
[box type=”bio”] What to Learn from this Article?[/box]
The management procedure being a closed one has better healing, uses a good and cost effective implant resulting in early healing and no loss of reduction following implant removal.
Case Report | Volume 5 | Issue 4 | JOCR Oct-Dec 2015 | Page 64-67| Shivanand M Bandekar1, Mihir R Desai1. DOI: 10.13107/jocr.2250-0685.349 .
Authors: Shivanand M Bandekar[1], Mihir R Desai[1]
[1] Department of Orthopedic Surgery, Goa Medical College, Bambolim. India.
Address of Correspondence
Dr. Mihir R Desai,
Room number 229, GARD hostel, Opp. Goa. Medical College, Bambolim, Goa 403202. India.
E-mail : mihirrdesai@gmail.com
Abstract
Introduction: Injuries around the elbow are common in pediatric population. Amongst them, most common is fractures of the supracondylar part of humerus, followed by condylar fractures. Fractures of the neck of the radius account for five- ten percent of the total injuries.Various techniques for closed reduction of the fracture have been described in literature. Open reduction and fixation is indicated when closed reduction fails to provide satisfactory results and the angulation remains more than 45-60 degrees.
Case Report: We present two cases of severely displaced radial neck fractures treated with closed reduction and intramedullary fixation using titanium elastic nails.The distal bent tip of the nail is used to maneuver the proximal rotated fragment and to reduce it back in its place.
Conclusion: It is an indirect closed reduction technique and associated with minimal intra and post- operative complications and gives encouraging results. It gives stable fixation and also prevents re-displacement after nail removal.
Keywords: Radial neck fracture, closed techniques, titanium nail.
Introduction
Radial neck fractures in children are rare, representing five percent of all elbow pediatric fractures. Most are minimally displaced or nondisplaced [1].
In most series, the age of occurrence varies from four to 14 years of age, with the median age ranging from nine to ten years [2]. The anatomical complexity of the elbow and its blood supply makes treatment difficult [3].
Chambers combined the classifications of Jeffrey and Newman to produce a new classification based primarily on the mechanism of injury. According to this classification there are two types of injuries; valgus injuries and those associated with elbow dislocations. Most of these fractures are either Salter Harris type 2 or Salter Harris type 4 injuries [2].
O’Brien subdivided radial head and neck fractures into three categories based on the degree of angular displacement of the superior articular surface from the horizontal [4].

Various techniques for reduction have been described in literature [2] which includes:
Immobilization with no manipulation
Manipulative closed reduction
Percutaneous pin reduction
Intramedullary pin reduction.
Open reduction with or without internal fixation.
Excision of either the entire head or a small head fragment. Conservative treatment is unable to reduce severe displacements, resulting in malunion. Open reduction frequently leads to intraarticular calcification, avascular necrosis, and joint stiffness. In most cases, intramedullary nailing allows complete reduction without open joint and a very low complication rate. The pin is left in place, stabilizes the epiphysis, and prevents secondary displacement [5].
Retrospective studies in the past found that open reduction of radial neck fractures generally had poor results and that open reduction with internal fixation was even worse, as has been reported by others [6].
Both our cases were managed by intramedullary nailing with a slight modification of the technique with the use of a titanium elastic nail with its tip purposely made more curved.
Case report
We report two cases of radial neck fracture of which both are male patients of nine and 13 years respectively. Both presented to the emergency ward with acute trauma history with fall on outstretched hand with valgus impacted force with elbow in extension.There was tenderness and swelling around elbow. Both had no neurovascular deficits.
