
[box type=”bio”] What to Learn from this Article?[/box]
Polytrauma cases involving ipsilateral mid shaft clavicle, AC joint, shaft humerus and coracoid process are rare but the possibility of each of them must be ruled out in injuries around the shoulder.
Case Report | Volume 6 | Issue 2 | JOCR April-June 2016 | Page 24-27 | Naveen Sharma, Avinash Mandloi, Ashish Agrawal, Shailendra Singh DOI: 10.13107/jocr.2250-0685.414
Authors: Naveen Sharma[1], Avinash Mandloi[1], Ashish Agrawal[1], Shailendra Singh[1]
[1] Department of Orthopaedics, NIMS Medical College, Jaipur. India.
Address of Correspondence
Dr. Avinash Mandloi,
M-292 Nalanda Parisar, Kesarbagh Road, Opp Chameli Devi Public School, Indore (M.P.), 452012. India.
E-mail: Avi_mandloi@yahoo.co.in
Abstract
Introduction: The clavicle, humerus and acromioclavicular (AC) joint separately are very commonly involved in traumatic injuries around the shoulder.
Acromioclavicular joint dislocation with distal clavicle fracture is a well recognized entity in clinical practice. AC joint dislocation with mid shaft clavicle fracture is uncommon and only few cases have been reported in literature.
However, to the best of our knowledge, this is the first case report to describe an acromioclavicular dislocation with ipsilateral mid shaft clavicle, mid shaft humerus and coracoid process fracture. Fractures of the humerus and clavicle along with the acromioclavicular joint dislocation were fixed at the same setting.
Case Report: A 65-year-old male met with a high velocity road traffic accident. Plain radiographs showed displaced mid third clavicle fracture with acromioclavicular joint dislocation with mid shaft humerus fracture. Surgical fixation was planned for humerus with interlocking nail, clavicle with locking plate and acromioclavicular joint with reconstruction of coracoclavicular ligaments. Intraoperatively, coracoid process was found to have a comminuted fracture. The operative plan had to be changed on table as coracoclavicular fixation was not possible. So acromioclavicular joint fixation was done using tension band wiring and the coracoclavicular ligament was repaired using a 2-0 ethibond. The comminuted coracoid fracture was managed conservatively. K wires were removed at 6 weeks. Early mobilization was started.
Conclusion: In acromioclavicular joint injuries, clavicle must be evaluated for any injury. Although it is more commonly associated with distal clavicle fractures, it can be associated with middle third clavicle fractures. As plain radiographs, AP view are most of the times insufficient for viewing integrity of coracoid process, either special views like Stryker notch or CT scan may help in diagnosing such concealed injuries. When associated with fractures of the humerus and clavicle, anatomical restoration of acromioclavicular joint along with anatomical reduction and a rigid fixation of associated fractures is essential. Proper rehabilitation protocol is a must for achieving promising results. In our case, we were able to achieve a stable surgical fixation of both the fractures as well as AC joint, which enabled us to start early joint mobilization and rehabilitation.
Keywords: acromioclavicular joint dislocation, fracture mid shaft clavicle, fracture mid shaft humerus.
Introduction
The clavicle, humerus and acromioclavicular (AC) joint separately are very commonly involved in traumatic injuries around the shoulder. Acromioclavicular joint dislocation with distal clavicle fracture is a well recognized entity in clinical practice [1]. AC joint dislocation with mid shaft clavicle fracture is relatively uncommon and only a few cases have been reported in literature so far [2,3]. However, to the best of our knowledge, this is the first case report to describe an acromioclavicular dislocation with ipsilateral mid shaft clavicle, mid shaft humerus and coracoid process fracture. Fractures of the humerus and clavicle along with the acromioclavicular joint dislocation were fixed at the same setting.
