
[box type=”bio”] What to Learn from this Article?[/box]
Chondroblastic osteosarcoma is a rare cause of spinal stenosis. A proper biopsy technique as well as full preoperative staging workup prior to any surgical procedure involving musculoskeletal tumors is essential.
Case Report | Volume 6 | Issue 1 | JOCR Jan-Mar 2016 | Page 72-75 | Travis Spencer Scudday, Olumide Ayodele Danisa, Lee Michael Zuckerman DOI: 10.13107/jocr.2250-0685.383
Authors: Travis Spencer Scudday[1], Olumide Ayodele Danisa[1], Lee Michael Zuckerman[1]
[1] Department of Orthopaedic Surgery, Loma Linda University Medical Center. Loma Linda, CA, USA.
Address of Correspondence
Dr. Olumide Ayodele Danisa, MD
Department of Orthopaedic Surgery, Loma Linda University Medical Center. 11406 Loma Linda Drive, Suite 218 Loma Linda, CA 92354. T: 909-558-6444. F: 909-558-6118. Email: odanisa@yahoo.com
Abstract
Introduction: Pelvic sarcoma presenting with neurologic symptoms is rare. Workup of neurological deficits, whether elective or emergent should address the possibility of a space occupying lesion including pelvic sarcoma. Poor biopsy technique and incomplete workup of musculoskeletal tumors results in misdiagnosis or major errors in 18% of biopsies. The sequelae of a suboptimal biopsy include local recurrence, a more extensive resection, or extremity amputation. Pelvic chondroblastic osteosarcoma presenting with neurological deficits has not been previously reported. We report two cases of chondroblastic osteosarcoma that were treated with urgent decompression of the lumbar spine due to neurologic symptoms.
Case presentations: Our two cases, a 25 year old Hispanic female and 22 year old Hispanic male, both presented with neurologic changes due to a space occupying tumor in the lumbar spine and pelvis. Both underwent spinal decompression following incomplete workup. A repeat biopsy was required in both cases due to a questionable initial diagnosis. Once the diagnosis was confirmed, they underwent definitive resection and treatment that was more morbid due to the primary decompressions.
Conclusion: We stress the importance of proper biopsy techniques as well as the need to complete a full preoperative staging workup prior to any surgical procedures involving musculoskeletal tumors. We review the current literature on lumbar chondroblastic osteosarcomas and review the issues surrounding biopsy of musculoskeletal tumors. Our cases underline the need for complete workup and correct biopsy techniques to ensure patients have the best chance at tumor free survival with minimal morbidity.
Keywords: Pelvic tumor, tumor biopsy, oncology, tumor spread, chondroblastic osteosarcoma.
Introduction
Primary sarcoma of the pelvis is rare with an incidence of 89 per 100,000 people. Osteosarcoma, chondrosarcoma and Ewing’s sarcoma are the most common primary sarcomas that affect the pelvis. Osteosarcoma and Ewing’s sarcoma occur more often in adolescents and young adults while chondrosarcoma is seen in older adults. Patients often present with a long history of symptoms including lower back pain, groin pain, or hip pain. Late in the disease, pelvic sarcoma may mimic spinal stenosis, lumbar radiculopathy or caudaequina syndrome by mass effect or neurological structure invasion.
Appropriate biopsy techniques of musculoskeletal tumors are vital to the patient’s outcome. The lack of thorough preoperative workup and unfamiliarity with tumor biopsy principles can result in increased patient morbidity and recurrence rates. Sarcoma as a cause of neurologic changes is rare but must be considered prior to continuing with decompression. We present the first cases of neurologic compression caused by a primary pelvic chondroblastic osteosarcoma and discuss the issues associated with prior laminectomies through pelvic sarcoma.
Case Report
Case 1:
A 25-year-old woman presented to an emergency department complaining of a year long history of worsening back pain, 6 months of worsening right leg weakness and 3 months of progressive right foot drop. She denied any bowel or bladder incontinence but did admit to decreased perianal sensation over the previous 3 weeks. A lumbar spine MRI revealed a large sacral mass. She was then transferred to our tertiary care facility where she was evaluated by the Spine service. Physical examination revealed profound right lower extremity weakness in the L5-S1 distribution with absence of deep tendon reflexes. Sensation was decreased in the anterior tibial, plantar and dorsal foot distributions. She had decreased perianal sensation but intact rectal tone.
Imaging
Plain film imaging revealed intact vertebral alignment and no suspicious vertebral deformities. A lytic lesion of the right sacrum however was evident. A lumbar spine MRI with and without contrast demonstrated a large 6 by 8 centimeter multilobulated heterogeneously enhancing mass centered over the right iliac wing that extended into the posterior elements of S1 and the right paraspinal muscles. There was extension into the right S1 and L5 nerve roots and sciatic notch.
