
[box type=”bio”] What to Learn from this Article?[/box]
The idea of presenting this case is to convey the message to the young surgeons that each case of hip fracture dislocation is different and rarest among rare patterns are possible.
Case Report | Volume 5 | Issue 4 | JOCR Oct-Dec 2015 | Page 34-35 | Jawahar Adi Raja, Brijesh P Valsalan. DOI: 10.13107/jocr.2250-0685.340 .
Authors: Jawahar Adi Raja[1] Brijesh P Valsalan[2]
[1] Department of Orthopaedics, Malabar Medical College, Calicut, Kerala, India.
[2] Department of Orthopaedics, Co-operative Hospital, Vatakara, Calicut, Kerala, India..
Address of Correspondence
Dr. Jawahar Adi Raja
21/217 H ‘Meadows’ Nut Street, Vatakara, Calicut, Kerala, India.
E-mail:orthojar@gmail.com
Abstract
Introduction: Anterior dislocation of hip associated with fracture of proximal femur is an uncommon injury. Only very few cases are reported in the literature. We report such an unusual and previously not described case of anterior dislocation of hip associated with fracture of trochanter and neck of the femur in an elderly lady.
Case Report: A 60 year old lady was presented to our casualty following a fall at home. She complained of pain in the left hip with deformity and inability to move the limb. The hip was externally rotated and clinical examination revealed anterior dislocation of the hip. X-ray showed associated fracture of the proximal femur extending between base of greater trochanter and head of the femur. Cemented Hemiarthroplasty was done under regional anesthesia.
Conclusion: Anterior dislocation of hip with extensive fracture of proximal femur, though a rare condition may present because of associated twisting force at the time of the fall. If operated with cemented prosthetic replacement of the head, patient can be mobilized early.
Keywords: Anterior dislocation hip; Fracture dislocation hip; Trochanteric fracture
Introduction
Dislocation of hip is not uncommon especially in road traffic accidents where because of direction of injury (as in dash board injury) and severity of impact, dislocation is often associated with fractures of various patterns [1]. Posterior dislocation of hip associated with fracture of the head of the femur or acetabulum are well known [1, 2]. However dislocation of the hip with fracture of the neck or shaft of the femur is very rare and only a few cases have been described [3].
The combination of anterior dislocation of hip with associated ipsilateral fracture trochanter and neck without any fracture of head of femur is very rare and has not been reported in the literature till date. However posterior dislocation of the hip with above mentioned fracture pattern is reported previously [1].
Case Report
A 60 year old lady was brought to our hospital casualty in March 2013 after a fall. She gave history of a sudden twist while climbing stairs following which she fell down. On examination she was conscious and oriented; but unable to move her left lower limb which was rotated externally and about 4 centimeter shorter. Left pubic region showed fullness with palpable rounded bony mass and more prominent femoral artery pulsation. Radiograph (Fig.1) showed dislocation of hip with fracture of trochanter extending through neck of femur to the base of the head. There was no fracture in any other bones of the limb. Neurovascular structures were clinically intact. Patient was immediately worked up for surgery and she underwent cemented hemiarthroplasty using Thompson Prosthesis. Posterior approach was opted to prevent neurovascular injury from distorted anterior anatomy and also because surgeons were more familiar with that approach. Fracture line was found extending from greater trochanter laterally passing obliquely and proximally to end at the base of the head of the femur. Greater trochanter was found avulsed as a separate fragment. At the end of six months patient had painless hip with near normal range of movements and an acceptable gait.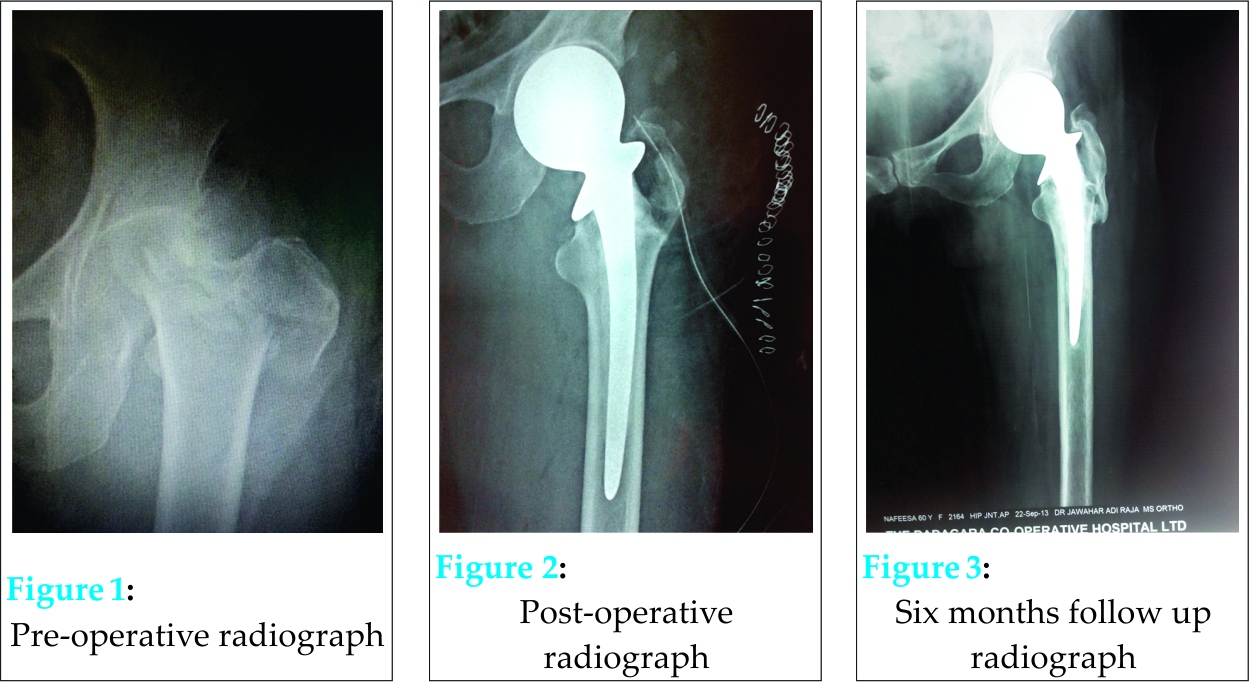
