
[box type=”bio”] What to Learn from this Article?[/box]
Rotating Hinge Knee arthroplasty with prophylactic gastrocnemius flap can be a bail out option in a neglected post-traumatic infective arthritis of knee with limb malalignment, contracted extensor apparatus and significant bone loss.
Case Report | Volume 5 | Issue 4 | JOCR Oct-Dec 2015 | Page 40-43 | Sanjeev Patnaik, Biswaranjan Nayak, Laxmikanta Mishra, Akshaya Kumar Sahoo. DOI: 10.13107/jocr.2250-0685.342 .
Authors: Sanjeev Patnaik[1], Biswaranjan Nayak[2], Laxmikanta Mishra[1], Akshaya Kumar Sahoo[3]
[1] Department of Orthopaedics, Apollo Hospital, Unit-15, Bhubaneswar, Odisha, India.
[2] Department of Neurosurgery, Apollo Hospital, Bhubaneswar, Odisha, India .
[3] Department of Plastic Surgery , Apollo Hospital, Bhubaneswar, Odisha, India.
Address of Correspondence
Dr. Sanjeev Patnaik ,
Senior Consultant Orthopaedics, Apollo Hospital, Bhubaneswar, Odisha, India PIN- 751005.
E mail – sportho1973@yahoo.co.in
Abstract
Introduction: Prophylactic gastrocnemius flap with primary rotating hinge knee is technically demanding in a case of neglected post-traumatic, infective arthritis of the knee, with challenges of compromised skin and soft tissues, articular bone defect, limb mal-alignment, gross instability, retained hardware and a contracted extensor mechanism with the patella fixed in the lateral gutter all in combination, is rarely reported. We report such a complex case in this study.
Case Report: We report a 48 years male patient with a history of fracture lateral femoral condyle of right knee due to road traffic accident 10 years back , for which he got operated with open reduction and internal fixation with cancellous screws, which subsequently got infected. Primary procedure undertaken was removal of implants, debridement, placement of antibiotic-cement spacer followed by prophylactic medial gastrocnemius flap and a temporary joint spanning external fixator. Definitive procedure undertaken, after clearance of infection in 12 weeks was conversion to a rotating hinge TKR using a lateral para-patellar arthrotomy & tibial tubercle osteotomy to address the challenges of fixed patella in the lateral gutter and contracted ligamentum patellae. At one year follow up, the knee was painless, stable, with satisfactory range of motion and improved function without any infection or aseptic lysis.
Conclusion: Prophylactic Gastrocnemius flap cover along with rotating hinge knee arthroplasty using a lateral para-patellar approach and tibial tubercle osteotomy in a case of neglected post-traumatic , infective arthritis of knee with the complexities of limb mal-alignment, compromised skin and soft tissue, articular bone loss and ligamentous instability is a satisfactory bail out option in such a highly complex joint scenario.
Keywords: Post-Traumatic Arthritis Knee, Rotating-Hinge Knee, Gastrocnemius flap, Primarytotal knee replacement
Introduction
Primary total knee arthroplasty is a well-established procedure, with a proven track record over decades now, for the treatment of advanced arthritis of the knee. It presents a high level of satisfaction and survivorship around 95% in 15 years [1]. The indications of TKA are now extending to new frontiers as a salvage procedure in catastrophic, complex long-standing deformities of the knee with super-added infection. Prophylactic Gastrocnemius flap cover prior to TKA is an excellent option in such compromised skin and soft tissue scenario. Rotating Hinge Knee TKA is a bail out when collateral ligamentous stability is questionable along with significant articular bone loss.