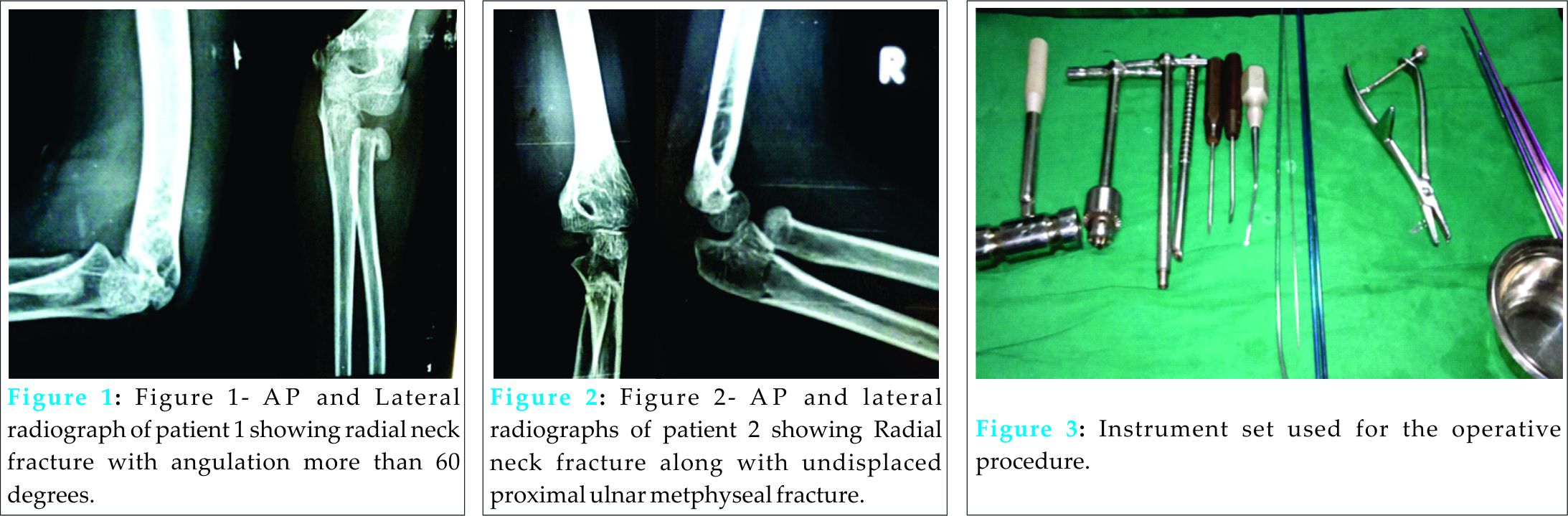
An Antero-posterior and lateral radiographs were taken. Radial neck fracture was diagnosed in one patient. Another patient had radial neck fracture along with proximal ulna undisplaced metaphyseal fracture.Fig 2- AP and lateral radiographs of patient 2 showing Radial neck fracture along with undisplaced proximal ulnar metphyseal fracture.
Fig 1- AP and Lateral radiograph of patient 1 showing radial neck fracture with angulation more than 60 degrees.
Both the patients were taken up for surgery under general anaesthesia. Supine position was given with careful draping of the corresponding limb so that elbow and wrist joints were kept free for closed manipulation of fracture fragment at the elbow and to introduce the titanium nail just proximal to distal radial physis.
A tourniquet was tied and kept in case the closed reduction and intramedullary nailing fails and in case open reduction had to be done.Fig 3- Instrument set used for the operative procedure.
2.5mm titanium elastic nail with its tip made more curved was introduced just proximal to distal radial physis under image intensifier.
Figs 4 and 5- showing entry point made in preepiphysial area of distal radial physis by an awl.
The nail was carefully advanced under image. When its tip reached the fracture site it was carefully rotated to engage the proximal fracture fragment. Simultaneous digital pressure was applied with thumb to enable engagement of the tip of the nail and the fracture fragment.
Once the tip got engaged with the proximal fragment it was gradually rotated back in its place and confirmed with the image intensifier.
Gradual traction and a varus force is also recommended during this procedure for better manipulation of the proximal fragment.The other end of the nail was bent and cut near the wrist joint for easy removal after eight- ten weeks.
Both the patients were regularly followed up for a period of six- eight months. Stitch removal near the entry point for the titanium nail was done after two weeks after confirming healthy wound status. An above elbow plaster slab immobilization was done immediately post-operatively up to a period of four weeks. After that gradual elbow mobilization was started at our institute only under supervision.
Up to 100-110 degrees of flexion was achieved in the first week with minimal extension lag which got corrected in the second week. By eight weeks full mobilization was achieved alongwith good range of pronation and supination.Figs 6 and 7- show full flexion and full extension without any lag in both the patients.
