
[box type=”bio”] What to Learn from this Article?[/box]
Adrenal adenoma can present with insufficiency fractures of the feet.
Case Report | Volume 5 | Issue 4 | JOCR Oct-Dec 2015 | Page 77-78| L L LiYeung, T H Lui. DOI: 10.13107/jocr.2250-0685.353 .
Authors: L L LiYeung[1], T.H. Lui[1]
[1]Department of Orthopaedics and Traumatology, North District Hospital, 9 Po Kin Road, Sheung Shui, NT, Hong Kong SAR, China.
Address of Correspondence
Dr. Lui,Tun Hing,
Department of Orthopaedics and Traumatology, North District Hospital, 9 Po Kin Road, Sheung Shui, NT, Hong Kong SAR, China.
Email: luithderek@yahoo.co.uk.
Abstract
Introduction: Symptomatic adrenal adenoma usually presents with systemic symptoms. Depending on the function of the adenoma, the patient can present with pheochromocytoma-like symptoms; primary hyperaldosteronism and Cushing syndrome (weight gain, weakness, depression, and bruising).
Case report: A 41 year-old lady presented with multiple metatarsal and phalangeal fractures of the both feet without significant injury. DEXA scan showed evidence of osteoporosis. Investigations showed that the picture was compatible with adrenal Cushing syndrome. Computed tomogram showed bilateral adrenal adenoma. Adrenal cortex scintigraphy with NP-59 scan showed hyperfunctioning right adrenal adenoma. Laproscopic R adrenalectomy was performed and histological study confirmed adrenal cortical adenoma with adjacent cortical atrophy suggestive of a functioning adenoma. Post-operatively, she was put on hydrocortisone replacement and recovered well.
Conclusion: Adrenal adenoma can present with insufficiency fractures of the feet.
Keywords: insufficiency fracture; secondary osteoporosis; stress; Cushing syndrome.
Introduction
Symptomatic adrenal adenoma usually presents with systemic symptoms. Depending on the function of the adenoma, the patient can present with pheochromocytoma-like symptoms (palpitations, sweating, headache, abdominal pain and labile hypertension); primary hyperaldosteronism (hypertension and unprovoked hypokalemia) and Cushing syndrome (weight gain, weakness, depression, and bruising). We reported a case of bilateral adrenal adenoma who presented with multiple insufficiency fracture of both feet.
Case Report
A 41 years-old lady presented to us with fracture of the base of her left fifth metatarsal after an inversion sprain (Fig 1). She was treated conservatively with a wooden based sandal and the fracture healed. She had sudden onset of left forefoot pain eight months later without any preceding injury. Radiographs showed fracture of her left second metatarsal with callus formation (Fig 2). Clinically, there was no neurological deficit of the feet. Blood test did not show any evidence of diabetes mellitus. She came back 1 year later for spontaneous onset of left 4th toe pain. Radiographs showed old fractures of bases of bilateral fifth metatarsals, proximal phalanges of bilateral third toes, left second metatarsal with callus formation and crack fracture of the proximal phalanx of the left fourth toe (Fig 3). She was newly diagnosed to have diabetes mellitus but the sensation of the feet was still intact. DEXA scan showed T-score of -3.0 over L2-4. She was not menopausal. Investigations were performed to look out the cause of secondary osteoporosis. Overnight Dexamethasone Suppression Test (ONDST) was 660nmol/L which was non suppressible. 24-hour urine cortisol level was 605nmol/day with urine output of 2.06L. The serum cortisol reached peak level of 699 in low dose short synacthen test (LDSST) and the ACTH level was less than 1.6. Computed tomogram showed bilateral adrenal adenoma (Fig 4). In order to plan for surgery, the functionality of the adenomas needed to be determined. Adrenal cortex scintigraphy with NP-59 scan showed hyperfunctioning right adrenal adenoma. Laproscopic right adrenalectomy was performed. Post-operatively, she was put on hydrocortisone replacement and recovered well.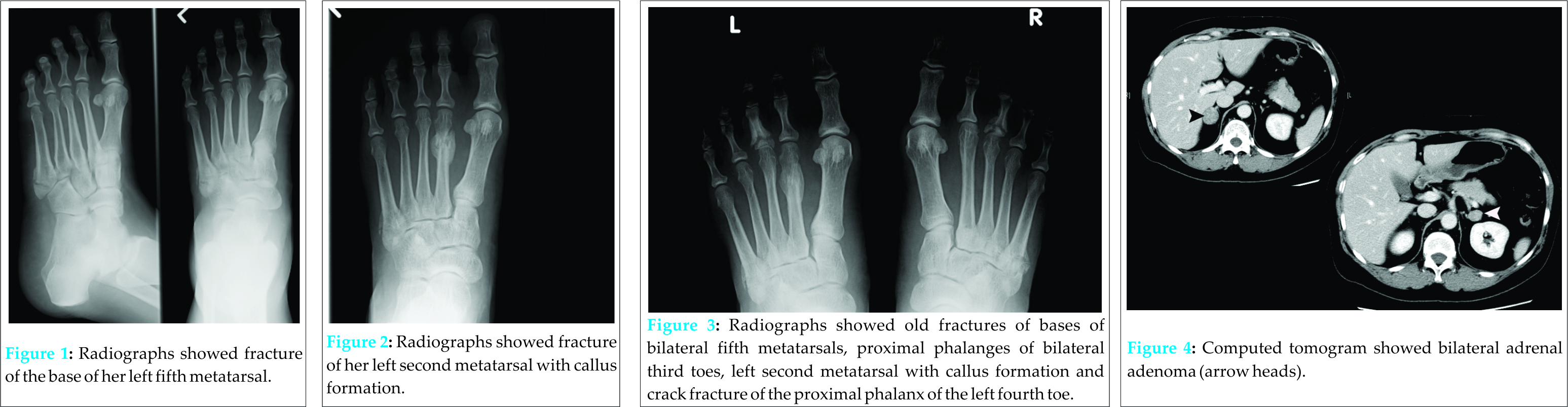
