
[box type=”bio”] What to Learn from this Article?[/box]
Surgical management can be a better option in managing coracoid fracture in comparison to conservative management since early movement and early return to previous occupation is quicker after surgical management.
Case Report | Volume 6 | Issue 1 | JOCR Jan-Mar 2016 | Page 37-39 | Shreedhar Archik, Saurav Narayan Nanda, Sanjay Tripathi, Ashlesh Choudhari, Harshada Rajadhyaksha DOI: 10.13107/jocr.2250-0685.372
Authors: Shreedhar Archik[1], Saurav Narayan Nanda[1], Sanjay Tripathi[1], Ashlesh Choudhari[1], Harshada Rajadhyaksha[2]
[1] Department of Orthopaedic, Lilavati -Shushrusha- Hinduja healthcare, Khar – Global Hospitals, Mumbai. Maharashtra. India.
[2] PGDR(Rehabilitation med)Director & consultant in Prakruti Sports rehabilitation centre. Mumbai. Maharashtra. India.
Address of Correspondence
Dr. Saurav Narayan Nanda,
Lilavati Hospital & Research Centre, Bandra(W), Mumbai – 400050. Maharashtra. India. E mail – saurav.scb@gmail.com
Abstract
Introduction: Isolated coracoid fractures are rare and few scattered cases are reported in literature. Coracoid fractures can be missed and the treatment for coracoid process fractures is still controversial. The case presented here is of an isolated coracoid process fracture which was treated surgically.
Case Report: A 15-year-old male presented after 4 days of injury complaining of persistent pain in the right shoulder following a jerk during bowling. Physical examination revealed tenderness in the left shoulder. There was pain on abduction and external rotation. The neurovascular examination was normal. Osseous avulsion of the distal tip of the coracoid process was confirmed by CT and MRI. The short head of the biceps and coracobrachialis was attached to the avulsed tip, while the pectoralis minor was attached to the coracoid base. The case was managed by open reduction and fixation with a 3.5mm cannulated screw and washer.
Conclusion: Isolated coracoid fracture is a rare entity causing impairment of upper limb movement. It can be diagnosed more accurately by MRI scan and CT scan. In case of young highly demanding individuals like athletes surgical management may be a better option as compared to conservative treatment to achieve early use of the extremity, good radiological union and clinical function.
Key Words: Fracture Coracoid, Isolated Fracture, Associated Injuries, Osteosynthesis.
Introduction
Coracoid fractures are rare fractures [1]. In the shoulder girdle, coracoid process fractures generally accompany dislocation of the acromioclavicular (AC) joint or glenohumeral joint, scapula corpus fracture, clavicular fracture, humerus proximal end fracture or rotator cuff tear [2].
The incidence has been estimated to be between 3% and 13% of all scapular fractures, these constitute 1% of all fractures and 5% of those of the shoulder [3]. Isolated injuries of coracoid are a rare occurrence with few scattered reports in literature [4-6]. Coracoid fractures can be missed and the treatment for coracoid process fractures is still controversial. The case presented here is of an isolated coracoid process fracture which was treated surgically.
Case Report
A 15-year-old male, professional cricket player (spin bowler), presented at the emergency department after 4 days of injury complaining of persistent pain in the right shoulder following a jerk during bowling. Physical examination revealed tenderness in the left shoulder. There was pain on abduction and external rotation. Neurovascular examination was normal.
Patient was advised plain radiograph initially. For a detailed study, MRI shoulder was requested. MRI impression was: 1.3 x 0.4 x 0.9 cm osseous avulsion of the distal tip of the coracoid process. The short head of the biceps and coracobrachialis was attached to the avulsed tip, while the pectoralis minor was attached to the coracoid base (Fig. 1).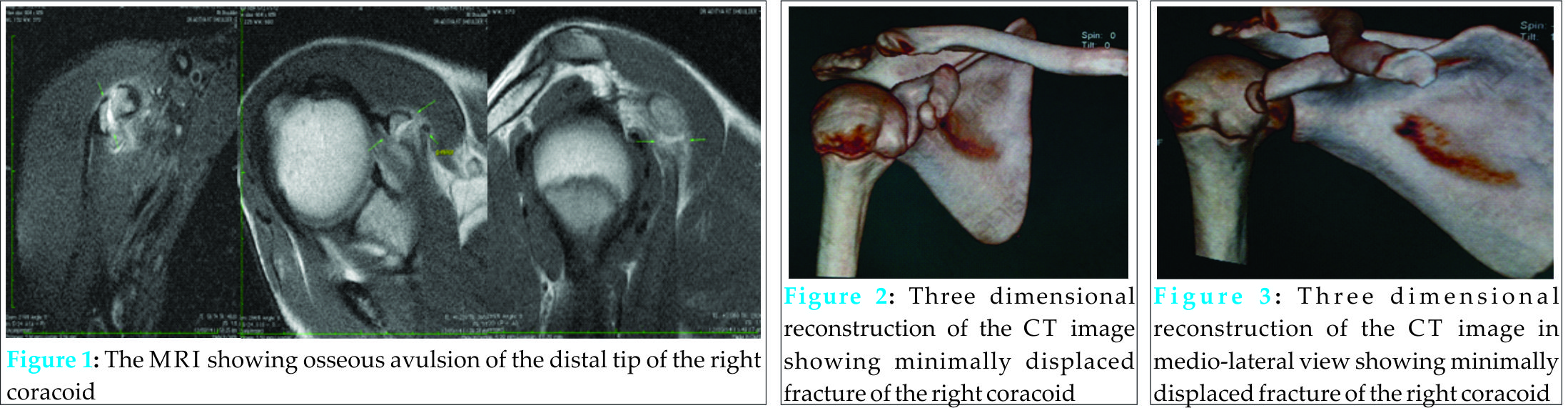
Three dimensional CT scan was done to confirm the diagnosis, and fixation was planned. A fragmented fracture was observed at the base of the coracoid process by CT images (Figs. 2, 3).