Operation
The patient was taken for an urgent decompression without further workup. A midline incision was used for a bilateral L4 to S2 laminectomies, facetectomies and foraminotomies with microscopic assisted epidural tumor resection from the right epidural space. The specimens were sent to pathology and were consistent with a chondrosarcoma. Due to these findings, the musculoskeletal oncologist was consulted for further recommendations.
Postoperative Course
The patient had partial resolution of her numbness but continued to have a dense foot drop. She completed the appropriate malignancy workup which revealed no evidence of metastatic disease. As the imaging and patient’s age were not consistent with a chondrosarcoma she underwent an open biopsy of the right ilium. Her final pathology was consistent with a chondroblastic osteosarcoma. She was discharged and underwent neoadjuvant chemotherapy with plans for a definitive resection after completing chemotherapy.
The patient then underwent repeat staging studies which were negative for metastatic disease. Her pelvic and lumbar spine imaging demonstrated tumor growth in the areas of contamination from the initial surgery. The subsequent procedure required a more extensive resection due to seeding from her index surgery. She underwent a staged procedure with an anterior approach followed by resection from a posterior approach. Her previous posterior midline incision was excised and her paraspinal muscles and spinal cord had to be resected bilaterally at the level of the previous surgery. She underwent a right internal hemipelvectomy, complete sacrectomy, and complete L5 resection, ligation of the thecal sac at the L4-5 level with ligation of the sciatic nerve at the sciatic notch, and L1 to ilium fixation and arthrodesis with morselized allograft and a fibular strut allograft. Coverage of the posterior defect was necessary with a pedicled vertical rectus myocutaneous flap. The initial decompression forced her left sacrum, L5 vertebrae and spinal cord to be resected. Her final pathology demonstrated negative margins with 75% tumor necrosis.
Following the definitive resection, she required three irrigation and debridements for superficial wound breakdown. She also underwent revision of a failed iliac screw with harvest of autograft from the right femur using a Synthes Reamer Irrigator Aspirator as there was no evidence of fusion three months from her initial fusion. She then completed a full course of physical therapy and returned to her home four months following her definitive resection. The patient was able to transfer to a wheelchair at the time of discharge and had evidence of early consolidation of the fusion.She was found to have a deep vein thrombosis in her right iliac vein at nine months after surgery. Twelve months postoperatively, she is without evidence of recurrent or metastatic disease.
Case 2:
A 22-year-old male presented to an outpatient department with lower back pain and bilateral leg pain with associated numbness. He had decreased strength in the S1 distribution on the right and the L5 and S1 distribution on the left. He had decreased sensation in the L5 and S1 distributions bilaterally. He denied any bowel or bladder incontinence. His deep tendon reflexes were intact.
Imaging
An abdomen and pelvic CT scan showed a large left sided destructive sacral lesion with an associated soft tissue mass on the anterior ilium. The left side of S1 and portions of S2 demonstrated tumor involvement. There were no calcifications found in the soft tissue mass. An MRI of the lumbar spine and upper sacrum again showed a large destructive sacral lesion with associated soft tissue mass. CT scans of the chest and head showed no evidence of metastatic disease.
Operation
He was taken for an open L5-S1 bilateral laminectomy, left sided S1 decompression and sacral biopsy. After mild improvement in his numbness and no improvement in his strength he was referred to the musculoskeletal oncologist as an outpatient.
Postoperative Course
Upon evaluation in our outpatient clinic, his physical findings were largely unchanged with a mild improvement in his bilateral leg pain and numbness. His staging studies were completed without evidence of metastatic disease. The pathology from the index biopsy and decompression demonstrated a possible chondrosarcoma versus chondroblastic osteosarcoma. As the treatment options for chondrosarcoma and chondroblastic osteosarcoma are different, a repeat open sacral biopsy was done at our tertiary care facility by the musculoskeletal oncologist. The second biopsy resulted in a definitive diagnosis of chondroblastic osteosarcoma. The patient then underwent neoadjuvant chemotherapy.
Following completion of neoadjuvant chemotherapy, the patient was scheduled for an en bloc resection to obtain negative margins. At the first stage, he underwent an anterior pelvic osteotomy, dissection and mobilization of the right lumbosacral plexus, L5-S1 diskectomy, low anterior resection with end sigmoid colostomy, and harvest of a left vertical rectus abdominismyocutaneous flap. The second stage included an en bloc resection of the sacrum and coccyx, L5 corpectomy, L4 laminectomy, transection of the spinal cord caudal to the right L4 nerve and cranial to the left L4 nerve root. The second stage was stopped after the tumor resection as the patient became coagulopathic. The final stage completed the reconstruction with posterior fusion of L2-L4 to the pelvis with moselized allograft and fibular strut allograft placement and posterior wound closure with the previously harvested rectus flap. Based on initial imaging, he would have required a complete sacrectomy only. His final pathology demonstrated negative margins with 15% necrosis of the tumor.
