
[box type=”bio”] What to Learn from this Article?[/box]
The importance of clinical examination and to recognise suttle signs especially in paediatric age groups which is necessary to reach a correct clinical diagnosis.
Case Report | Volume 6 | Issue 1 | JOCR Jan-Mar 2016 | Page 8-10 | Kunal R.Bansal, Ajay S. Chandanwale. DOI: 10.13107/jocr.2250-0685.363
Authors: Kunal R.Bansal[1], Ajay S. Chandanwale[1]
[1] Department of Orthopaedics, B J Govt Medical College, Pune, Maharashtra. India.
Address of Correspondence
Dr. Kunal R. Bansal,
A-503 , Ganga Melrose, S No 60/A , Sopan Baug, Pune – 411001, Maharashtra. India. E-mail: kun_bansal@yahoo.co.in
Abstract
Introduction: Spinal cord injury in children frequently occurs without fracture or dislocation. SCIWORA is a syndrome occurring when the spinal cord sustains neural damage during a traumatic event without positive radiographic findings. The incidence of SCIWORA was found to be 8% to 32% in various studies with very few cases documented in children below the age of 1 year. We report such a case of spinal cord injury without radiological abnormality in an 8 months old female child.
Case Report: An 8 months old female child was brought to the emergency room after a history of fall from the bed four days back. External spine examination revealed no abnormality. She had no upper or lower limb movements, both active and withdrawal movements with painful tactile stimuli, power was grade 0; are flexic; abdominal ,cremasteric and anal reflexes were absent, bladder was palpable and urine could be expressed on manual pressure. MRI of cervical spine with screening of whole spine: suggestive of non hemorrhagic cord edema at C4 level, with suspicious tear of anterior longitudinal ligament at that level. The child was immobilized in pediatric cervical collar and treatment was initiated with corticosterioids and the dose adjusted as per age of the patient. A paediatric physiotherapist started with physical therapy after four days of commencement of treatment.
Conclusion: In present times with wide spread use of MRI, the definition of SCIWORA is slowly turning towards spinal cord injury without neuroimaging abnormality [4]. Traumatic spinal cord infarction is a special type of SCIWORA which presents with normal radiology with delayed neurological deterioration [1]. Corticosteroid usage has been useful in cases of SCIWORA as proved by NASCISII Trial.
Keywords: SCIWORA- Spinal cord injury without radiological abnormality, MRI –Magnetic resonance imaging, CT scan –Computerised tomographic imaging.
Introduction
Spinal cord injury in children frequently occurs without fracture or dislocation. SCIWORA is a syndrome occurring when the spinal cord sustains neural damage during a traumatic event without positive radiographic findings. The incidence of SCIWORA was found to be 8% to 32% in various studies [8] with very few cases documented in children below the age of 1 year,, We report such a case of spinal cord injury without radiological abnormality in an 8 months old female child.
Case Report
An 8 month old female child was brought to the emergency room after a history of fall on her face from the bed four days back with hyperextension of neck and sudden onset weakness in both upper & both lower limbs. Parents gave the history that the child was all right four days back & was able to stand with support. History of head injury, chest, and abdominal trauma was not reported by the parents.. The child had no history of altered consciousness, vomiting, ear, nose bleed, convulsion, or fever with vomiting and diarrohea. Birth history and perinatal history was not significant. Patient was the second child with one elder sister who was 3 years old and was normal for her age, with no history of prior treatment.
Clinical Examination
The child was afebrile, conscious & normocephalic with no bulge of anterior fontanelle. There was no evidence of external injury to head, chest, abdomen and extremities. There was no evidence to suggest external violence or abuse. The external spine examination revealed no abnormality.
She had no upper or lower limb movements, both active and withdrawal movements with painful tactile stimuli, power was grade 0; are flexic; abdominal, cremasteric and anal reflexes were absent, bladder was palpable and urine could be expressed on manual pressure.
Investigations
Haemoglobin-13.1g/dl, Total WBC count-6,800/mm3., Differential counts- neutrophils-68%, lymphocytes-24%, monocytes-5%, eosinophils,2%, basophils-1%. Peripheral smear examination waswithin normal limits.
Urea-16mg%, Creatinine-0.8 mg% Total bilirubin-0.9 mg%, Random blood sugar-98mg%
Roentgenography:
No obvious trauma related abnormalities were noted.