Coracoid fracture was an isolated fracture with no other associated fracture clinically or radiologically. The patient was admitted for surgery taking consideration of the age and profession of the patient. After making the incision along the Langer’s line on the coracoid process, the fracture line was reached. After open reduction, fixation was made with a 3.5mm cannulated screw with a washer (Fig. 4). Intra operatively the fragment was assessed to be reduced well.
In immediate post operative X-ray, both screw & the fragment were found to be in proper position (Fig. 5).
Postoperatively, the patient was followed up for 2 weeks with the application of a simple shoulder sling. Passive joint exercises were allowed in the first 2 weeks; from the 3rd postoperative week, active joint movement exercises were started and 5th week onwards shoulder strengthening exercises were commenced. The bone was united and fracture had healed as there was no pain at the fracture site and also muscle strength was adequate at the end of 6th post operative week. The patient returned to his previous occupation pain free and with a full range of joint movement (Fig. 6). The patient was followed up for next 6 months and there was no complaint of pain and difficulties in bowling.
Discussion
Isolated coracoid fractures are extremely rare. All coracoid process fractures constitute approximately 1% of all fractures and 2–13% of scapula fractures [7–9]. Fractures are often seen at the base of the coracoid process and are generally minimally displaced and associated with AC joint injuries [10]. Coracoid fractures may be easily missed. Lal et al., in a case report where surgery had not been applied and Vaienti and Pogliacomi in a series of 9 cases with delayed diagnosis, applied conservative treatment and clearly demonstrated this situation [11, 12]. In cases which cannot be clarified with direct radiographs, the use of CT may be necessary. In a study by Botchu et al. of 7 cases, it was shown that coracoid process fractures can be diagnosed with ultrasonography [13].
In the case presented here, diagnosis was made with CT. An important point related to coracoid fractures is the neurological injury which may accompany the fracture.
Neer stated that in fractures involving the coracoid process, there may be compression on the brachial plexus and suprascapular nerve paralysis and therefore evaluation with electromyography prior to exploration is recommended [14].There are no clear cut guidelines about the preferred modality of treatment of coracoid process fractures. The majority of such fractures are preferably treated conservatively [10]. Most of the previous studies on this subject were in the form of case reports or limited case series with no definite determination of the best treatment modality. The study in literature with the largest number of recruited patients with coracoid process fractures was conducted by Anavian et al. Surgery was applied to 14 coracoid process fractures of 26 patients including scapula fractures and successful results were obtained for all patients [15].
Indications for surgical treatment were painful nonunion, >1 cm displacement, concomitant scapula fracture on the same side and the presence of superior shoulder suspensory complex injuries [15]. In a study by Lal and Bansal of 22 patients, all with coracoid fractures and various shoulder girdle injuries, 10 patients were treated conservatively and nonunion was encountered in 1 patient [8]. Spormann et al. operated on 3 cases of isolated coracoid process fracture and obtained successful results [16].
Again successful results were obtained from surgical treatment applied bySubramanian et al. of an isolated coracoid fracture in an unstable shoulder [17]. Garcia-Elias and Salo applied sling in a patient with a fractured coracoid process in association with shoulder dislocation and reported nonunion of the coracoid process [18]. In studies by Guttentag and Rechtine and Goos, conservative treatment was done to coracoids fractures in athletes and patients who were engaged in heavy manual work, however poor results were obtained [19, 20] in such cases. In coracoid fractures, surgical fixation can be applied with open reduction and internal fixation with screws [16]. Even though the most frequently used method is the anterior approach, indirect reduction and fixation may be applied with a posterior approach [15]. In a study by Bhatia, fluoroscopy-guided percutaneous fixation was applied to a coracoid process fracture which was accompanied by AC joint dislocation [21]. In the current case, fixation was achieved with 1 screw and a washer following open reduction with an anterior approach. In the current case of isolated fragmented coracoid process fracture showing minimal displacement in a spin bowler cricket player, surgery was preferred as it was thought that nonunion might be encountered particularly because of the effect of forces around the coracoid.