Case Report
A 65-year-old hypertensive male came to the emergency department with swelling and tenderness over left shoulder and left arm following a high velocity road traffic accident. He sustained a direct impact of the shoulder and arm of the left side over the ground. There was no open wound and no neurovascular deficit in the affected upper limb. Initially, a U shaped POP slab with sling was given. Plain radiographs of left shoulder and left arm showed displaced mid third clavicle fracture with acromioclavicular joint dislocation type 3 (Rockwood classification) with mid shaft humerus fracture [Fig. 1, 2, 3]. After complete pre-anaesthetic check up and after obtaining informed consent, surgical fixation was scheduled. First humerus fixation with interlocking nail, followed by clavicle fixation with reconstruction plateand then reconstruction of coracoclavicular ligaments for stabilization of the acromioclavicular joint was planned.
Technique
Patient was induced under general anaesthesia and was positioned in beach chair semi sitting position with sandbag below ipsilateral scapula. Painting and draping of the whole limb and the shoulder girdle was done. First, humerus shaft was fixed by closed intramedullary interlocking nail with proximal and distal locking screws under image guidance. Clavicle was then exposed using a transverse incision, centered over the fracture and along the length of the clavicle. A precontoured 3.5 mm locking plate (7 hole) was applied on the anterosuperior surface of the clavicle and anatomical reduction was achieved. Coracoclavicular ligaments were then exposed for assessment. While doing so, coracoid process was found to be fractured. The fracture pattern was comminuted but undisplaced. The operative plan had to be changed on table, as coracoclavicular ligament reconstruction was not possible. Hence, acromioclavicular joint fixation was done by extending the incision in ‘S’ shaped manner anteriorly, directed towards the acromioclavicular joint. The fibres of deltoid and trapezius were split to expose the joint. At this point, fibres of the torn capsule of the acromioclavicular joint were visible and were removed using a nibbler. Reduction of the joint was achieved and two 1.5 mm smooth Kirschner wires were introduced from the acromion to the lateral third of clavicle transversely, taking care of the inferomedial structures [Fig. 4]. The wires were bent at ninety degrees at the lateral border of acromion and reinforcement was done using a stainless steel wire in figure of eight manner. The torn fibres of the coracoclavicular ligament were sutured using a 2-0 ethibond. The comminuted coracoid fracture was managed conservatively.