
[box type=”bio”] What to Learn from this Article?[/box]
After closed reduction of elbow dislocation and above elbow slab application in simple dislocation , diligent vascular examination of limb need to be done ,in patients who has pain and swelling around elbow in spite of good peripheral pulses ,can some times surprise like in this case with transected brachial artery if not careful in evaluating.
Case Report | Volume 5 | Issue 4 | JOCR Oct-Dec 2015 | Page 27-29 | JayanthKumar B C, Deepak Sampath, Hanumantha Reddy N, Vishnu Motukuru. DOI: 10.13107/jocr.2250-0685.338 .
Authors: JayanthKumar B C[1], Deepak Sampath[1], Hanumantha Reddy N[1], Vishnu Motukuru[1]
[1] Department of Orthopaedic surgery, St.Martha’s Hospital, Bangalore. India.
Address of Correspondence
Dr. Jayanth Kumar B C,
Department of Orthopaedic surgery, St.Martha’s Hospital, # 1,Nrupathunga road, Bangalore 560001. India.
E mail – jkbcortho@gmail.com.
Abstract
Introduction: Vascular injury associated with closed posterior elbow dislocations is rare and it usually occurs along with open dislocation, anterior dislocation, penetrating injuries, dislocations associated with fracture. We report such a case of We report such a case of closed posterior elbow dislocation with complete brachial artery rupture.
Case Report: A 58 year old lady sustained a posterior dislocation of right elbow following a fall at home. She presented three days later with complaints of severe pain, swelling around the right elbow and numbness of fingers following a closed reduction done elsewhere. Compute Tomography Computed tomography–angiography showed complete transection of brachial artery. Patient was treated with thrombectomy, right great saphenous vein interposition repair of brachial artery and forearm fasciotomy.
Conclusion: Posterior dislocation of elbow with vascular injury, though a rare condition, early diagnosis and treatment of the vascular injury is the key to prevent compartment syndrome and Volkmann ischemic contracture and to regain a normal upper limb function. Vascular injuries associated with posterior elbow dislocation are very rare, but high index of suspicion of arterial injury need to be thought off and repeated vascular examination during pre and post reduction stage should be done to prevent complications.
Keywords: Posterior elbow dislocation; brachial artery transection; compartment syndrome.
Introduction
Elbow dislocation is the most frequently encountered presentation after shoulder dislocation [1]. The most common mechanism of injury is fall on outstretched hand that forces elbow into hyperextension. Types of elbow dislocations are anterior, posterior, postero-medial, postero-lateral, lateral, medial and divergent. Vascular injury associated with elbow dislocations are rare [2], and it usually occurs along with open dislocation, anterior dislocation, penetrating injuries, dislocations associated with fracture [3]. Vascular injury is usually evident from ischemic clinical picture that includes absence of distal pulses, pale hand, cold extremity and diminished sensation. However, sometimes complete brachial artery transection can be present with well per-fused limb, palpable radial artery and normal capillary refilling time because of rich collateral circulation around the elbow [4,5].