Case report
We report a 48 year male patient with a history of fracture lateral femoral condyle of right knee due to road traffic accident 10 years back, for which he had been operated with open reduction and internal fixation with cancellous screws, which subsequently got infected. He had repeated trauma to the limb two years post surgery and this time was treated conservatively in a plaster cast. For last eight years he had a downward spiral in knee function . On presentation to our clinic one year back, he had pain in the right knee, inability to bear weight and varus deformity along with discharging sinus (Fig-1a). He was barely able to take a few steps without support and had constant pain. On examination, the knee was swollen with mild effusion, skin was adherent to the bone with puckering, 20 degrees of varus deformity, gross medio-lateral instability and patella was fixed in the lateral gutter. The distal neuro vascular status was intact. On radiographic examination, the knee was postero-laterally sub-luxated (Fig1 b,c). CT angiography was done to chalk out the course of the popliteal vessels (Fig-1d,e).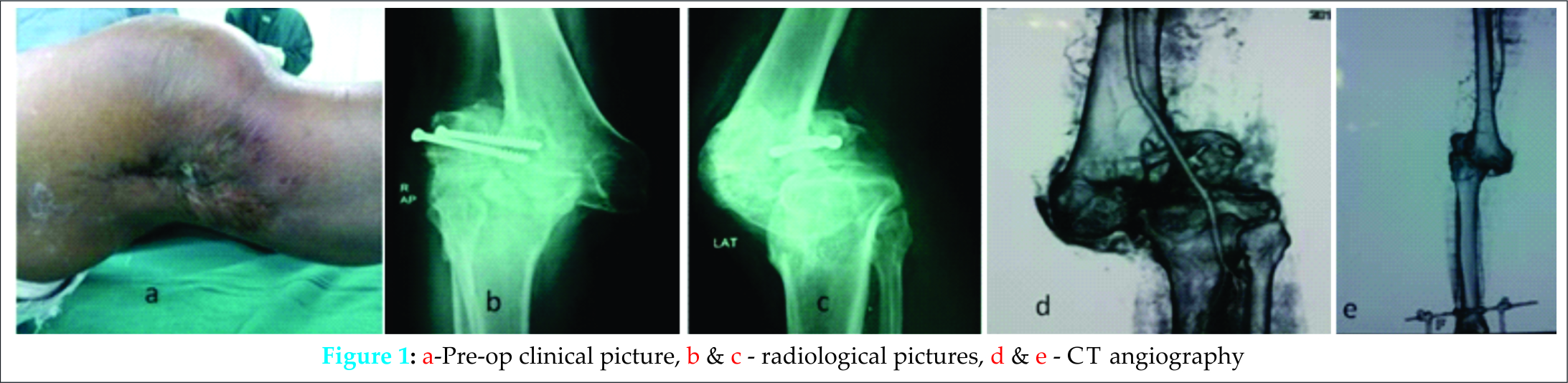 Initially he was on distal tibial skeletal traction to address the mal-alignment but to no avail. Then we planned for a multi staged surgery after proper haematological workup along with culture from the wound site. In the first stage, implants were removed along with debridement of the infected granulation tissue, necrotic lateral femoral condyle was removed , antibiotic cement spacer was given, adherent and puckered skin was excised followed by medial Gastrocnemius myocutaneous flap and a temporary joint spanning external fixator was given (Fig-2a,b) . The patient received four weeks of IV antibiotics and regular wound dressing which led to complete healing of the soft tissues along with normalization of the infection markers (Fig-2c,d).
Initially he was on distal tibial skeletal traction to address the mal-alignment but to no avail. Then we planned for a multi staged surgery after proper haematological workup along with culture from the wound site. In the first stage, implants were removed along with debridement of the infected granulation tissue, necrotic lateral femoral condyle was removed , antibiotic