He underwent three subsequent irrigation and debridement as well as a split thickness skin graft for wound dehiscence. He was then transferred to a nursing facility for long term rehabilitation. Five months following his resection he was found to have both local recurrence and multiple metastatic lung nodules. The patient and his family chose palliative care.
Discussion
Inadequate biopsy of musculoskeletal tumors may lead to major diagnostic errors or a substantial change in the treatment plan. In 1982, Mankin et al. reported an 18% rate of major errors in diagnosis and an 18% rate of alterations of the treatment plan secondary to an inadequate biopsy. Mankin et al. repeated their study in 1996 with no improvement in the rates of inaccurate diagnosis or changes in treatment plan when an inadequate biopsy was performed. The biopsy of musculoskeletal tumors done prior to referral to a specialist is known to be related with worse outcomes. Complications arising from an improper biopsy result in significant changes for the patient and include a higher rate of amputation, more extensive resection, and a higher rate of local recurrence. In our cases, misdiagnosis would have greatly altered the treatment protocols as neoadjuvant chemotherapy improves survival in osteosarcoma but not in chondrosarcoma.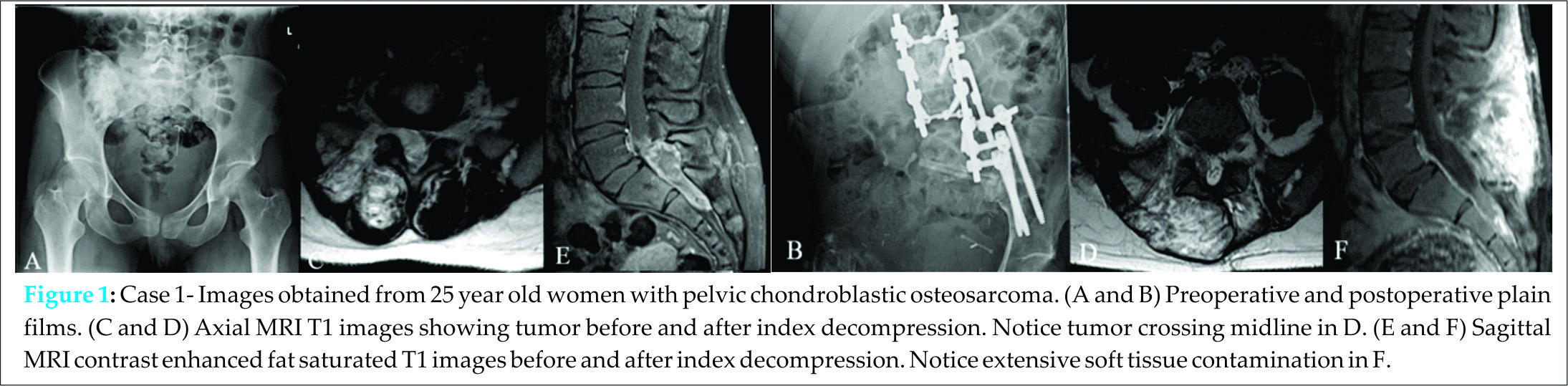
A carefully planned biopsy begins with preoperative staging. Thorough preoperative staging for musculoskeletal tumors includes plain radiography, whole-body technetium-99m-phosphonate bone scintigraphy, CT of the chest, abdomen, pelvis, and the appropriate serum markers for the most common primary malignancies. A systematic preoperative workup will lead to a diagnosis in 85% of cases while a biopsy alone will fail to diagnose the primary tumor in 65% of patients. The biopsy is taken from the most easily accessible lesion. The biopsy tract must not cross tissue planes or compartments. The incision should be placed in line with future approaches enabling resection of the entire biopsy tract. Failure to resect a previous biopsy tract results in local recurrence in up to 38% of tumors. Hemostasis should be ensured and any drains should exit near the incision so they can be easily incorporated into the definitive resection. These principles must be adhered to despite neurologic deficits caused by the tumor as the goal is survival and not palliative decompression.
Osteogenic sarcoma of the spine is rare. Wide resection of osteosarcoma in the extremities improves survival. Classically, using the Weinstein, Boriani, Biagnini (WBB) staging system neural structures are preserved at the cost of a wide tumor free margin. Recently, there has been a trend toward wide resection in osteosarcomas of the spine including resection of the spinal cord if necessary. Talac et al. showed a higher survivorship with lower recurrence rates associated with en bloc resection of spinal sarcomas. Patients with positive margins had a 56% recurrence rate while patients with tumor free margins had a 17% recurrence rate.
