
[box type=”bio”] What to Learn from this Article?[/box]
1. Diagnosing rare injuries require high index of suspicion and aim is not to miss them.
2. Adequate reconstruction with or without suture anchors is required in high demanding patients eso in sports persons and athletes.
Case Report | Volume 5 | Issue 4 | JOCR Oct-Dec 2015 | Page 79-81| Rajendra Annappa, Prem Kotian, Janardhana Aithala P, Srikanth Mudiganty. DOI: 10.13107/jocr.2250-0685.354 .
Authors: Rajendra Annappa[1], Prem Kotian[1], Janardhana Aithala P[1], Srikanth Mudiganty[1]
[1]Department of Orthopaedics, Kasturba Medical College, Mangalore 575001, Manipal University. India.
Address of Correspondence
Dr. Rajendra Annappa
Address: Assistant Professor, Department of Orthopaedics, Kasturba Medical College, Mangalore-575001, Manipal University. India.
E-mail: rajendra.orthopaedics@gmail.com
Abstract
Introduction: Thumb carpometacarpal dislocation is a rare injury with many treatment options described in literature.
Case Report: A 47-years-old male patient presented to hospital with an isolated dorsal dislocation of the thumb carpometacarpal joint. Closed reduction of the dislocation could be easily done but joint was grossly unstable and redislocated. Repair of ruptured dorsoradial ligament and joint capsule was done with immobilization for 6 weeks. At 2-years follow-up evaluation, the patient was pain free and returned to his previous level of activity. No restriction of carpometacarpal movements or residual instability was noticed. Radiographic examination showed normal joint congruity and no signs of osteoarthritis.
Conclusion: Capsuloligamentous repair can be considered the treatment of choice in thumb carpometacarpal dislocations with instability after closed reduction.
Conclusion: Capsuloligamentous repair can be considered the treatment of choice in thumb carpometacarpal dislocations with instability after closed reduction.
Keywords: First carpometacarpal dislocation, Ligament reconstruction of dislocation, thumb carpometacarpal joint instability
Introduction
Thumb determines prehension in the hand. The main function of prehension, opposition takes place at carpometacarpal joint of thumb [1]. Fracture dislocation of thumb carpometacarpal joint, Bennetts fracture is a more common injury than isolated dislocation. Carpometacarpal (CMC) dislocation accounts for less than 1%of all hand injuries [2]. It is the result of force transmitted axially when thumb is in partial flexion. Dislocation is associated with capsular and ligamentous injuries due to which instability persists even after reduction [3,4,5].
Treatment of choice for CMC joint dislocation is controversial. Different options for treating dislocation are closed reduction and cast application, closed reduction and K wire fixation, open reduction and ligamentous reconstruction. Case reports available in literature have limited evidence to come to an conclusive and universally accepted management guidelines [6-11]. We managed a case of dislocation of thumb CMC joint by open reduction and repair of capsule and ligament and followed it up for 2 years with excellent results.
Case Presentation
A 47 year old, right hand dominant banker presented to emergency department after a fall from motorcycle. There was pain and swelling at the base of left thumb. On examination there was deformity and tenderness at the radial side of hand at the base of the thumb and restricted thumb movements. Anteroposterior and oblique radiographs of the hand showed dislocation of trapeziometacarpal joint. Patient also had an undisplaced lateral malleolar fracture which was managed conservatively.
Fig 1
Procedure
Closed reduction was easily possible with traction and minimal manipulation without anaesthesia but joint was found to be grossly unstable and surgical intervention was planned. Regional anaesthesia was given and tourniquet was applied. Incision was given on the dorsoradial side of wrist along the border of first metacarpal. The superficial radial nerve, branch of radial artery were retracted. Dorsal ligament complex was torn intrasubstance and capsular tear was also preset but articular cartilage was intact. Joint was stabilized using a K wire with thumb in abduction and extension.. End to end capsular repair was done by 3.0 vicryl sutures and ligament repair was done by nonabsorbable sutures. This was reinforced by a slip of flexor carpi radialis tendon which was passed under the tendon of abductor pollicislongus with few intermittent sutures with nonabsorbable sutures. Wound closure was done and below elbow cast was applied. Post operatively reduction was confirmed by check X-ray. Suture removal was done on 12th day. K wire was removed after 6 weeks and mobilization started.
