
[box type=”bio”] What to Learn from this Article?[/box]
The possibility of malignancy must be kept in mind in musculoskeletal masses of patients with hemihyperplasia.
Case Report | Volume 6 | Issue 2 | JOCR April-June 2016 | Page 28-30 | Nihat Demirhan Demirkiran, Olcay Akdeniz, Onur Hapa, Hasan Havıtçıoğlu. DOI: 10.13107/jocr.2250-0685.416
Authors: Nihat Demirhan Demirkiran[1], Olcay Akdeniz[1], Onur Hapa[1], Hasan Havıtçıoğlu[1]
[1] Department of Orthopedics, Dokuz Eylul University Hospital 35340 Balcova, Izmır, Turkey.
Address of Correspondence
Dr. Nihat Demirhan Demirkiran,
Department of Orthopedics, Dokuz Eylul University Hospital 35340 Balcova, Izmır, Turkey.
E-mail: drdemirhandemirkiran@hotmail.com
Abstract
Introduction: Mesenchymal chondrosarcoma is a malignant tumor which originates from chondrogenic tissue. Agressive surgery is considered the major treatment method for the primary disease but there may be unsatisfactory results of surgery depending on location or extension to unresectable sites of majority of mesenchymal chondrosarcomas. Hemihyperplasia, formerly called hemihypertrophy, is a rare congenital overgrowth disorder in which one or more body parts on one side of the body grows more than other, causing asymmetry. Isolated hemihyperplasia is caused by an underlying abnormality of cell proliferation in individuals with neither any other underlying diagnosis nor vascular or skin anomalies. Isolated hemihyperplasia reveals an increased risk of embryonal tumors such as Wilms tumor, adrenal carcinoma or hepatoblastoma. However no such concomitance has been reported with chondrosarcoma. We report the first case of mesenchymal chondrosarcoma presenting with isolated hemihypertrophy.
Case Report: A 64-year-old female presented with a palpable mass in posterolateral aspect of the left lateral malleolus which developed over 5 months. Hemihypertrophy involving the right side of her body was present and the patient had a history of foot shortening operation at adolescent age. Further examination of the patient revealed no vascular or skin anomalies, nor any findings suggesting a syndrome. Isolated hemihyperplasia diagnosis was achieved. After preoperative imaging studies, surgical excision was considered as best treatment option in local musculoskeletal tumor council and marginal resection was performed. The resected mass was sent for histopathological investigation. Immunohistochemical and morphological findings revealed malignant mesenchymal chondrosarcoma.
Conclusion: IH is well known to be associated with increased incidence of some embryonal tumors like Wilms’ tumor, adrenal carcinoma and hepatoblastoma. But no such association has been reported with chondrosarcoma. In musculoskeletal masses of patients with hemihyperplasia, the possibility of malignancy must be kept in mind.
Keywords: chondrosarcoma, hemihyperplasia, mesenchymal tumor.
Introduction
Mesenchymal chondrosarcoma is a malignant tumor which originates from chondrogenic tissue. Agressive surgery is considered the major treatment method for the primary disease but there may be unsatisfactory results of surgery depending on location or extension to unresectable sites of majority of mesenchymal chondrosarcomas. Hemihyperplasia, formerly called hemihypertrophy, is a rare congenital overgrowth disorder in which one or more body parts on one side of the body grows more than other, causing asymmetry. Isolated hemihyperplasia is caused by an underlying abnormality of cell proliferation in individuals with neither any other underlying diagnosis nor vascular or skin anomalies. Isolated hemihyperplasia reveals an increased risk of embryonal tumors such as Wilms tumor, adrenal carcinoma or hepatoblastoma. However no such concomitance has been reported with chondrosarcoma. We report the first case of mesenchymal chondrosarcoma presenting with isolated hemihypertrophy.
Case Report
We report a case of mesenchymal chondrosarcoma arising from the left ankle region of a patient with isolated hemihypertrophy of right side of her body.