cement spacer was given, adherent and puckered skin was excised followed by medial Gastrocnemius myocutaneous flap and a temporary joint spanning external fixator was given (Fig-2a,b) . The patient received four weeks of IV antibiotics and regular wound dressing which led to complete healing of the soft tissues along with normalization of the infection markers (Fig-2c,d).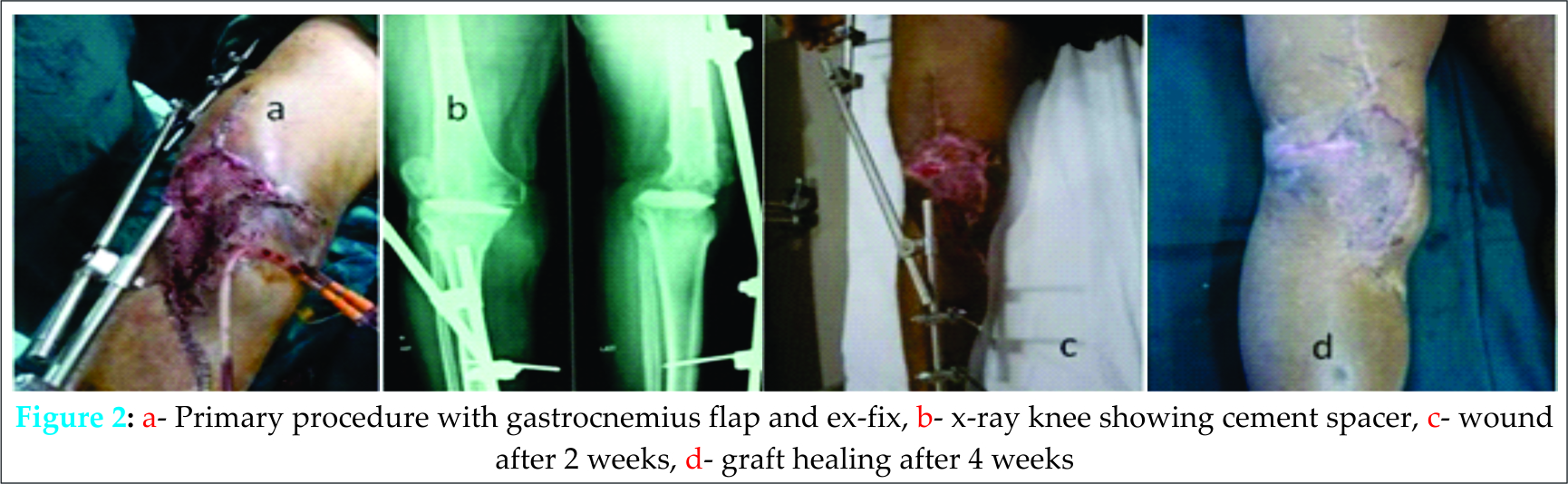 The external fixator was removed at four weeks and knee immobilizer was given along with static quadriceps exercises for four weeks. Eight weeks after the primary procedure, he was planned for total knee replacement using rotating hinge knee (NexGen®RH Knee-Zimmer), with metal wedge augments for lateral femoral condyle. Mid line skin incision of the previous surgery was used. To address the fixed patella in the lateral gutter and the contracted extensor apparatus, a lateral para patellar approach along with tibial tubercle osteotomy was done. The cement spacer was removed, knee joint was debrided of cement and granulation tissue and thoroughly lavaged. Rotating hinge knee (NexGen®RH Knee-Zimmer) was implanted with Palacos cement. Osteotomized tibial tubercle was reattached with two cancellous screws. Wound closure was done over closed suction drains (Fig-3),
The external fixator was removed at four weeks and knee immobilizer was given along with static quadriceps exercises for four weeks. Eight weeks after the primary procedure, he was planned for total knee replacement using rotating hinge knee (NexGen®RH Knee-Zimmer), with metal wedge augments for lateral femoral condyle. Mid line skin incision of the previous surgery was used. To address the fixed patella in the lateral gutter and the contracted extensor apparatus, a lateral para patellar approach along with tibial tubercle osteotomy was done. The cement spacer was removed, knee joint was debrided of cement and granulation tissue and thoroughly lavaged. Rotating hinge knee (NexGen®RH Knee-Zimmer) was implanted with Palacos cement. Osteotomized tibial tubercle was reattached with two cancellous screws. Wound closure was done over closed suction drains (Fig-3),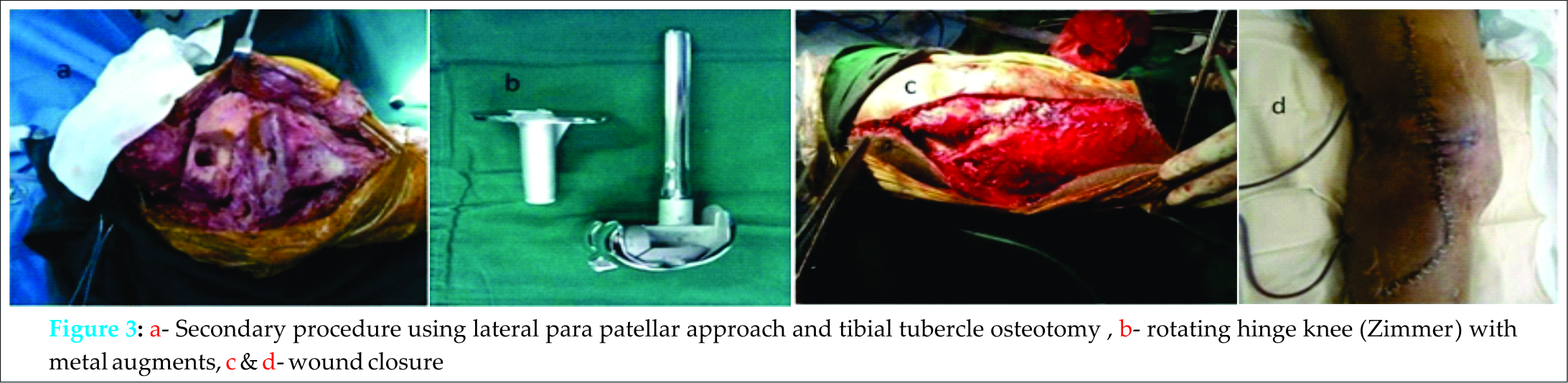 and compression dressing was given. Post operative radiographs shows good alignment (Fig- 4a, b).