Differentiating between the different causes for neural compression is difficult as the patient’s symptoms may be identical in several different diseases. Emergency room consultations for spinal cord or lumbar nerve root compression are common. The possibility of a space occupying malignancy must be discussed when creating a differential diagnosis for a patient with neurologic symptoms. Emergency decompressions may improve clinical symptoms in the short term but will endanger the long term survival and increase the morbidity of the definitive resection. Adhering to proper tumor biopsy principles will give the pathologist the best chance for a definitive diagnosis and will decrease the chances for seeding the tumor.
Conclusion
To our knowledge, these are the first cases of chondroblastic osteosarcoma presenting with predominately neurologic symptoms. Our cases reinforce the need for correct biopsy techniques despite neurological deficits. Sherman et al. have shown late local recurrence for a marginal resection of malignant pelvic tumors to be 40% versus 9% following wide resection. Given our patients’ young age, the optimal chance for recurrence free survival necessitated a wide surgical resection. In our cases, early decompression forced more extensive resection including ligation of the spinal cord and put the patients at a higher risk of recurrence. An R0 resection could be obtained in both cases, but the morbidity of the resection was significantly increased. Coupled with proper preoperative workup and biopsy, modern surgical techniques can expect a high rate of tumor free margins and a five year survival rate of 68% for non-metastatic disease. The biopsy of musculoskeletal tumors is best performed in the tertiary care hospital by the physician who will complete the definitive resection.
Clinical Message
Sarcomas causing neurologic deficits are rare but must be considered in patients with a space occupying lesion. Performing urgent decompression on these patients causes higher morbidity and possibly more mortality than performing a systematic and complete tumor workup despite the delay in surgical intervention.
References
1. Jawad MU, Haleem A A, and Scully S P. Malignant sarcoma of the pelvic bones: treatment outcomes and prognostic factors vary by histopathology. Cancer 2011; 117(7): 1529-41.
2. Wurtz LD, Peabody T D, and Simon M A. Delay in the diagnosis and treatment of primary bone sarcoma of the pelvis. J Bone Joint Surg Am, 1999.81(3): 317-25.
3. Mankin HJ, Mankin C J, and Simon M A. The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996; 78(5): 656-63.
4. PollockRC andStalley P D. Biopsy of musculoskeletal tumours–beware. ANZ J Surg 2004;74(7): 516-9.
5. Bickels J., et al. Biopsy of musculoskeletal tumors. Current concepts. Clin Orthop Relat Res 1999;(368): 212-9.
6. Rougraff BT, Kneisl J S, and Simon M A. Skeletal metastases of unknown origin. A prospective study of a diagnostic strategy. J Bone Joint Surg Am1993;75(9): 1276-81.
7. Schwartz HS and Spengler D M. Needle tract recurrences after closed biopsy for sarcoma: three cases and review of the literature. Ann Surg Oncol 1997;4(3): 228-36.
8. Keynan O et al. Ligation and partial excision of the cauda equina as part of a wide resection of vertebral osteosarcoma: a case report and description of surgical technique. Spine (Phila Pa 1976), 2005;30(4): 97-102.
9. Schoenfeld A.J. et al. Chondrosarcoma of the mobile spine: a review of 21 cases treated at a single center. Spine (Phila Pa 1976) 2012;37(2): 119-26.
10. Boriani, S., J.N. Weinstein, and R. Biagini, Primary bone tumors of the spine. Terminology and surgical staging. Spine (Phila Pa 1976), 1997. 22(9): p. 1036-44.
11. Talac R et al. Relationship between surgical margins and local recurrence in sarcomas of the spine. Clin Orthop Relat Res 2002;(397): 127-32.
12. Shimada Y et al. Clinical features of cauda equina tumors requiring surgical treatment. Tohoku J Exp Med 2006;209(1): 1-6.
13. Sherman CE, O’Connor M I, and Sim F H. Survival, local recurrence, and function after pelvic limb salvage at 23 to 38 years of followup. Clin Orthop Relat Res. 2012;470(3): 712-27.
14. Biau DJ et al., Monitoring the adequacy of surgical margins after resection of bone and soft-tissue sarcoma. Ann Surg Oncol 2013;20(6): 858-64.
15. BiauDJ et al. Using the CUSUM test to control the proportion of inadequate open biopsies of musculoskeletal tumors. Clin Orthop Relat Res 2013;471(3): 905-14.
| How to Cite This Article: Scudday TS, Danisa OA, Zuckerman LM. Management of Pelvic Chondroblastic Osteosarcoma after Urgent Spinal Decompression – A Report of 2 Cases. Journal of Orthopaedic Case Reports 2016 Jan-Mar;6(1): 72-75. Available from: https://www.jocr.co.in/wp/2016/01/02/2250-0685-383-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