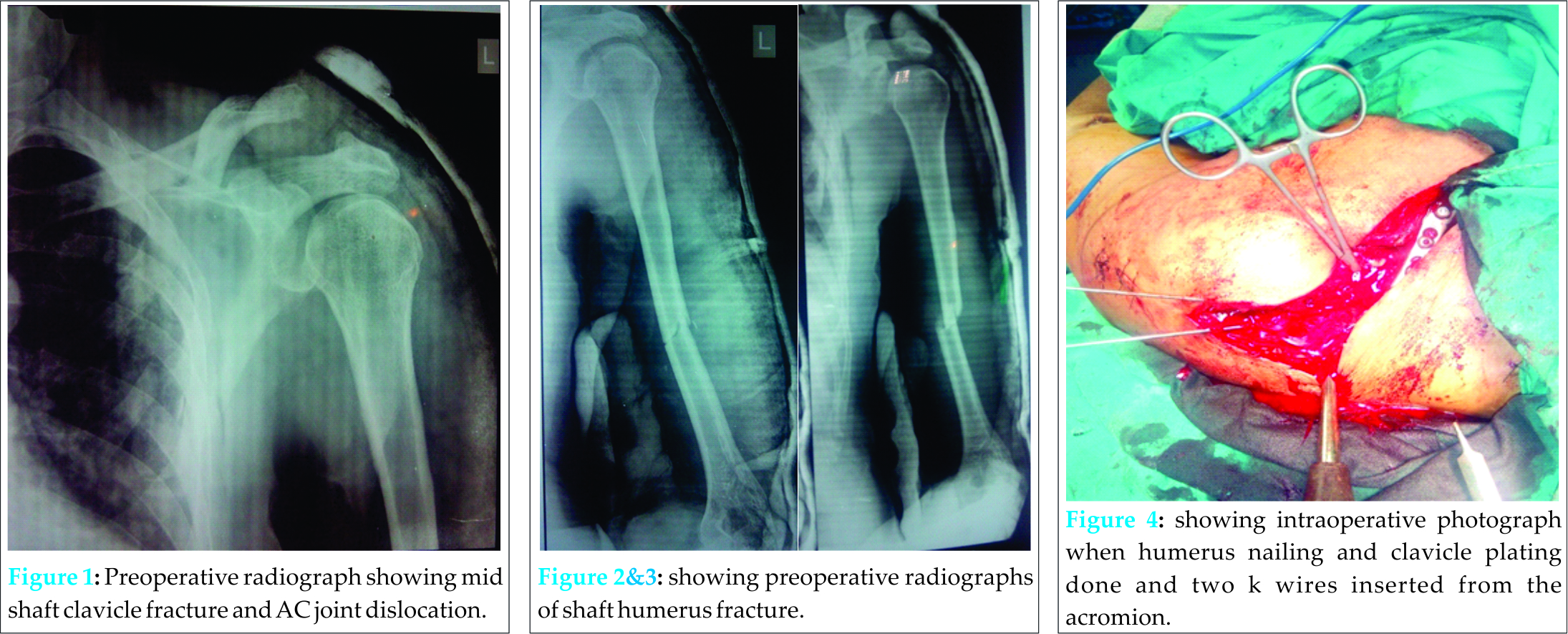
Postoperatively, arm pouch was given and three week immobilization was advised [Fig. 5]. Pendulum exercises were started at three weeks. At six weeks the Kirschners wires were removed and gentle passive range of motion exercises were started followed by active range of motion exercises as per pain tolerance of the patient. At three months, signs of union of humerus and clavicle were seen on radiographs and reduction of the AC joint was maintained with no postoperative complications. Patient was able to resume his daily activities with no tenderness at any fracture sites. At six months, union was radiologically complete [Fig. 6, 7] and patient was able to do180 degrees of forward flexion, 160 degrees of lateral elevation, external rotation of 90 degrees, and internal rotation upto T12 level .Functional assessment as done by Constant and Murley scoring system was found to be 92 at the end of six months.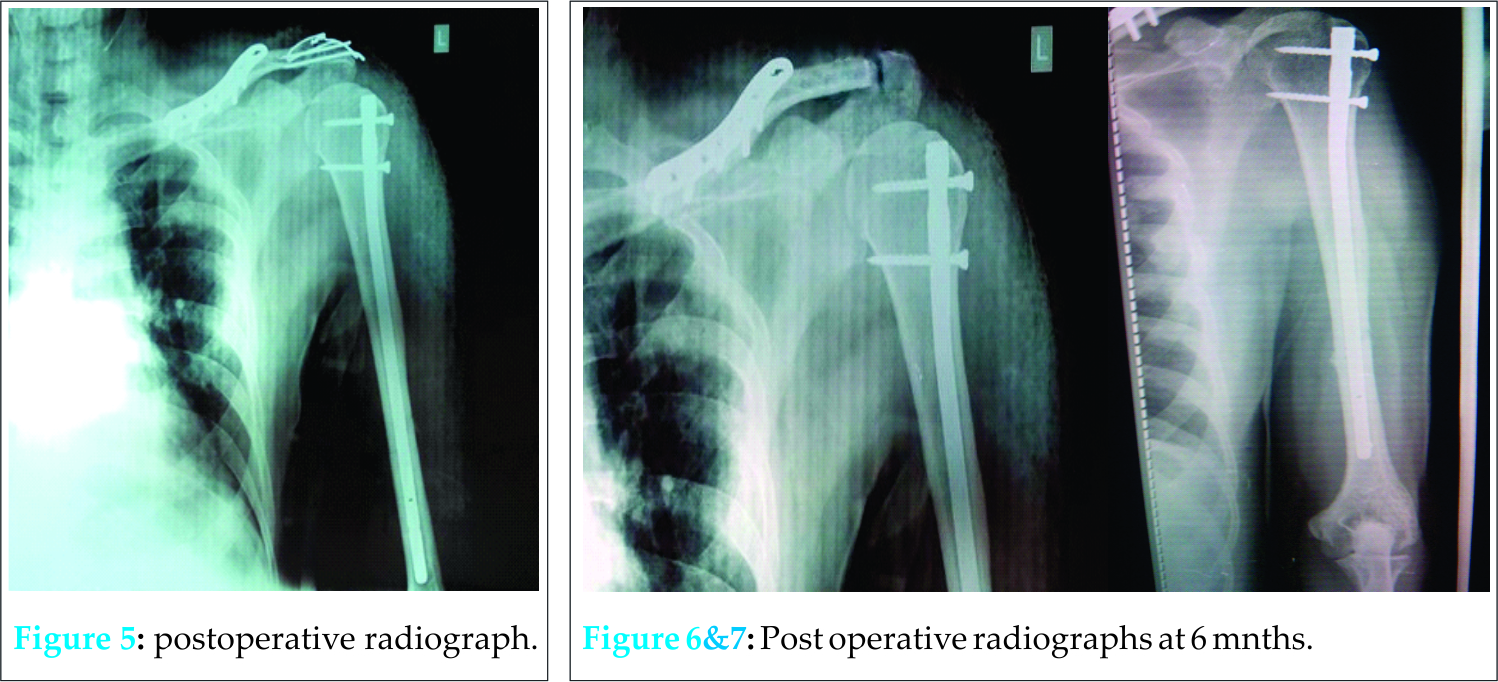
Discussion
The shoulder joint is vulnerable to injuries from sports, falls and other accidents. As the shoulder girdle is subjected to compression force directed from laterally, the main strut maintaining position is the clavicle and its articulations. As the force exceeds the capacity of this structure to withstand it, failure can occur in one of three ways. The acromioclavicular (AC) articulation may fail, the clavicle may break, or the sternoclavicular joint may dislocate [4].The usual mechanism of injury for mid shaft transverse humerus fracture is either bending force with direct blow or fall on outstretched hand. Although enough literature is there to suggest conservative treatment for midshaft clavicle [5], shaft humerus [6], and AC joint dislocation[7], in rare cases like this one where integrity of all the three are disturbed, surgical intervention is better to obtain a stable fixation and early joint mobilization [8,9,10]. Plating is a standard surgical treatment option for displaced mid shaft clavicle