Computed Tomography Scan
Brain (plain+ contrast): No evidence of trauma related abnormality.
Magnetic ResonanceImaging: Imaging of cervical spine with screening of whole spine: suggestive of non hemorrhagic cord edema at C4 level, with suspicious tear of anterior longitudinal ligament at that level.
Treatment
The child was diagnosed as having traumatic spinal cord involvement based on clinical findings and above investigations; the child was immobilized in pediatric cervical collar. As child was presented 4 days after trauma she was treated with Inj Dexamethasone 0.6mg/kg stat dose followed by 0.15mg/kg Q.I.D. for 2 weeks along with Inj Ranitidine 1mg/kg/dose B.I.D & Syp Paracetamol 15mg/kg/dose. After 2 weeks, child was shifted on oral Tablet Prednisolone 5mg Q.I.D. crushed and dissolved in water for 2 wks and tapering was done.
The Physiotherapy was given by pediatric physiotherapist after 4 days of starting treatment. The girl started regaining power in lower limb first followed by upper limbs. After 15 days, the girl was able to turn to prone position on her own in bed. The child had good neck holding in pull to sit test, the child had started active movements of both lower and upper limbs. The child was discharged after 1 month of hospital stay on pediatric cervical collar which is to be kept for 12 weeks. Parents have been asked to follow up after 1 month.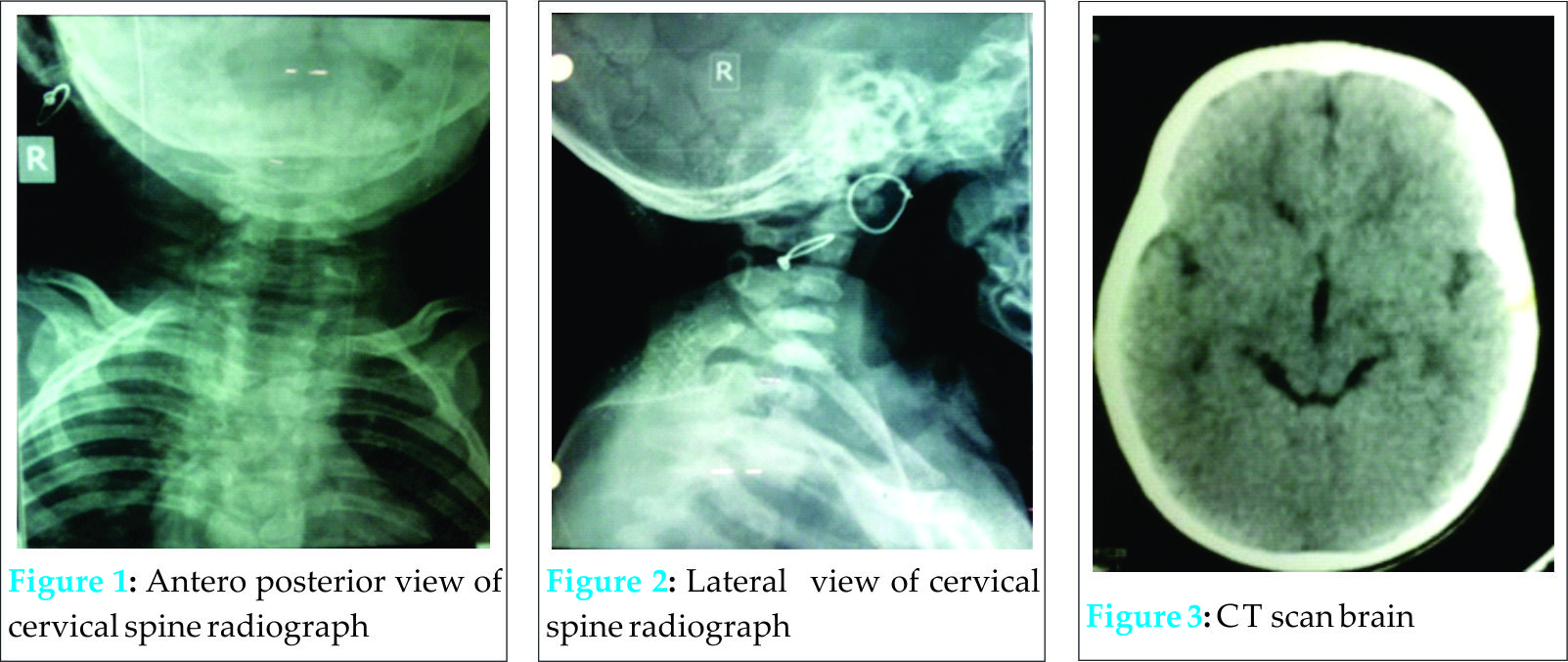
Discussion
In 1982, Pang and Wilberger [8]defined this disorder as marked by objective signs of myelopathy resulting from trauma, with no evidence of ligamentous injury or fractures on plain Xray films or tomographic studies. The original definition excludes penetrating trauma, electrical shock, obstetric complications, and congenital spine anomalies. Most studies of traumatic myelopathy in children report an incidence of SCIWORA of 8% to 32% [12].