Discussion
Multiple metatarsal and phalangeal fractures of the foot of different ages without any significant injury are uncommon. The differential diagnosis on the top of the list is Charcot neuroarthropathy. This lady was newly diagnosed to have diabetes mellitus. However, there was no neurological deficit of the lower limbs. The other consideration is stress fractures of the foot. Stress fracture can be divided into fatigue fracture and insufficiency fracture. This lady is a housewife and not involved in any activity that can contribute to fatigue fracture. DEXA scan was performed as insufficiency fracture was suspected [1,2] and the result confirmed the presence of osteoporosis. She was still pre-menopausal and was screened for secondary causes of osteoporosis [3]. TSH level was 0.55. Overnight Dexamethasone Suppression Test (ONDST), urine cortisol level, low dose short synacthen test (LDSST) and the ACTH level was compatible with adrenal Cushing syndrome. Adrenal adenoma is a cause of Cushing syndrome that is surgically treatable [4]. The presence of adenoma in both adrenal glands needs further study of the functionality of the tumours for surgical planning. Adrenal cortex scintigraphy with NP-59 scan is a useful investigation tool to determine the activity of the tumours. Right adrenalectomy was performed because it was the functioning tumour. Histological study confirmed adrenal cortical adenoma with adjacent cortical atrophy suggestive of a functioning adenoma.
The clinical significance of this report is that it demonstrates the multiple phalangeal and metatarsal fractures can be the sole presentation of adrenal adenoma.
Conclusion
Adrenal adenoma can present with insufficiency fractures of the feet.
Clinical Message
Causes of secondary osteoporosis should be investigated in pre-menopausal patient with insufficiency fracture of the feet..
References
1. Newton MT, Archer JA, Scruggs M, Geter K, Al-Dabagh H, Lloyd E et al. Low bone mass and fractures on foot radiographs: missed opportunities to evaluate for osteoporosis: a pilot study. J Am Podiatr Med Assoc. 2009;99:1-7. PMID:19141714.
2. Kaye RA. Insufficiency stress fractures of the foot and ankle in ostmenopausal women. Foot Ankle Int. 1998;19:221-4. PMID:9578100.
3. Hosmer WD, Genant HK, Browner WS. Fractures Before Menopause: A Red Flag for Physicians. Osteoporos Int 2002;13:337–341. PMID: 12030549.
4. Nakamura A, Shimizu C, Nagai S, Taniguchi S, Umetsu M, Atsumi T et al. Unilateral adrenalectomy improves insulin resistance and polycystic ovaries in a middle-aged woman with virilizing adrenocortical adenoma complicated with Cushing’s syndrome. J Endocrinol Invest. 2007;30:65-9. PMID:17318025.
| How to Cite This Article: L L LiYeung, T H Lui. Bilateral Adrenal Adenoma Presented As Multiple Metatarsal And Phalangeal Fractures. Journal of Orthopaedic Case Reports 2015 Oct-Dec;5(4): 77-78. Available from: https://www.jocr.co.in/wp/2015/10/01/2250-0685-353-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