A 64-year-old female presented with a palpable mass about 35 x 28 x 30 mm in posterolateral aspect of the left lateral malleolus which developed over 5 months. (Fig 1). Hemihypertrophy involving the right side of her body was present and the patient had a history of foot shortening operation at adolescent age. (Fig 2,3) 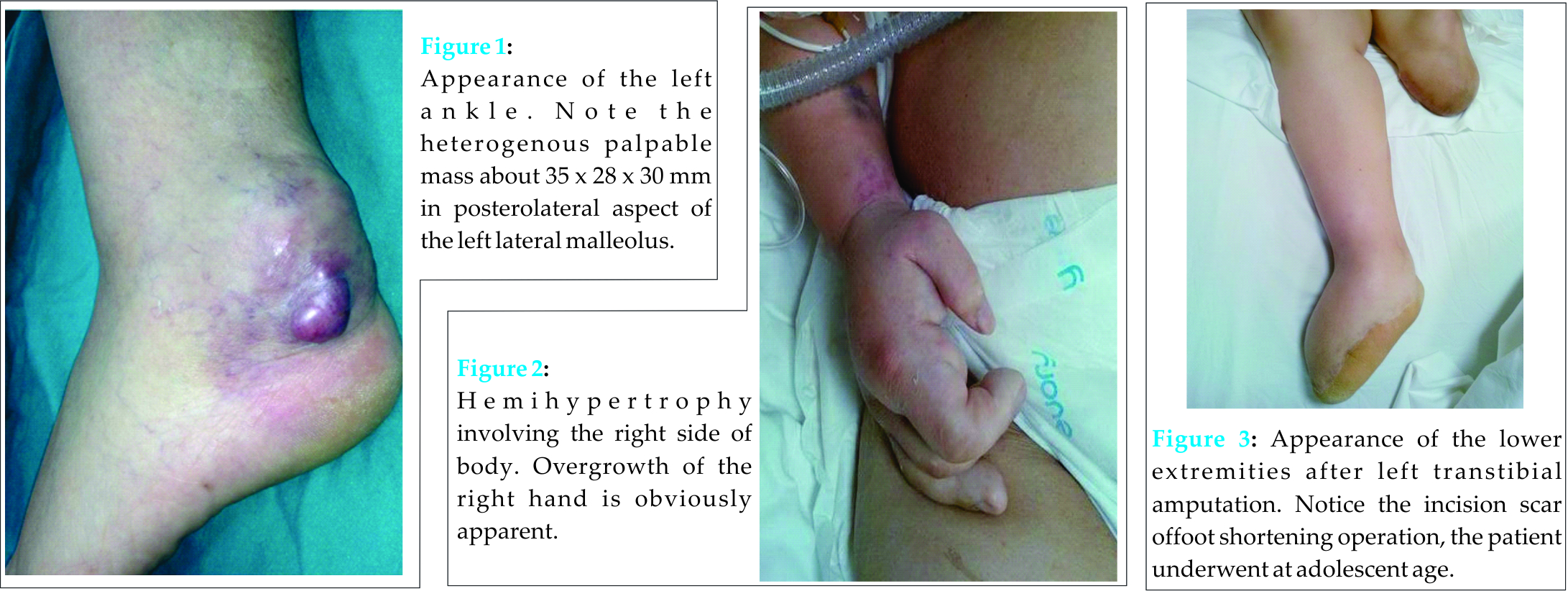 Further examination of the patient revealed no vascular or skin anomalies, nor any findings suggesting a syndrome. Isolated hemihyperplasia diagnosis was achieved. Imaging studies of the left ankle revealed; radiograph of the left ankle region was taken and it showed enlarged soft tissue shadow with large area of stipple calcification within it. From these findings diagnosis of the soft tissue sarcoma with calcification was kept. MRI revealed one heterogeneous hyperintense and hypointense large soft tissue mass lesion (Axial36x31 mm, coronal 36×57 mm sized) in posterior left ankle region in T-2 and T-1 weighted images respectively.It was situated posterior to lateral malleolus adjacent to gastrocnemius muscle, between arteria tibialis posterior and achiles tendon. By contrast with accompanying soft tissue oedema, underlying bone was completely normal. (Fig 4) Surgical excision was considered as best treatment option in local musculoskeletal tumor council and marginal resection was performed. Per-operatively mass and heamatoma was observed.(Fig 5).