Fig 2, Fig 3

Results
Patient gained painless, complete range of movements by 6 months and returned to his occupation with no difficulty in carrying out any preinjury level activity. At the end of 2 years, patient had full range of movements and no instability. Radiographic examination showed no signs of subluxation or early osteoarthritis.
Fig 4, Fig 5

Discussion
Thumb CMC joint is biconcavoconvex joint which permits movements in multiple planes. The articular surfaces of the CMC joint of the thumb resemble two reciprocally opposed saddles whose transverse axes are perpendicular. The shape of the articular surfaces provides a degree of intrinsic stability, but the ligaments and joint capsule play the principal role in stabilization. There are four major ligaments: volar (anterior oblique), intermetacarpal, dorsoradial, and dorsal oblique (posterior oblique) [1,4-7]. Strauch et al in a cadaveric study found that the dorsoradial ligament complex was the primary restraint to dorsal dislocation and responsible for obtaining joint stability in thumb opposition [5].
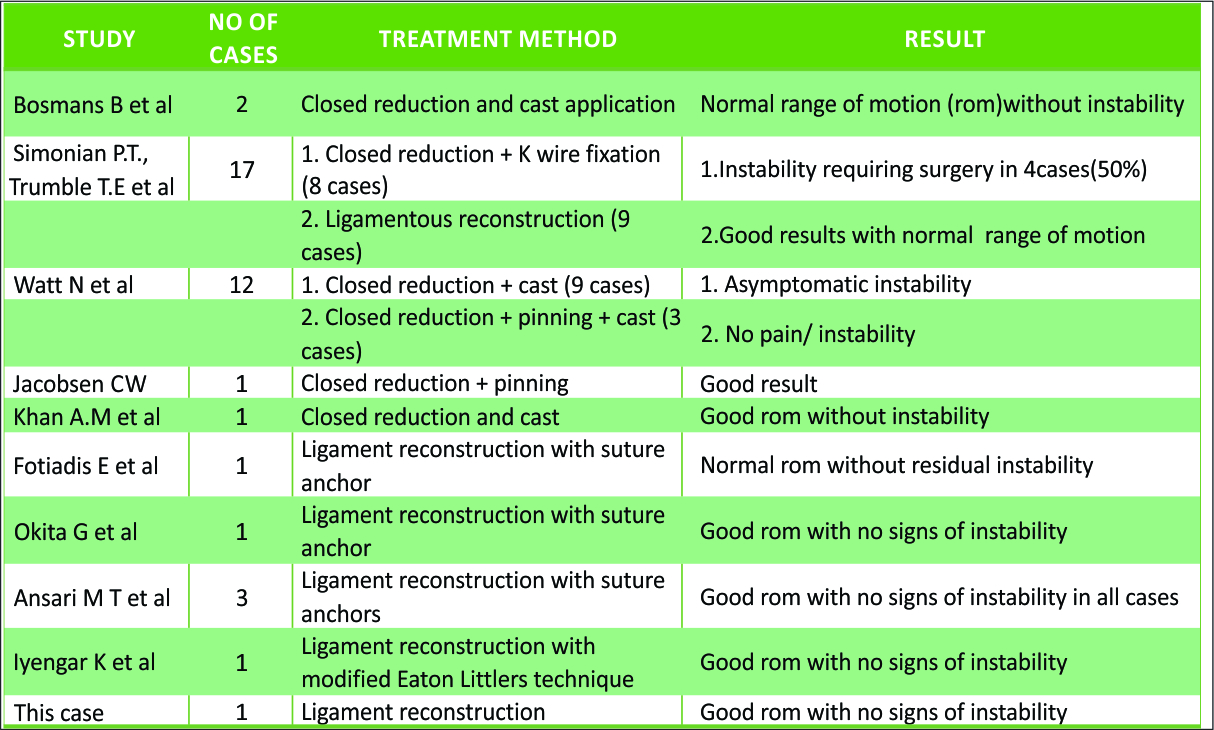
Closed reduction and cast application and percutaneous pinning have been advocated by many authors. Overall out of 16 reported cases 6 required surgery for instability. Closed reduction and K-wire fixation was associated with more complication and revision surgery in 7 cases [10-16]. Repair of ligaments has been found to be associated with least complications. Simonian and Trumble compared early ligamentous reconstruction with closed reduction and pinning. Four out of 8 patients initially managed with closed reduction and percutaneous k wires underwent revision with open reduction with ligamentous reconstruction because of recurrent instability. Based on many reports, it can be concluded closed reduction and casting can be definitive treatment option in cases where thumb carpometacarpal joint was found to be stable after immediate and anatomic reduction [4].