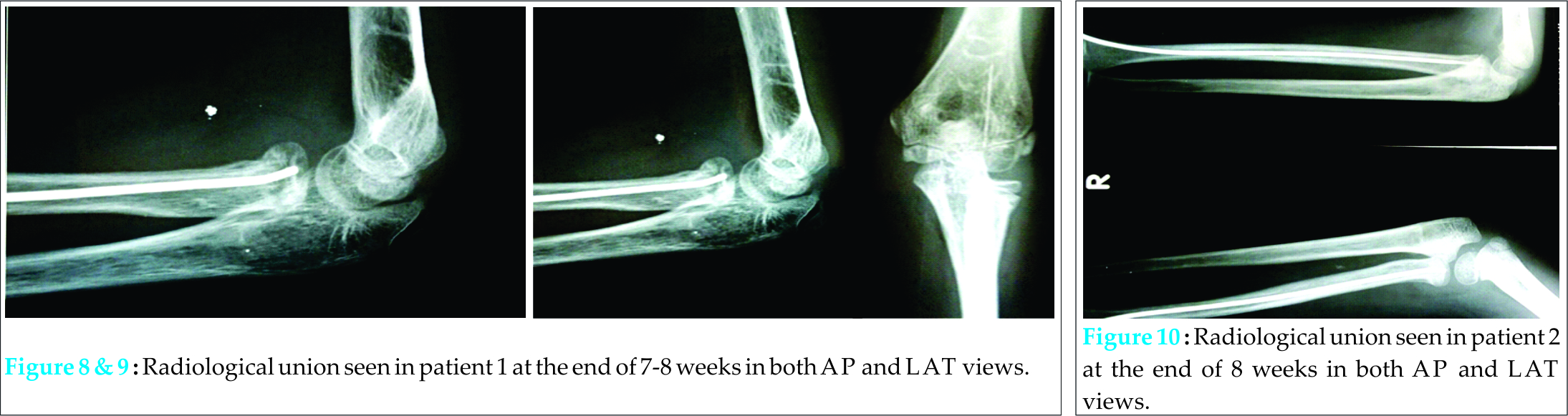
Radiological union was also achieved in the same time period and by 8-9weeks the intramedullary titanium nails were removed from both the patients.
Figs 8 and 9- Radiological union seen in patient 1 at the end of 7-8 weeks in both AP and LAT views.
Fig 10- Radiological union seen in patient 2 at the end of 8 weeks in both AP and LAT views.
Both the patients did not have any significant postoperative complications like posterior interroseous nerve injury, loss of reduction, infection or stiffness. The reduction was well maintained and fracture site well consolidated after nail removal.
Discussion
Fractures of the radial head or neck may occur as a result of two different mechanisms. Most commonly they result from a fall onto an outstretched hand with the elbow in extension and valgus [4].
The head of the radius and its blood supply can be damaged by the injury itself and by surgical manipulation such as in open reduction [3].
O’Brien subdivided radial head and neck fractures into three categories based on the degree of angular displacement of the superior articular surface from the horizontal [4]. This classification has proved to be most effective as a guide in both treatment and prognosis. In type I fractures the displacement is 30 degrees or less. Type II fractures have between 31 and 60 degrees of angulation. Type III fractures have more than 60 degrees of displacement [4].
In our cases both patients had type 3 fractures with angular displacement more than 60 degrees.The management of fractures of the neck of the radius in children is controversial [3]. There is little agreement as to what may be accepted as a satisfactory reduction. Minor degrees of angulation can be accepted and treated conservatively, but advice on the maximum acceptable angulation varies widely, up to as much as 45degrees [6].
Judet, Judet and Le Franc classified radial neck fractures into four types as follows:
Grade I: undisplaced fracture;
Grade II:< 30° (angulation of radial neck), S < 1/2 diameter of radial shaft (translation 1/1 diameter of radial shaft (translation >100%)
Grade III: = 30° to 60°, S 1/1 diameter of radial shaft (translation >100%)
Grade IV: = 60° to 90°, S>1/1 diameter of radial shaft (translation >100%).
Grade-I and grade-II fractures are treated by a cast with no reduction, grade-III by closed reduction and a cast, and grade-IV by CIMP, if necessary using percutaneous Kwires to aid reduction [3].