Further examination of the patient revealed no vascular or skin anomalies, nor any findings suggesting a syndrome. Isolated hemihyperplasia diagnosis was achieved. Imaging studies of the left ankle revealed; radiograph of the left ankle region was taken and it showed enlarged soft tissue shadow with large area of stipple calcification within it. From these findings diagnosis of the soft tissue sarcoma with calcification was kept. MRI revealed one heterogeneous hyperintense and hypointense large soft tissue mass lesion (Axial36x31 mm, coronal 36×57 mm sized) in posterior left ankle region in T-2 and T-1 weighted images respectively.It was situated posterior to lateral malleolus adjacent to gastrocnemius muscle, between arteria tibialis posterior and achiles tendon. By contrast with accompanying soft tissue oedema, underlying bone was completely normal. (Fig 4) Surgical excision was considered as best treatment option in local musculoskeletal tumor council and marginal resection was performed. Per-operatively mass and heamatoma was observed.(Fig 5). 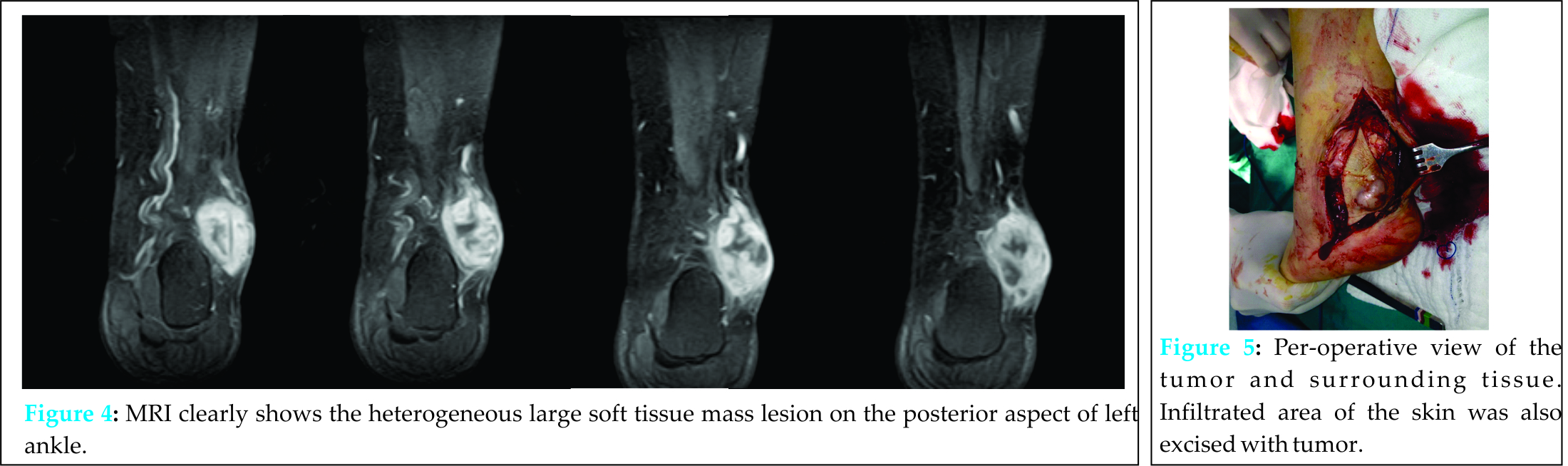 Tumor had no osseos involvement with fibula. After disection of tumor from adjacent tibialis posterior artery and achiles tendon, mass was excised. The resultant defect on achiles tendon was repaired with vicryl sutures. Following bleeding control, skin was closed with a flap from posterior calf. The resected mass was sent for histopathological investigation. Grossly, specimen was gray white colored and solid in consistency, containing local bleeding regions. (Fig 6) Microscopic examination showed immature cartilaginous tissue with osteoclast like giant cells and undifferentiated small round cells. The undifferentiated tumor cells were diffuse stained with Vimentin, CD99, BCL-2 and focally stained with actin. When immunohistochemical and morphological findings were considered together, diagnosis of malignant mesenchymal chondrosarcoma was achieved. Postoperatively the patient was reconsulted with medical and radiation oncology and screening of the abdomen and chest were done which revealed evidence of pulmonary metastases. Chemotherapy was initiated. The patient presented surgical wound problems which turned out to be a local recurrence during chemotherapy. (Fig 7). Amputation of the left lower limb was performed. At last follow-up, the patient had multiple systemic metastases and severe repiratory distress.
