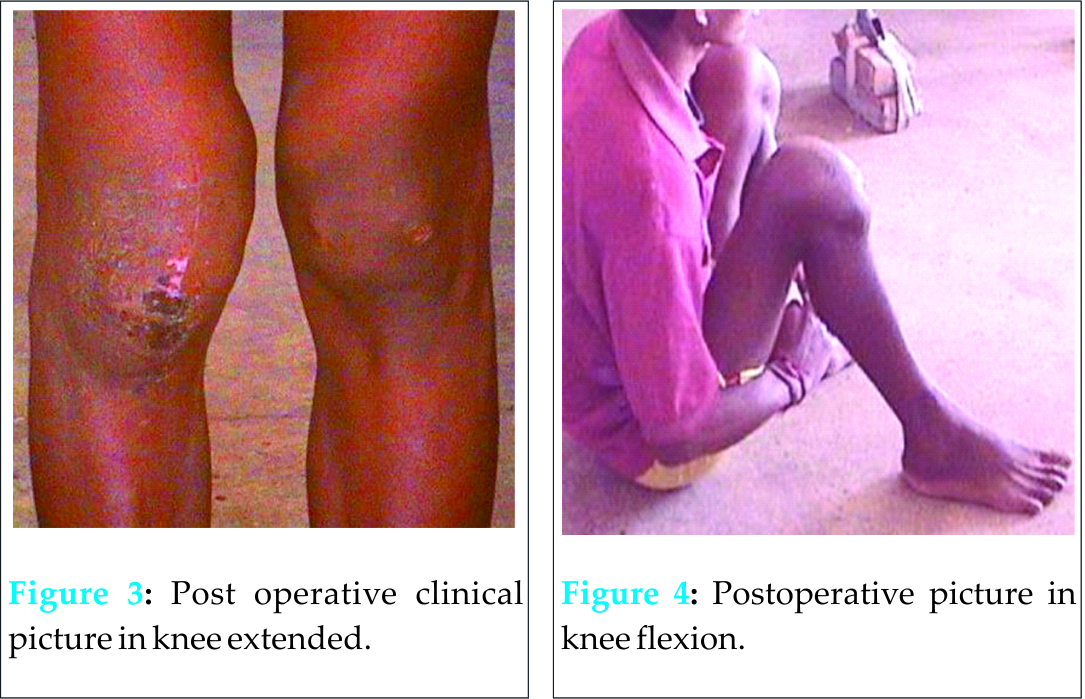
Quadriceps exercise started on second post operative day. Normal activities were permitted after 2 weeks when stitches were removed. [Figs 3, 4] Patient was followed up at two weeks, 6 weeks and subsequently at 6 month intervals upto 5 years. Post operative, immediate 10° quadriceps lag was corrected in two weeks time. There has been no evidence of recurrence till date.
Macroscopically, the mass was covered with a thin layer of capsule and the lobulated surfacewas covered with thin layer of cartilage. Tumour tissue is friable and heterogeneous.
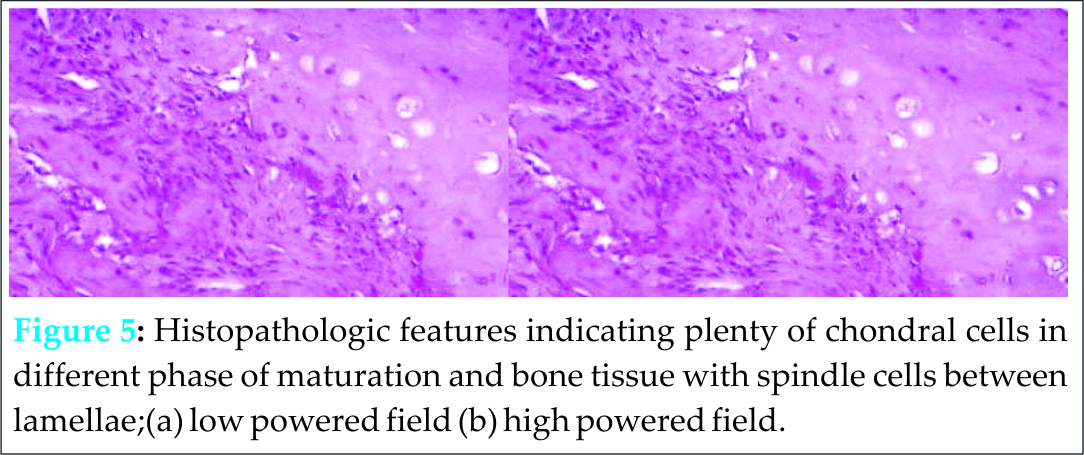
Histopathological examination demonstrated thin layer of cartilage cover,irregular lamellar bone in deeper zone and spindle cells between them without cytoplasmic atypia. Plenty of cartilage cells are seen without columnformation. Marrow elements are absent. Periosteumcould not be demonstrated and there was no evidence of malignancy.