This disorder is more common in children younger than 8 years of age [8,10]. With the advent of MRI, there have been description of various injury pattern to the spinal cord on MRI like cord transection, major hemmorahge, minor hemmorahge, disc prolapsed, contusion, cord edema, muscular and interspinous ligament tear and normal [4,6,9].
Male to female ratio is 1.6:1 [2]. Majority of injuries occurred in upper cervical cord C1-C4 [2]. Injuries are children less than 3 years is most commonly due to motor vehicle accident and domestic violence [2], injuries in adolescents are due to outdoor sporting activities[2].
Mechanism of neural injury most often relates to inherent elasticity of juvenile spine, which permits self-reducing but significant inter segmental displacements when subjected to flexion extension and distraction forces [3, 8].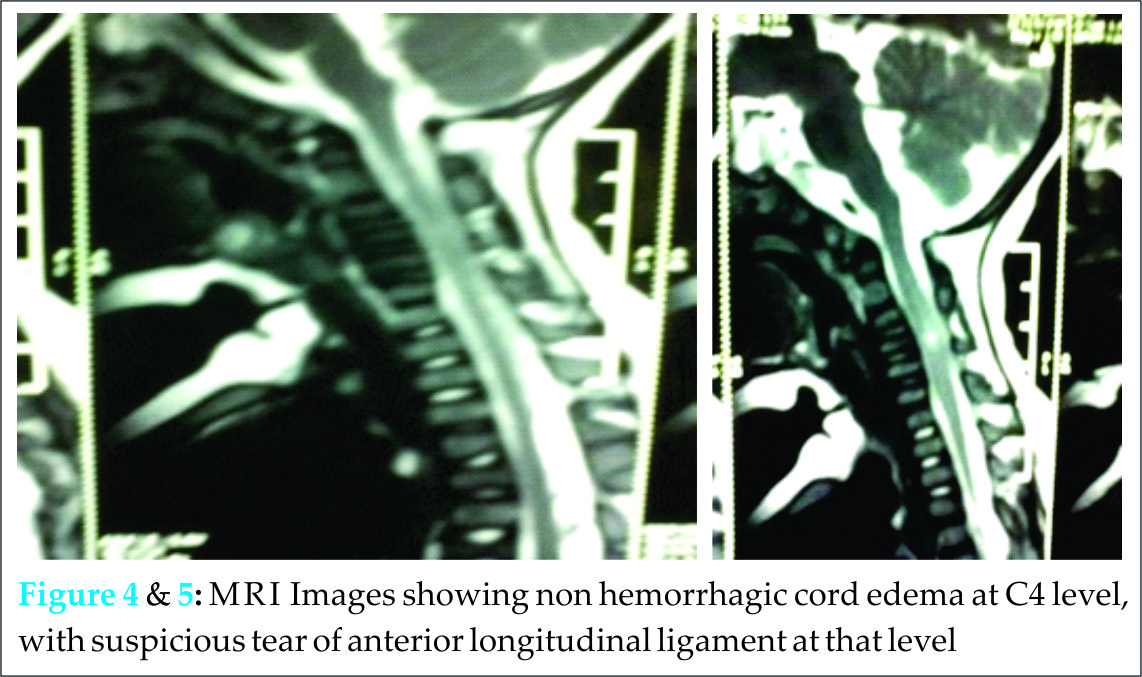
The other associated injuries are head injuries, chest injuries. Associated injuries increase the likelihood of significant cord injury. Low GCS scores on initial examination indicate poor prognosis in terms of recovery [7]. GCS scores of 15/15 have correlation of lower grades of cord injury on MRI [7].