Fracture of the neck disrupts part of the periosteum with its vessels, more so in severely displaced fractures. Open reduction of the fracture can further damage the vascularity of the radial head. The high complication rate after open reduction and the poor functional results and inconvenience for the pediatric patients makes conservative treatment of radial neck fractures in children preferable. An attempt at closed reduction is recommended for fractures that are angulated more than 30 degrees. Closed reduction may fail in severely displaced fractures [7,8].
In 1980, Metaizeau proposed intramedullary nailing as a surgical option for the treatment of radial neck fractures. The main advantage of intramedullary nailing is that it simultaneously allows accurate and stable reduction without disturbing the blood supply [7]. The method designed by Metaizeau, involves the insertion of a specially designed long wire into the marrow cavity of the radius and then towards the radial head for reduction. The elbow is then immobilised for two to three weeks, and the wire is removed after eight weeks. This method must be performed carefully to avoid injury to the sensory branch of the radial nerve and the physis [8]. It has acceptable indirect reduction with the preservation of the lateral periosteum and the epiphyseal vascular supply, associated with internal fixation that prevents displacement during the healing period [9].
In both the cases, we have used same technique with a slight modification with the use of a titanium elastic nail with its tip purposely made more curved.
Both the cases were regularly followed up for a period of 6 months. An above elbow plaster slab was kept for 4 weeks after which both the elbows were mobilized.The Titanium nails were removed after total of 8 weeks. Both the patients had excellent results with good functional range of movements and radiographic union at the end of 8 weeks.
Conclusion
Radial neck fractures in paediatric population pose a major surgical challenge.The techniques of fixation vary from simple immobilisation to open reduction and internal fixation.The results of closed reduction and intramedullary pinning have been shown in literature to be very encouraging giving full radiological and functional recovery in 8 weeks.Though we had only two cases where we used this technique of using titanium elastic nails, we strongly recommend the use of this technique because of simplicity of the procedure, good implant strength and cost factor and the advantages of being a closed procedure.
Clinical Message
We recommend the use of the technique using titanium elastic nails as it has the advantages of being a simple procedure and good implant strength and moreover a closed procedure.
References
1. Falciglia F, Giordano M, Aulisa AG, Lazzaro AD, Guzzanti V. Radial Neck Fractures in Children: Results When Open Reduction Is Indicated. J PediatrOrthop 2014;34:756–762.
2. Rockwood Wilkins. Fractures in children. 7th edition. Lippincott Williams & Wilkins. 2010.
3. Stiefel D, Meuli .Fractures of the neck of the radius in children:early experience with intramedullary pinning. J Bone Joint Surg [Br] 2001;83-B:536-41.vol. 83-B, NO. 4,2001.
4. Herring JA. Tachdjian’sPediatric Orthopaedics, 4th Edition.
5. Mataizeau JP. Reduction and osteosynthesis of radial neck fractures in children by centromedullary pinning. Injury 2005 Feb;36Suppl 1:A75-7.
6. Steele JA, Graham HK. Angulated radial neck fractures in children: A prospective study of percutaneous reduction. J Bone Joint Surg [Br] 1992;74-B:760-4.
7. Devgan A, Singh R, Kumar S, Verma, Magu NK, Siwach RC. Indirect Reduction and Intramedullary Pinning in Severely Displaced Radial Neck Fractures in Children. International Journal of Clinical Medicine 2011;2:75-78.
8. Cha SM, Shin HD, Kim KC, Han SC. Percutaneous reduction and leverage fixation using K-wires in paediatric angulated radial neck fractures. International Orthopaedics (SICOT) (2012) 36:803–809.
9. Tarallo L, Mugnai R, Fiacchi F, Capra F, Catani F. Management of displaced radial neck fractures in children: percutaneous pinning vs. elastic stable intramedullary nailing. J OrthopaedTraumatol (2013;14:291–297.
| How to Cite This Article: Bandekar SM, Desai MR. Management of Displaced Radial Neck Fractures with Closed Technique using Titanium Elastic Nail and Review of Literature: A Case Report . Journal of Orthopaedic Case Reports 2015 Oct-Dec;5(4): 64-67. Available from: https://www.jocr.co.in/wp/2015/10/01/2250-0685-349-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