Discussion
Solitary exostosis in patella, as reported in literature, is very rare. Singh J et al (2009) [1] reported 26 neoplastic patellar lesions without any incidence of exostosis after a database study of four tumour registries.Orava, Osterback, and Hurme (1986) [2] reported two cases in relation to patellar tendon lesions and one by Enriquez, Quiles and Torres (1981) [3]. However few more cases are reported in literatures other than English [4 to 7].
They were believed to stop growth with skeletal maturity. But recently mutation of tumour gene is also correlated with solitary exostosis and the traditional theory of ‘skeletal dysplasia’ is shifting towards the theory of ‘cell-of-origin’ [9 and 10]. This might be the explanation of continued growth of solitary exostosisafter skeletal maturity in some cases. Other features in the present case do not support the diagnosis of exostosis.
Dysplasia epiphysealishemimelia (DEH) [4, 11], BPOP [12 to 16], Turret exostosis[17] and florid reactive periostitis [18] are considered as other possibilities in relation to this case.
DEH, alsoknown as Trevor-Fairbank disease is an epiphyseal developmental malformation of skeleton resulting in exophytic, tumour-likelesion in early childhood with male preponderance. Predilectedsites are epiphyses of weight bearing long bones and tarsus of one side of body. Localised, classic and generalized forms are identified. Commonly startsfrom medial secondary centre of ossification. Such lesion from patella is also reported in literature [4, 11]. Basic pathology reported is isabnormal cartilage proliferation and enchondral ossification from secondary centre of ossification. Differentiating features are presence of cartilaginous bands betweenareas of cancellous bone. Tumour gene is not yet demonstrated [4]. Age of the patient, location,non-expansion of parent bone and histologicfeatures are not correlating with the present case.
BPOP, also known as Nora’s lesion, is proliferation of bone in relation to intact cortical surface of short and rarely in long bones [12]. It simulates with reactive heterotrophic ossification. Genetic mutation is recently suggested [13]. BPOP apparently arises from the periosteal tissues through a process of cartilaginous metaplasia[14].
3rd or 4th decade is identified as the usual age group for BPOP. Cortical continuity may not be present in early stages but it ultimately develops with the progression of the disease. Sex dominance is not reported in literature. Plain radiology in most occasions resembles exostosis. CT scan and MRI could help in demonstrating space between tumour and cortex in certain stages of the disease and also heterogeneous character of the mass itself. Inherent weakness of the article is non application of these modalities due to nonavailability at that stage.But per-operative and macroscopic observations could demonstrate them.Microscopically, it is composed of hyper cellular cartilage with basophilic tinctorial character with evidence of calcification and ossification.. Trabecularbone maturesin deeper zones. The presence of spindle cellin the inter-trabecular space creates confusion with parosteal osteosarcoma and myositis ossificance traumatic.But in this case they are without hyperchromtosia and cytologicalatypia. Thinning of cartilage layers are usual and more so in long standing cases[12 to16].These features are observed in the present case. 50% local recurrence is reported in literature [13]. But this patient did not have recurrence in 5years.
BPOP, Turret exostosis and florid reactive periostitisare belied to represent different stages of a posttraumatic proliferative process [17]. Turret exostosis is a benign osteo-cartilagenous lesion.By the influence of mild trauma reactive periosteumis believed to produce such tumour like mass [17]., Central area of mature bone from endochondral ossification with thin hypocellular peripheral rim of cartilage and absence of periosteum are microscopic features. No history of trauma can be obtained in this case.
Osteochondroma or BPOP in unusual site may represent focal lesion of heterotrophic ossificansatraumatica and diffuse idiopathic skeletal hyperostosis (DISH) also known as Forestier’s disease [19, 20]. Since there is no multifocal involvement they are excluded.
The disposition of mass resulted in incorporation of the tendon fully within the mass leaving an anterior longitudinal cleavage. Mass including tendon excision can be confidently avoided if preoperative biopsy and MRI studies are done. In this case same thing has been done on clinical basis only.
Conclusion
Exostosis like lesions when arising from unusual site and at unusual age group other rare conditions is to be thought of. Though the final diagnosis of BPOP is obtained after careful histo-pathological examination, the clinic-radiological findings are also suggestive. As evident from literature search this is possibly second incidence where BPOP arising from sesamoid bone and first for patella.