Long term neurological outcome in children with SCIWORA is determined by admission neurological status [8]. The outcome can be improved by ruling out occult injuries which would lead to recurrent SCIWORA and also to identify patients with delayed neurological deterioration, who are normal on initial neurological examination but show deterioration later can be identified by transient warning symptoms of transient paresthesias, subjective paralysis and lhermittes phenomenon 30 minutes to 4 days prior to onset of deterioration [8].
Bracing is recommended in cases of SCIWORA as there is some occult instability in these cases which may lead to recurrent episodes [5, 8].
However, in some studies these minor recurrent episodes of SCIWORA recovered completely and bracing did not provide additional benefits in preventing these episodes [1].
Abnormal somatosensory evoked potential also have correlation with prognosis of neurological recovery in SCIWORA [9].
Injury prevention, prompt recognition, use of MRI and timely bracing remain key measures to improve outcome in cases of SCIWORA [9].
Conclusion
In present times with wide spread use of MRI, the definition of SCIWORA is slowly turning towards spinal cord injury without neuroimaging abnormality [4]. Traumatic spinal cord infarction is a special type of SCIWORA which presents with normal radiology along with delayed neurological deterioration [1]. Corticosteroid usage has been useful in cases of SCIWORA as proved by NASCISII Trial
Clinical Message
Early detection by maintaining high index of suscpicion, MRI findings, bracing, early adoption of steroids are cornerstones in the treatment of SCIWORA. Further avenues for research are detecting recurrent episodes in cases of SCIWORA, severity of these attacks, end point of bracing in cases of occult instability for prevention of these attacks and measures for early detection of individuals prone for such incidences.
References
1. BoschPP,Vogt MT,WogtWT. Pediatric spinal cord injury without radiological abnormality(sciwora):the absence of occult instability and lack of indication for bracing. Spine Phila Pa 1976;2002:27(24);2788.
2. BrownRL;Brunn MA;Garcia VF. Cervical spine injuries in children: review of 103 patients treated conservatively at level 1 pediatric trauma centre.Journal Of Pediatric surgery 2001:36(8);1107.
3 CirakB, Zigfeld S,Knight VM,Chang D,AvellinoAM,Paidas CN. Spinal injuries in children. Journal of pediatric surgery 2004;39(4);607.
4. Hendey GW,WolfsonAB,Moiver WR,Hoffman JR. Spinal cord injury without radiological abnormality :results of national emergency x-radiography utilization study in cases of blunt cervical trauma, ,National emergency x-radiography utilization study group. J Trauma. 2002;53(1):1.
5. Pediatric spinal cord injury without radiographic abnormality: a meta-analysis.Launay F, Leet AI, Sponseller PDClin Orthop Relat Res. 2005;
6. Liao CC, Lui TN, Chen LR, Chuang CC, Huang YCJ. Spinal cord injury without radiological abnormality in preschool-aged children: correlation of magnetic resonance imaging findings with neurological outcomes. Neurosurg. 2005;103(1):17.
7. Martin BW, Dykes E, Lecky FE. Patterns and risks in spinal trauma. Arch Dis Child 2004;89(9):860.
8. Pang D, Pollack IF. Spinal cord injury without radiographic abnormality in children–the SCIWORA syndrome. J Trauma 1989;29(5):654.
9. Pang D. Spinal cord injury without radiographic abnormality in children, 2 decades later. Neurosurgery 2004;55(6):1325.
10. Polk-Williams A, Carr BG, Blinman TA, Masiakos PT, Wiebe DJ, Nance ML. Cervical spine injury in young children: a National Trauma Data Bank review.J Pediatr Surg. 2008;43(9):1718.
11. Robles LA. Traumatic spinal cord infarction in a child: case report and review of literature. Surg Neurol. 2007;67(5):529.
12. Yucesoy K, Yuksel KZ. SCIWORA in MRI era Clin Neurol Neurosurg. 2008;110(5):429.
| How to Cite This Article: Bansal KR, Chandanwale AS. Spinal Cord Injury without Radiological Abnormality in an 8 Months Old Female Child: A Case Report. Journal of Orthopaedic Case Reports 2016 Jan-Mar;6(1): 8-10. Available from: https://www.jocr.co.in/wp/2016/01/02/2250-0685-363-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