Multicentre, randomized controlled studies would give clearer ideas about the choice of treatment alternatives.
Conclusion
Isolated coracoid fracture is a rare entity causing impairment of upper limb movement. It can be diagnosed more accurately by MRI scan and CT scan. In case of young athletes surgical management may be a good option to achieve early use of the extremity, good radiological union and better clinical function.
Clinical Message
Displaced, isolated fracture of the coracoid can be treated with open reduction and osteosynthesis in young athletes to achieve early use of the extremity, good radiological union and clinical function.
References
1. Petty OH. “Fracture of the coracoid process of the scapula caused bymuscular action,” Annals of Surgery 1907;45(3):427-430 Ogawa K, Yoshida A, Takahashi M, and Ui M. “Fractures of the coracoid process.”. Journal of Bone and Joint Surgery B,1997; 79, (1):17-19.
2. McGinnis M and Denton JR. “Fractures of the Scapula: A Retrospective Study of 40 Fractured Scapulae.Journal of Trauma and Acute Care Surgery. 1989; 29(11):1,” 488-1493. doi:10.1097/00005373-198911000-00006
3. Ogawa K, Inokuchi S and Matsui K. “Fracture of the Coracoid Process.” Acta Orthopaedica Scandinavica.1990; 61, (1):7-8.
4. Eyres KS, Brooks A and Stanley D. “Fractures of the Coracoid Process.” The Journal of Bone and Joint Surgery 1995; 77(3):425-428. .
5. F´ery A, Sommelet J. Fracture of the coracoid process. Rev Chir Orthop Reparatrice Appar Mot 1979;65:403-7.
6. Ada JR and Miller ME. “Scapular fractures: analysis of 113 cases.” Clinical Orthopaedics and Related Research 1991; 269: 174–180.
7. Imatani RJ. “Fractures of the scapula: a review of 53 fractures.” Journal of Trauma 1975;15(6):473-478. .
8. Wilber MC and Evans EB. “Fractures of the scapula. An analysis of forty cases and a review of the literature.” Journal of Bone and Joint Surgery A. 1977;59(3):358-362.
9. Butters KP. “Fractures and dislocations of the scapula.” in Fractures in Adults C. A. Rockwood Jr., D. P. Green, R. W. Bucholz, and J. D. Heckman, Eds., pp. 1163–1164, Lippincott- Raven, Philadephia, Pa, USA, 4th edition, 1996.
10. Vaienti E and Pogliacomi F. “Delayed diagnosis of isolated coracoid process fractures: results of 9 cases treated conservatively.” Acta Biomedica 2012;83(2):138-146.
11. Lal H, Bansal P, Sabharwal VK, Mawia L, and Mittal D. “Recurrent shoulder dislocations secondary to coracoid process fracture: a case report.” Journal of Orthopaedic Surgery 2012;20(1):121-125.
12. Botchu R, Lee K, and Bianchi S. “Radiographically undetected coracoid fractures diagnosed by sonography. Report of seven cases.” Skeletal Radiology 2012;41:(6):693-698.
13. Neer II CS. “Fractures about the shoulder,” in Fractures, C. A. Rockwood and D. P. Green, Eds., pp. 713–721, Lippincott, Philadephia, Pa, USA, 1984.
14. Anavian J, Wijdicks CA, Schroder LK, Vang S, and Cole P. “Surgery for scapula process fractures: good outcome in 26 patients.” Acta Orthopaedica 2009;80(3):344-350.
15. Spormann C, Holzach P, and Ryf C. “Open reduction and internal fixation of isolated fractures of the coracoid-process— presentation of three cases and review of the literature.” Swiss Surgery. 1998;4(4):198-202.
16. Subramanian AS, Khalik MA, and Shah MM. “Isolated fracture of the coracoid process associated with unstable shoulder.” ANZ Journal of Surgery 2007;77(3):188-189.
17. Garcia-Elias M and Salo JM. “Non-union of a fractured coracoid process after dislocation of the shoulder. A case report.” Journal of Bone and Joint Surgery B 1985;67(5):722-723.
18. Guttentag IJ and Rechtine GR. “Fractures of the scapula. A review of the literature.” Orthopaedic Review 1988;17(2):147-158.
19. Goss TP. “The scapula: coracoid, acromial, and avulsion fractures.” American Journal of Orthopedics 1996;25(2):106-115.
20. Bhatia DN. “Orthogonal biplanar fluoroscopy-guided percutaneous fixation of a coracoid base fracture associated with acromioclavicular joint dislocation.” Techniques in Hand and Upper Extremity Surgery 2012;16(1):56-59.
| How to Cite This Article: Archik S, Nanda SN, Tripathi S, Choudhari A, Rajadhyaksha H. An Isolated Displaced Fracture of the Coracoid Process Treated with Open reduction and internal fixation – A Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2016 Jan-Mar;6(1): 37-39. Available from: https://www.jocr.co.in/wp/2016/01/02/2250-0685-372-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