Isolated CMC dislocation is associated with various degrees of joint capsule and ligament damage. We intraoperatively found torn dorsoradial ligament complex but intact volar ligaments. This was also found in case reports by Fotiadis et al (1 case) and Shah and Patel (4 cases) where dorsal capsuloligamentous complex was completely ruptured but the volar ligament was intact. Repair of capsule and ligaments is to be considered in such cases.
Fig 6
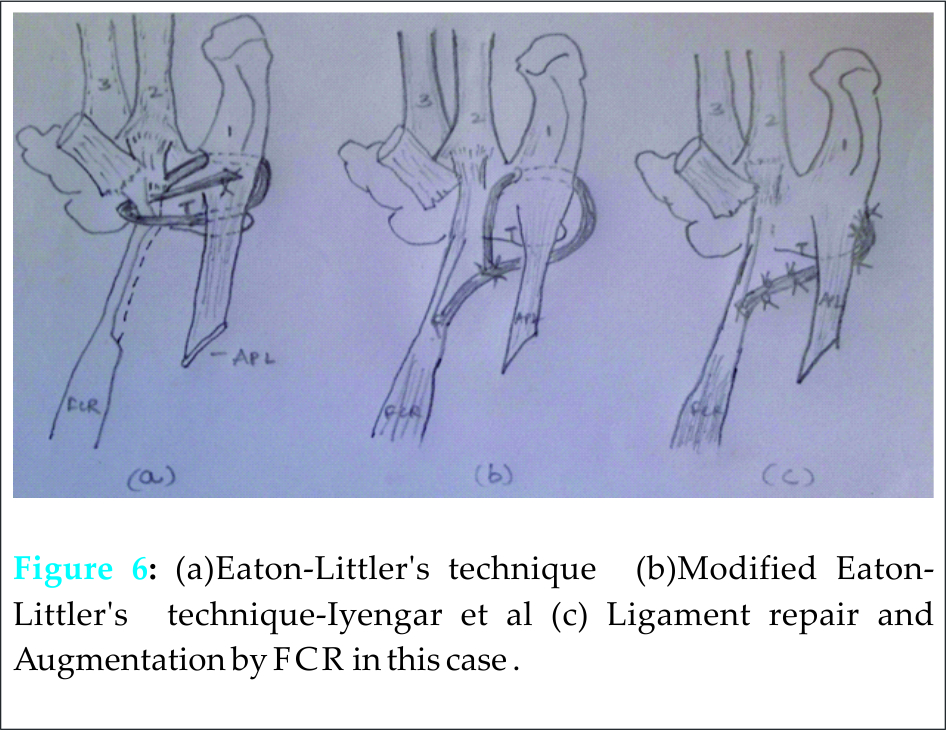
Eaton-Littler described ligament reconstruction method for painful thumb with hypermobility [14]. In this technique, the FCR slip, based distally is released in continuity till its insertion on the index metacarpal. It is then re-routed through a drill hole in the base of the thumb metacarpal, under the abductor pollicislongus insertion and secured on the radial side of the joint. Iyengar et al, [15] modified this classical technique by restricting the release of FCR slip 2 to 2.5 cm short of its insertion. This slip was then directed in an oblique manner to reproduce the direction of active action of the anterior oblique ligament. They routed the FCR slip through the extra-articular bone tunnel and sutured in a taut position back to itself. The routed FCR slip covered both the dorsal (Dorso-radial ligament) and volar aspect (volar beak ligament) of the carpometacarpal joint by passing under the abductor pollicislongus tendon. In our study ligament and capsule was repaired end to end and reinforced with slip of FCR tendon sutured to repaired ligament and capsule on either side of joint line. Alternatively suture anchors can be used to reconstruct ligaments. Fotiadis et al, Okita et al and Ansari et al have used suture anchors effectively with good results in patients with high demands [14-15].