fractures which was the chosen option here [11]. For fracture shaft humerus, intramedullary nailing was the preferred option over plating in such a polytrauma case as it entails less surgical dissection, less operative time and minimal blood loss [8]. The operative treatment options for AC joint injuries are intra-articular AC joint fixation, extra-articular coracoclavicular repairs and ligament reconstruction [12]. In rare circumstances like the present one, where there is comminuted fracture of the coracoid process along with AC joint dislocation , intra articular AC joint fixation with coracoclavicular ligament repair was chosen as the preferred option. For AC joint fixation, both Kirschners wires and cortical screws have been used but literature suggests that Kirschners wire are better over cortical screws as screws caused more osteolysis of distal clavicle than pins [13]. For coracoid fractures, both operative and nonoperative methods of treatment have been described. Results seem to be similar in both groups. Therefore, most authors recommend nonoperative treatment for coracoid process fractures [14,15]. Furthermore, as in our case, the coracoid fracture was comminuted, and therefore it was managed conservatively.
Conclusion
In acromioclavicular joint injuries, clavicle must be evaluated for any injury. Although it is more commonly associated with distal clavicle fractures, it can be associated with middle third clavicle fractures. In a case of clavicle fracture with AC joint dislocation, suspicion for coracoid fractures must be there. We recommend ruling out coracoid process fracture in such patients before taking them in theatre to avoid any intraoperative hustle. As plain radiograph, AP view are most of the times insufficient for viewing integrity of coracoid process, either special views like Stryker notch or CT scan may help in diagnosing such concealed injuries. When associated with fractures of the humerus and clavicle, anatomical restoration of acromioclavicular joint along with anatomical reduction and a rigid fixation of associated fractures is essential. Proper rehabilitation protocol is a must for achieving promising results. In our case, we were able to achieve a stable surgical fixation of both the fractures as well as AC joint, which enabled us to start early joint mobilization and rehabilitation.