and compression dressing was given. Post operative radiographs shows good alignment (Fig- 4a, b).
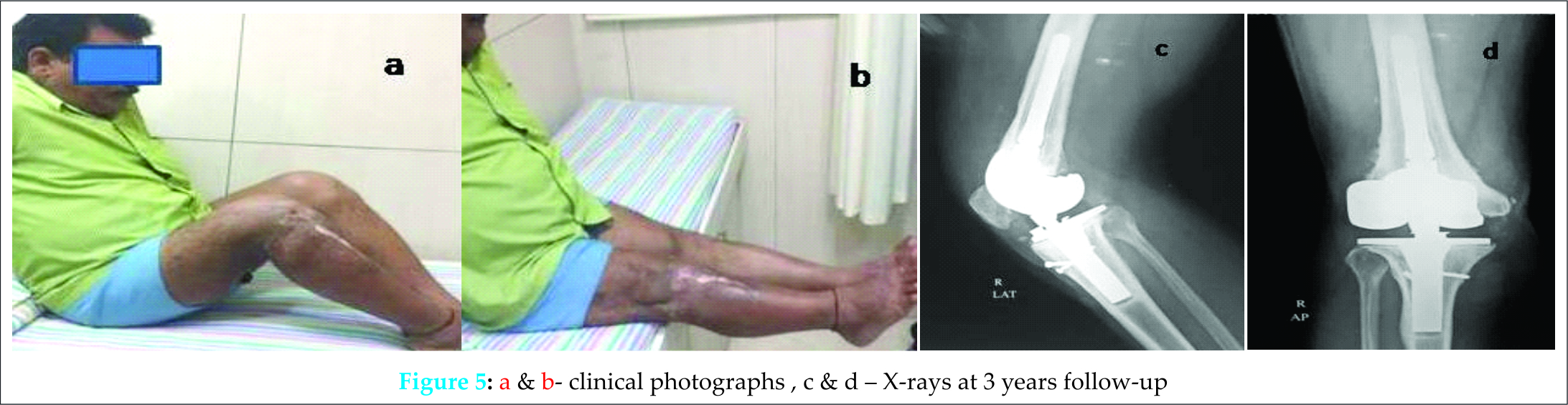
The knee was placed in an immobiliser for six weeks. Static quadriceps exercises were encouraged, toe touch weight bearing was allowed after two weeks, knee bending was restricted to 20-30 degrees for six weeks, active extension exercise was delayed for six weeks to allow healing of osteotomy site. Graded knee bending exercises along with full weight bearing was started after six weeks. The patient was followed up regularly and at the end of one year his wound was completely healed, knee was painless and stable (Fig-4c, d).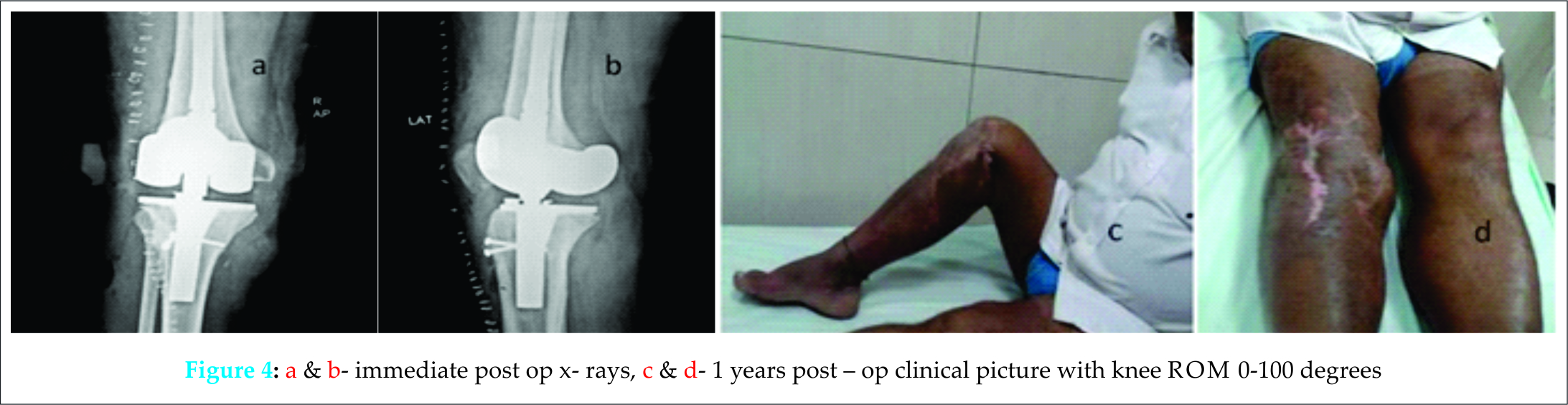 The pre-operative Knee Society Scores for pain and function were 30 and 40 points respectively, and improved significantly post-operatively to 80 (pain) and 76 (Function) points respectively at latest follow up of 3 years. The knee ROM significantly improved from Pre-op 30 degree flexion to 100 degree flexion. There was no evidence of infection or aseptic lysis (Fig-5).