Discussion
Dislocation of hip usually occurs as a result of high energy trauma and is often associated with injury to head of femur or acetabulum [4]. An additional acetabular fracture occurs if longitudinal forces are stronger than adduction forces. But if longitudinal force is combined with adduction force, neck of femur gets fractured especially in osteoporotic bone [5]. Our patient might have been subjected to considerable rotational force which caused this very rare pattern of injury. We believe that first mechanism was longitudinal force which was then supervened by adduction and external rotation force leading to anterior dislocation of hip and associated fracture of neck and trochanter of the femur. Such injuries are orthopedic emergencies and require immediate surgical intervention [5].Up to 1/3 of these cases can lead to osteonecrosis of the head of the femur especially if associated with severe bone destruction as in our case [2]. As there was comminution of trochanter and the entire neck was involved by the fracture pattern, open reduction was not attempted. Head of the femur along with attached part of the neck was removed. Remnant neck was nibbled out and cemented hemiarthroplasty performed (Fig.2). The avulsed greater trochanter fragment which got fallen back by itself after reduction of the hip was stabilized with thick (No.1) absorbable sutures of Monofilament Polydioxide (PDS) material. Walker assisted mobilization was started on 5th post-operative day;non-weight bearing for three weeks and then gradually increasing partial weight bearing walking. At six months follow up after surgery, the radiograph (Fig.3) of the operated hip showed near normal joint anatomy and good functional outcome.
Conclusion
The pattern of injury described above do not fit into present classification systems described for hip fracture dislocation injuries. We recommend that classification system be reviewed to include such rare patterns of injury too. The mechanism of injury of our case could be longitudinal force with adduction to start with followed by external rotation of the limb. The only treatment option left with for such injuries are hemiarthroplasty followed by early non-weight bearing mobilization.
Clinical Message
Though rare, anterior dislocation of hip with associated fracture of trochanter and neck of the femur may present to casualty. Such cases should be managed on emergency basis.
References
- Esenkaya I, Gorgec M. Dislocation of the hip and ipsilateral femoral neck fracture. Sicot Case-Reports:February 2002
- Alexa O, Puha B, Veliceasa B, Paduraru D. Posterior dislocation of the hip associated with ipsilateral trochanteric fracture-a very rare case. Romanian Society of Surgery Magazine Chirurgia;104(6):761-764.
- Reggiori A, Brugo G. Traumatic anterior hip dislocation associated with anterior and inferior iliac spines avulsions and a capsular-labral tear. Strategies Trauma Limb Reconstr. April 2008;3(1):39-43
- Radulescu R, Badila A, Japie I, Papuc A and Manolescu R. Anterior dislocation of the hip associated with intertrochanteric fracture of the femur-Case presentation Med Life Sep 15 2013;6(3):336-339.
- Agarval R, Rai AK, Saraf SK, Singh S, Singh A. An unusual pattern of Posterior Dislocation of Hip associated with Comminuted Trochanteric Fracture. The internet Journal of Orthopedic Surgery 2008;Volume 9:Number 1.
- Dawson A.B, Van Rijn B.Traumatic Anterior Dislocation of the Hip. Arch Orthop Trauma Surg 1989;108:55-57.
- 7. Chadda M, Agarwal A, Singh A. Traumatic anterior dislocation of the hip joint with posterior acetabular wall fracture. ActaOrthop.Belg. 2005;71:111-114
| How to Cite This Article: Raja JA, Valsalan BP. A Case of Anterior Dislocation of Hip Associated with an Unusual Pattern of Fracture of Proximal Femur. Journal of Orthopaedic Case Reports 2015 Oct-Dec;5(4): 34-35. Available from: https://www.jocr.co.in/wp/2015/10/01/2250-0685-340-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