Clinical Message
Such polytrauma cases involving ipsilateral mid shaft clavicle, AC joint, shaft humerus and coracoid process are rare but the possibility of each of them must be ruled out in injuries around shoulder.
References
1.Neer CS. Fractures of the distal third of the clavicle. Clin Orthop Relat Res. 1968;58:43-50.
2. Wurtz LD, Lyons FA, Rockwood CA. Fracture of the middle third of the clavicle and dislocation of the acromioclavicular joint. A report of four cases. J Bone Joint Surg Am 1992;74:133–7.
3.Yeh PC, Miller SR, Cunningham JG, Sethi PM. Midshaft clavicle fracture and acromioclavicular dislocation: a case report of rare injury. J shoulder Elbow Surg. 2009;18(5):e1-4. doi: 10. 1016/j.jse.2008.09.011
4.Bucholz RW, Heckman JD, Court brown Charles M, Tornetta P. Rockwood and green’s fractures in adults. 7th edition. Philadelphia. Lippincott Williams and Wilkins 2010. Chapter 36:1108
5. Neer CS. Nonunion of the clavicle. JAMA 1960;172:1006-1011.
6.Toivanen JA, Nieminen J, Laine HJ et al. Functional treatment of closed humeral shaft fractures. IntOrthop 2005;29(1):10-13.
7.Schlegel TF, Burks RT, Marcus RL, et al. A prospective evaluation of untreated acute grade III acromioclavicular separations. Am J Sports Med 2001;29(6):699-703.
8.Petsatodes G, Karataglis D, Papadopoulos P, Christoforides J, Gigis J, Pournaras J. Antegrade interlocking nailing of humeral shaft fractures .J Orthop Sci. 2004;9(3):247-52.
9.Gallay SH, Hupel TM, Beaton DE, et al. Functional outcome of acromioclavicular joint injury in polytrauma patients. J Orthop Trauma 1998;12:159-163.
10.Bucholz RW, Heckman JD, Court brown Charles M, Tornetta P. Rockwood and green’s fractures in adults. 7th edition. Philadelphia. Lippincott Williams and Wilkins 2010. Ch 36:1121.
11.Poigenfurst J, Rappold G, Fischer W. Plating of fresh clavicular fractures: results of 122 operations. Injury 1992;23:237-241.
12.Bucholz RW, Heckman JD, Court brown Charles M, Tornetta P. Rockwood and green’s fractures in adults. 7thedition.Philadelphia. Lippincott Williams and Wilkins 2010.ch 39:1226.
13.Eskola A, Vainionpaa S, Korkala O, et al. Acute complete acromioclavicular dislocation. A prospective randomized trial of fixation with smooth or threaded Kirschner wires or cortical screw. Ann ChirGynaecol 1987;76:323-326.
14.Vaienti E, Pogaliacomi F. Delayed diagnosis of isolated coracoid process fractures: results of 9 cases treated conservatively. Acta biomed 2012;83(2):138-46.
15.Ogawa K, Yoshida A, Takahashi M, Ui M. fractures of the coracoid process. J Bone Joint Surg Br.1997;79(1):17-9
| How to Cite This Article: Sharma N, Mandloi A, Agrawal A, Singh S. Acromioclavicular Joint Dislocation with Ipsilateral Mid Third Clavicle, Mid Shaft Humerus and Coracoid Process Fracture – A Case Report. Journal of Orthopaedic Case Reports 2016 April-June;6(2): 24-27. Available from: https://www.jocr.co.in/wp/2016/04/01/2250-0685-414-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