Tumor had no osseos involvement with fibula. After disection of tumor from adjacent tibialis posterior artery and achiles tendon, mass was excised. The resultant defect on achiles tendon was repaired with vicryl sutures. Following bleeding control, skin was closed with a flap from posterior calf. The resected mass was sent for histopathological investigation. Grossly, specimen was gray white colored and solid in consistency, containing local bleeding regions. (Fig 6) Microscopic examination showed immature cartilaginous tissue with osteoclast like giant cells and undifferentiated small round cells. The undifferentiated tumor cells were diffuse stained with Vimentin, CD99, BCL-2 and focally stained with actin. When immunohistochemical and morphological findings were considered together, diagnosis of malignant mesenchymal chondrosarcoma was achieved. Postoperatively the patient was reconsulted with medical and radiation oncology and screening of the abdomen and chest were done which revealed evidence of pulmonary metastases. Chemotherapy was initiated. The patient presented surgical wound problems which turned out to be a local recurrence during chemotherapy. (Fig 7). Amputation of the left lower limb was performed. At last follow-up, the patient had multiple systemic metastases and severe repiratory distress.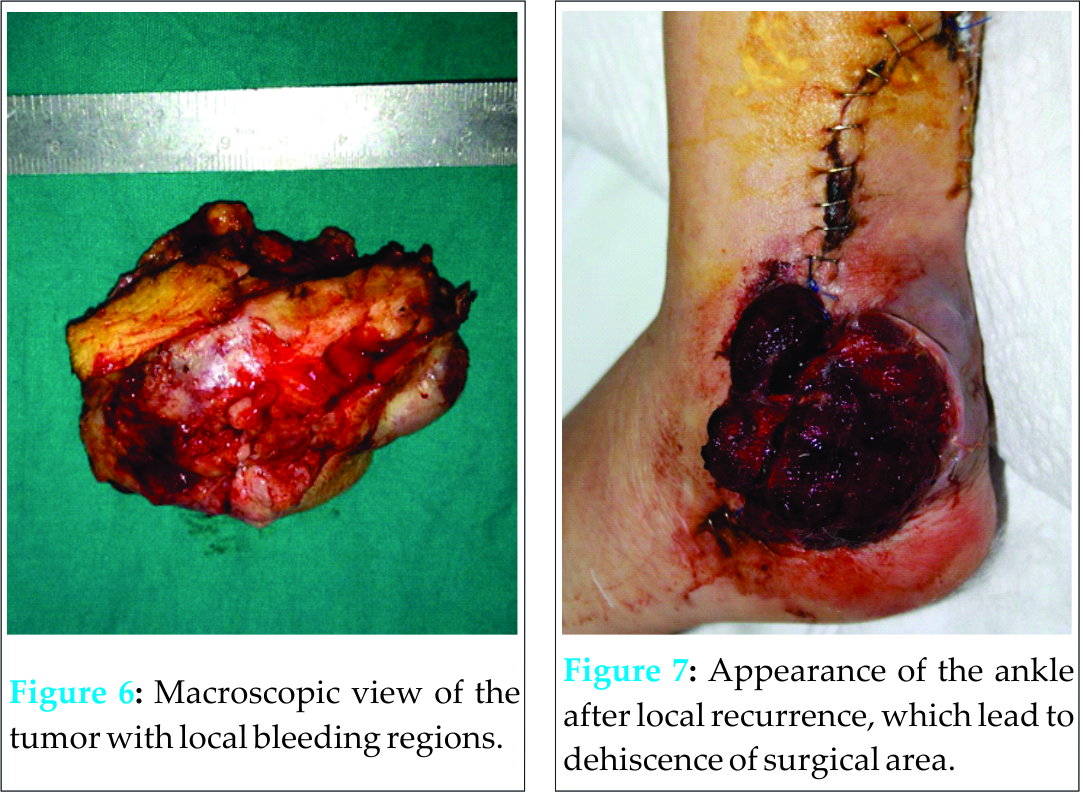
Discussion
Chondrosarcoma is a malignant tumor of chondrogenic origin. [1] Four types of chondrosarcoma have been described: grade I, grade II, mesenchymal and myxoid. [2] The mesenchymal subtype is a rare and the most malignant variant of chondrosarcoma which is related with poor prognosis despite chemotherapy and radiotherapy.