The pre-operative Knee Society Scores for pain and function were 30 and 40 points respectively, and improved significantly post-operatively to 80 (pain) and 76 (Function) points respectively at latest follow up of 3 years. The knee ROM significantly improved from Pre-op 30 degree flexion to 100 degree flexion. There was no evidence of infection or aseptic lysis (Fig-5).
Discussion
Total knee arthroplasty in patients with preoperative periarticular soft-tissue defects along with bony mal-alignment can result in suboptimal results and ominous complications. Meticulous preoperative evaluation and planning of soft tissue coverage,liaisoning with plastic surgeon helps to prevent skin sloughing and necrosis, which can ultimately lead to exposed knee implant and the need for additional intervention. As expected, the results from salvage soft-tissue protocols are mixed. Risk of infection is substantially higher once implant has been placed, and the results are often poor with regard to functional rehabilitation and recovery [2,3].
To override these perceived complications, some surgeons have tried prophylactic treatment of such soft-tissue defects. Tissue expanders have been used to stretch the soft tissue to increase their coverage prior to total knee arthroplasty, but this has an increased risk of infection. Simultaneous flap coverage in the setting of total knee arthroplasty has also been reported with fair results. There are sporadic reports on prophylactic soft-tissue coverage in a staged fashion several months prior to total knee arthroplasty [4].
The local soft-tissue environment dictates the choice of coverage. The gold standard for coverage about the knee is the gastrocnemius flap which has excellent results, especially in a setting of infection and hence we selected this flap. Free flaps may be considered in situations where local tissue is inadequate. Free-flap options for the lower extremity include the rectus abdominis muscle, latissimusdorsi muscle, anterolateral thigh, and deep inferior epigastric perforator (DIEP), among others [4,5,6].
In order to address the patella fixed in the lateral gutter and the externally rotated tibia, a lateral para-patellar approach was used in our case. The additional benefit of this approach is spontaneous correction of fixed external tibial rotational deformity and preservation of medial blood supply to the patella[7,8.]
As an extensile approach was anticipated, tibial tubercle osteotomy was performed in our case to prevent avulsion of ligamentum patellae due to the contracted extensor apparatus. It provides a safe and reliable means of extensile exposure of the knee and affords little tension on the extensor mechanism during eversion of the patella [9,10].
Due to the combined medio-lateral collateral ligament insufficiency and severe bone loss a constrained device- rotating hinge knee ( NexGen®RH Knee-Zimmer) was used. The indications for use of the Kinematic Rotating Hinged knee prosthesis includes severe bone loss combined with ligamentous instability, nonunion of a periprosthetic fracture, an acute periprosthetic fracture, severe collateral ligamentous instability, reimplantation for infection, nonunion of a supracondylar femoral fracture, congenital dislocation of the knee, and treatment of a severely comminuted distal femur [11]. The rotating hinge knee prosthesis provides locking stability in the heel strike and push-off phases of the gait cycle [12]. To address the lateral femoral condyle bone loss and to reconstruct a stable platform with transfer of load to the host bone, two modular metallic augments were incorporated in the femoral component of the rotating hinge knee. The other methods of reconstruction include the use of cement, custom-made tumour-type or hinged implants and bone grafting [13].