We report a case of patient who was referred to our Hospital three days after closed reduction of posterior right elbow dislocation. The approach to diagnosis and management of arterial injury in this case is presented here.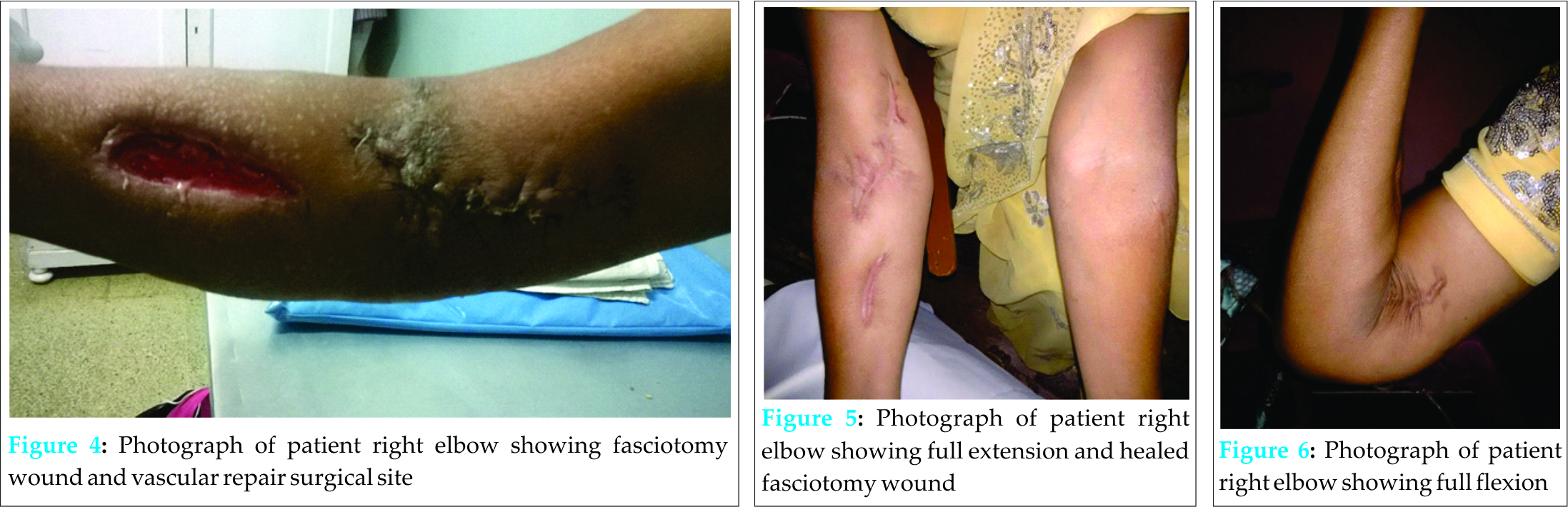
Case Report
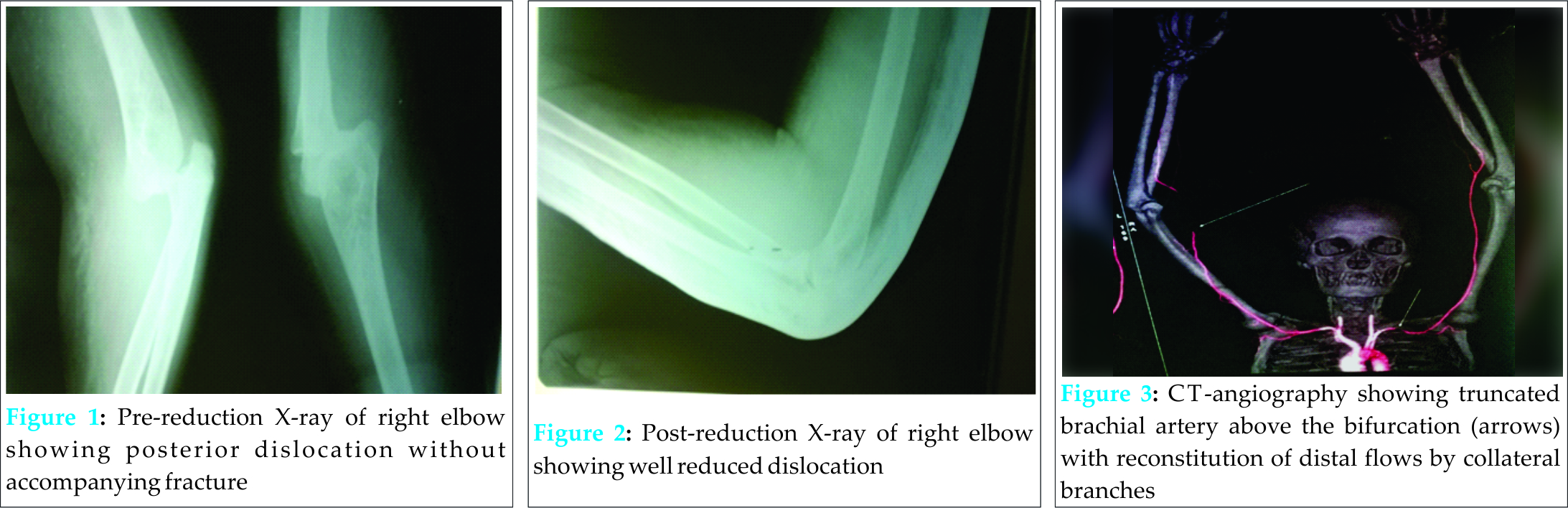
A 58 year old lady sustained posterior dislocation of right elbow following a fall at home. She underwent closed reduction of the dislocation elsewhere, and above elbow slab application (Fig 1,2). She was referred to our hospital three days later with complaints of severe pain, swelling around the right elbow and numbness of fingers. As per the treatment notes there was no obvious neuro vascular injury and radial artery pulse was felt immediately after reduction of elbow dislocation. On examination we noted that the elbow was swollen, there were superficial blebs, forearm was tense, and there was mild stretch pain. Vascular examination showed good capillary refill with palpable radial artery pulse and decreased sensation over fingers. We evaluated the patient using X-ray of the right elbow -which showed well reduced dislocation and no evidence of fracture. To rule out any vascular injury, Arterial Doppler scan was performed which showed -large hematoma causing extrinsic compression over distal end of brachial artery with minimal monophasic flow in distal arteries.
We took the patient for brachial artery exploration to clear-the hematoma under general anesthesia. A two cm vertical incision was made over medial aspect of lower arm and hematoma was removed. We were surprised to note a pulsating tubular structure with occluding lumen occluded lumen, which led to our suspicion of a complete brachial artery rupture. Immediately, the patient was referred to a vascular surgeon for CT-angiography and for further management. CT angiography showed, complete right brachial artery transection five cm above the elbow with thrombus in both ends and significant blood flow in distal arteries through collateral circulation (Fig 3). The patient was further treated with excision of injured segment of vessel and right trans brachial proximal and distal thrombectomy. The artery was reconstructed by interposition repair of right great saphenous vein graft and forearm fasciotomy (Fig 4) in anticipation of compartment syndrome and reperfusion injury. The elbow was immobilized in above elbow slab. Patient was administered with antibiotics, analgesics and anticoagulants as a post-surgical procedure. Sutures were removed on 15th post-operative day; and skin grafting was done for fasciotomy wound after three weeks. Three weeks after immobilization, the patient was advised with elbow range of motion exercises.