Clinical Message
Managing such a lesion one should go for pre-operative biopsy and MRI study to avoid sacrifice of patellar tendon where reconstruction is difficult and morbidity is high.
References
1. Singh J, James SL, Kroon HM, Woertler K, Anderson SE, Jundt G, Davies AM.Tumour and tumour-like lesions of the patella–a multicentre experience.EurRadiol. 2009; 19(3):701-12.
2. Orava S, OsterbackL,Hurme M. Surgical treatment of patellar tendon pain in athletes. Brit.J.Sports Med. 1986;20(4):167-169.
3. EnriquezJ, Quiles M, Torres C. A unique case of dysplasia epiphysealishemimelica of the patella.ClinOrthopRelat Res1981;160:168–171.
4. Araujo CR Jr, Montandon S, Montandon C, Teixeira KISS, Moraes FB , MoreiraMAR.DysplasiaEpiphysealisHemimelica of the Patella.Radiographics March-April 2013; 33.
5. MaurerHJ. Symmetrical osteocartilaginousexostoses (osteochondroma) of the patella.FortschrGebRontgenstr Nuklearmed1963;98:771–772.
6. LouisR, Pouye I, Conty RC, Quenum C, Ouiminga RM. Voluminous osteochondroma of the knee cap: patellectomy. Bull Soc Med Afr Noire Lang Fr1968;13(3):722–729.
7. SadykhovAG. Osteochondroma of the patella. OrtopTravmatol Protez1962;23:77–78.
8. Berber O, Dawson-Bowling S, Jalgaonkar A, Miles J, Pollock R C, Skinner J A, Aston W J S, Briggs T W R. Bizarre parostealosteochondromatous proliferation of bone: clinical management of a series of 22 cases. J Bone Joint Surg Br. 2011 Aug ;93 (8):1118-21.
9. Szuhai K, Yavas A, Knijnenburg J, van Duin M, van Dikken H, Tarminieu AH, Cleton-Jansen AM,Bovee JV, Hoqendoom PC. The role of EXT1 in nonhereditary osteochondroma: identification of homozygous deletions. L J Natl Cancer Inst. 2007;99(5):396-406.
10. Porter DE, Simpson AH. The neoplastic pathogenesis of solitary and multiple
osteochondromas. J Pathol1999;188(2):119-25.
11. Timm C, Immenkamp M, Roessner A. On the Clinical Picture of Dysplasia EpiphysealisHemimelica. Z OrthopIhre Grenzgeb.1986;124(2):148-56.
12. Adler D, AignerT, von Salis-Soglio G, Gutberlet M, Heyde CE. Nora’slesion. Discussion of a rare bone proliferation. Orthopade. 2010;39(11):1065-70.
13. Kraft D, Hailer NP. [Nora’slesion at the second metacarpal bone of a twelve-year-old female].Z OrthopIhreGrenzgeb 2006;144(2):228-31.
14. AbramoviciL,Steiner GC. Bizarre parostealosteochondromatous proliferation (Nora’slesion): a retrospective study of 12 cases, 2 arising in long bones. Hum Pathol 2002;33(12):1205-10.
15. García-Alvarez F, Laclériga AF, Bueno AL, Castiella T, Seral F. Bizarre parostealosteochondromatous proliferation. Difficulty in diagnosis. ChirOrganiMov 1999;84(2):179-82.
16. Meneses MF, Unni KK, Swee RG. Bizarre parostealosteochondromatous proliferation of bone (Nora’slesion).Am J SurgPathol. 1993;17(7):691-7.
17. LeClere LE, Riccio AI, Helmers SW, Thompson KE. Turret exostosis of the talus.Orthopedics. 2010 Jul 13;33(7):517.
18. Mnif, Zrig, Jawahdou, Sahnoun, Koubaa, Abid. An unusual localisation of osteochondroma. A single case report. Chir Main 2009; 28(4):247-9.
19. Pollock JM; Brogdon BG; Simonds J; Boudreaux C; Nimityongskul P; Massi DS Multifocal variant of heterotopic ossification. Br J Radiol. 2008; 81(963):e88-92.
20. Resnick, Shaul, Robins . Diffuse idiopathic skeletal hyperostosis (DISH): Forestier’s disease with extraspinal manifestations. Hum Pathol. 2007;38(8):1265-72. Epub 2007.
| How to Cite This Article: Pal JN, Kar M, Hazra S, Basu A. Differential diagnosis of BPOP arising in relation to patella. Journal of Orthopaedic Case Reports 2015 Oct-Dec;5(4): 3-6. Available from: https://www.jocr.co.in/wp/2015/10/01/2250-0685-331-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]