Conclusion
Careful assessment and high index of suspicion is required to identify ligament injury after thumb CMC dislocation. Ligament repair is indicated for instability after reduction. Ligament repair is associated with uniformly good results in various studies in literature. Different methods of ligament reconstruction are available for operating surgeon to choose.
Clinical Message
Diagnosing ligament injury is important in isolated carpometacarpal dislocations. Complications of inadequate treatment can increase recurrent instability, joint degeneration and chronic pain. Repair of capsuloligamentous tear is treatment of choice for instability after closed reduction of thumb CMC dislocations. Stable joints after reduction can be managed with casting or percutaneous pinning. In patients with high demands reconstruction with suture anchors can be considered.
References
1. Edmunds J.O. Current concepts of the anatomy of the thumb trapeziometacarpal joint. J Hand Surg Am. 2011;36:170–182.
2. Mueller JJ. Carpometacarpal dislocations: report of five cases and review of the literature. J Hand Surg 1986;11A: 184–188.
3. Bosmans B., Verhofstad M.H.J., Gosens T. Traumatic thumb carpometacarpal joint dislocations. J Hand Surg. 2008;33A:438–441.
4. Simonian P.T., Trumble T.E. Traumatic dislocation of the thumb carpometacarpal joint: early ligamentous reconstruction versus closed reduction and pinning. J Hand Surg Am. 1996;21:802–806.
5. Strauch R J, Behrman MJ, Rosenwasser MP: Acute dislocation of the carpometacarpal joint of the thumb: an anatomic and cadaver study. J Hand Surg 1994;19A:93-98.
6. Bettinger P.C., Linscheid R.L., Berger R.A., Cooney W.P., III, An K.N. An anatomic study of the stabilizing ligaments of the trapezium and trapeziometacarpal joint. J Hand Surg. 1999;24A:786–798.
7. Colman M., Mass D.P., Draganich L.F. Effects of the deep anterior oblique and dorsoradial ligaments on trapeziometacarpal joint stability. J Hand Surg. 2007;32A:310–317.
8. Watt N., Hooper G. Dislocation of the trapezio-metacarpal joint. J Hand Surg Br. 1987 Jun;12:242–245.
9. Jacobsen CW, Elberg JJ: Isolated carpometacarpal dislocation of the thumb. Scand J PlastReconstrSurg 1988;22:185-186.
10. Khan A.M., Ryan M.G., Teplitz G.A. Bilateral carpometacarpal dislocations of the thumb. Am J Orthop. 2003 Jan;32:38–41.
11. Fotiadis E., Svarnas T., Lyrtzis C., Papadopoulos A., Akritopoulos P., Chalidis B. Isolated thumb carpometacarpal joint dislocation: a case report and review of the literature. J OrthopSurg Res. 2010;5:16.
12. Okita G., Anayama S., Sato N., Haro H. Surgical reconstruction using suture anchor for dislocation of the carpometacarpal joint of the thumb: a case report. Arch Orthop Trauma Surg. 2011;131:225–228.
13. Ansari M T, M. Kotwal P P, Morey V M. Primary repair of capsuloligamentous structures of trapeziometacarpal joint: A preliminary study. J ClinOrthop Trauma. 2014 Dec; 5(4): 185–192.
14. Eaton R.G., Lewis B., Lane M.D., Littler J.W., Keyser J.J. Ligament reconstruction for the painful thumb metacarpal: a long term assessment. J Hand Surg [Am] 1984;9:692–699.
15. Iyengar K, Gandham S, Nadkarni J, Loh W. Modified Eaton-Littler’s Reconstruction for Traumatic Dislocation of the Carpometacarpal Joint of the Thumb—A Case Report and Review of Literature, J Hand Microsurg. 2013,5(1):36-42.
| How to Cite This Article: Annappa R, Kotian P, Aithala PJ, Mudiganty S. Ligamentous Reconstruction of Traumatic Dislocation of Thumb Carpometacarpal Joint: Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2015 Oct-Dec;5(4): 79-81. Available from: https://www.jocr.co.in/wp/2015/10/01/2250-0685-354-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