Discussion
Closed posterior elbow dislocation is a common condition. Vascular injury is very rare in a closed dislocation without accompanying fracture. Clinically these cases present as acute limb ischemia/weak radial pulse on affected side. Occasionally such cases may present late with well per fused limb with palpable radial artery and normal capillary filling time [6]. Early recognition of brachial artery rupture in cases with elbow dislocation is very important, since it may lead to potentially devastating complications such as limb loss and Volkmann’s ischaemic contracture. In the case presented here, we encountered a complete rupture of brachial artery; however, distal circulation was still maintained by rich collateral circulation around elbow. Perry et al reported that significant arterial injury exist without a detectable change in distal pulses or evidence of ischemia in 10% of the proven arterial injuries [7]. Due to rarity of this complication and the variable clinical presentation, the presence of distal pulse is not enough proof of an intact artery; rather early diagnosis depends on high index of suspension [8].
In recent times CT- angiography is more commonly used to evaluate the vascular injury. Typical angiographic findings include long segment of abruptly occluded flow usually about 5-6 cm above the elbow. Active contrast extravasation may not be present due to intraluminal thrombi. Duplex USG has been shown to be accurate for detecting significant vascular injuries. In addition, duplex USG can differentiate arterial transection from entrapment or thrombosis by detecting gap between two transected ends [9]. Different options available to treat vascular injury include repair with saphenous vein graft, synthetic vein graft, and brachial artery ligation.
Conclusion
The rich peri-articular collateral circulation can mask the findings of acute arterial injury, which may lead to delay in diagnosis. The case presented here emphasizes the need for repeated vascular examination during pre- and post- reduction stage. There is a high index of suspicion of vascular injury, and to look for signs of ischemia, proper reduction of dislocation and the need for short hospital stay in closed reduction of elbow dislocation to prevent complications. We recommend to review all cases after 24 hrs for pain, swelling, blebs, numbness, in spite of good capillary refill. In case any of these symptoms are present, subject the patient for duplex scan or CT angiography at earliest.
Clinical Message
Brachial artery transection following closed elbow dislocation although rare should have high index of suspicion of arterial injury; and repeated vascular examination should be done to prevent complications.
References
1. Khun MA, Ross G.Acute elbow dislocations. Ortho Clin North Am 2008; 39:155-61
2. Endean ED, Veldenz HC, Schwarcz TH, Hyde GL.Recognition of arterial injury in elbow dislocation. J. VascSurg 1992;16:402-6.
3. Marcheix B, Chaufour X, Ayel J, Hollington L, MansatP, Barret A, et al. Transection of the brachial artery afterclosed posterior elbow dislocation. J VascSurg2005;42:1230-2.
4. Ayel JE, Bonnevialle N, Lafosse JM, Pidhorz L, AlHomsy M, Mansat P, et al. Acute elbow dislocationwith arterial rupture:analysis of nine cases. Ortho.TraumatolSurg Res2009;95:343-51.
5. Carter SJ, Germann CA, Dacus AA, Sweeney TW,Perron AD. Orthopedic pitfalls in the ED:neurovascular injury associated with posterior elbow dislocations. Am J Emerg Med2010;28:960-5.
6. Eijer H, Ballmer FT, Ris HB, Hertel R. Delayeddiagnosis of a ruptured brachial artery after posteriordislocation of the elbow. Injury 1998;29:390-2.
7. Perry MO,Thal ER, Shires GT. Managementof arterialinjuries. Ann Surg 1971173:403-8.
8. Eijer H, Ballmer FT, Ris HB, Hertel R. Delayed diagnosis of aruptured brachial artery after posterior dislocation of the elbow.Injury.1998;29:390-2.
9 Johansen J, Lynch K, Paun M, Copass M. Non-invasive vascular tests reliably exclude occult arterial trauma in injured extremities. J Trauma. 1991;31:515-22.
10.YunusNazli,NeccmettinColak,Ismail Uras,MahmutKomurcu,and Omar Cakir.brachial artery transaction associated with open elbow dislocation in a 12 year old: a case report vascular 2013; 21:27-30.
| How to Cite This Article: JayanthKumar BC, Sampath D, Reddy NH, Motukuru V. Complete Brachial Artery Transection following closed Posterior Elbow Dislocation: A Rare Case Report. Journal of Orthopaedic Case Reports 2015 Oct-Dec;5(4): 27-29. Available from: https://www.jocr.co.in/wp/2015/10/01/2250-0685-338-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