Conclusion
Prophylactic Gastrocnemius flap cover along with rotating hinge knee arthroplasty using a lateral para-patellar approach and tibial tubercle osteotomy in a case of neglected post-traumatic , infective arthritis of knee with the complexities of limb mal-alignment, compromised skin and soft tissue, articular bone loss and ligamentous instability is a satisfactory bail out option in such a highly complex joint scenario.
Clinical Message
Rotating hinge knee along with prophylactic gastrocnemius flap can be used as a bailout option in extremely complex primary TKR associated with neglected post-traumatic, infective arthritis of the knee, with challenges of, compromised skin and soft tissues, articular bone defect, limb mal-alignment and gross instability, but careful case selection is of paramount importance.
References
1. Ranawat CS, Flynn WF Jr, Deshmukh RG. Impact of modern technique on long-term results of total condylar knee arthroplasty. ClinOrthopRelat Res. 1994; 309:131–135
2. Casey WJ 3rd, Rebecca AM, Krochmal DJ, Kim HY, Hemminger BJ, Clarke HDet al. Prophylactic flap reconstruction of the knee prior to total knee arthroplasty in high-risk patients. AnnPlast Surg. 2011 Apr;66(4):381-7.
3. Papadopoulos EC, Parvizi J, Lai CH, LewallenDG. Total knee arthroplasty following prior distal femoral fracture. Show allKnee 2002 Dec;9(4):267-74.
4. Dane C. Hansen DO, Wong K, Moon MD. Sharat K, Kusuma MD,. Prophylactic Free Flap for Chronic Lower-Extremity Soft-Tissue Defect Prior to Total Knee Arthroplasty-A Case Report, JBJS Case Connect 2013; Jul 24;3(3):e75.
5. Jaureguito JW, Dubois CM, Smith SR, Gottlieb LJ, Finn HA . Medial Gastrocnemius Transposition Flap for the Treatment of Disruption of the Extensor Mechanism after Total Knee Arthroplasty. J Bone Joint Surg Am 1997 Jun;79(6):866-73.
6. Papp A, Kettunen J, Miettinen H. Pedicledgastrocnemius flapin complicated totalkneearthroplasty. Scandinavian Journal of Surgery 2003;92:156–159.
7. Frederick BF. A sequential three-step lateral release for correcting fixed valgus knee deformities during total knee arthroplasty. ClinOrthopRelat Res. 1990 Nov;(260):170-5.
8. Burki H, Von Knoch M, Heiss C, Drobny T, Munzinger U. Lateral approach with osteotomy of the tibial tubercle in primary total knee arthroplasty. ClinOrthopRelat Res. 1999 May;(362):156-61.
9. Whiteside LA, Ohl MD, Matthew D. Tibial tubercle osteotomy for exposure of the difficult total knee arthroplasty. ClinOrthopRelat Res. 1990 Nov;(260):6-9.
10. Chinzei N, Ishida K, Kuroda R, Matsumoto T, Kubo S, Iguchi T et al. Tibial Tubercle Osteotomy With Screw Fixation for Total Knee Arthroplasty . Orthopedics 2014 Apr;37(4):367-73.
11. Springer BD, Hanssen AD, Sim FH, Lewallen DG David G. The kinematic rotating hinge prosthesis for complex knee arthroplasty. ClinOrthopRelat Res. 2001 Nov;(392):283-91.
12. Hwang SC, Kong JY, Nam DC, Kim DH, Park HB, Jeong ST et al. Revision total knee arthroplasty with a cemented posterior stabilized, condylar constrained or fully constrained prosthesis: a minimum 2-year follow-up analysis. ClinOrthopSurg 2010 Jun;2(2):112-20.
13. Whittaker JP, Dharmarajan R, Toms AD. The management of bone loss in revision total knee replacement. J Bone Joint Surg Br. 2008 Aug;90(8):981-7.
| How to Cite This Article: Patnaik S, Nayak B, Mishra L, Sahoo AK. Complex Primary Total Knee Replacement (TKR) Using Prophylactic Gastrocnemius Flap and Rotating-Hinge Knee in Post-traumatic , Infective Arthritis of the Knee – A Case Report. Journal of Orthopaedic Case Reports 2015 Oct-Dec;5(4): 40-43. Available from: https://www.jocr.co.in/wp/2015/10/01/2250-0685-342-fulltext/ |

[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