[1,3,4,5] With a high incidence of local recurrence and distant metastasis, all cases presenting mesenchymal chondrosarcoma have been reported fatal even after complete surgical excision[6]. The first description of mesenchymal chondrosarcoma (MC) in the literature was reported by Lichtenstein and Bernstein in 1954[7,8]. MC corresponds to less than 1% of all sarcomas and mostly affects children and young adults between the ages of 15 and 35 years [9]. Mesenchymal chondrosarcoma originates from chondrogenic tissue and is characterized by a bimorphic histological appearance, with both undifferentiated mesenchymal tissue and well-differentiated malignant hyaline cartilage.[5, 8] Most cases with MC are treated surgically although there have not been an agreement on a therapeutic standard, due to its very low incidence. [9]. Agressive surgery is considered the major treatment method for the primary disease but there may be unsatisfactory results of surgery depending on location or extension to unresectable sites of majority of mesenchymal chondrosarcomas [1]. Hemihyperplasia, formerly called hemihypertrophy, is a rare congenital overgrowth disorder in which one or more body parts on one side of the body grows more than other, causing asymmetry. [10,11,12]. Hemihyperplasia may present in two forms: isolated or part of a syndrome. There have been several syndromes in which hemihyperplasia has been described, these include: Beckwith-Wiedemann syndrome, Proteus syndrome, Russell-Silver syndrome, Neurofibromatosistype I and Klippel-Trénaunay-Weber syndrome [10,11]. Isolated hemihyperplasia is pragmatically described as asymmetric regional body overgrowth which is obviously apparent “from the end of the bed” , and caused by an underlying abnormality of cell proliferation in individuals without any other underlying diagnosis [12]. Etiology of idiopathic nonsyndromic hemihypertrophy is unclear. There are no widely accepted diagnostic criteria to distinguish IH from normal growth variation. However abscence of vascular or skin anomalies are interpreted in favor of IH as such anomalies are usually associated with the mentioned syndromes. Isolated hemihyperplasia reveals an increased risk of embryonal tumors such as Wilms tumor, adrenal carcinoma or hepatoblastoma[12]. Many prognostic implications and peculiar treatment options may be available for indiviuals with an underlying syndrome. Therefore before the diagnosis of IH is made, all the well known overgrowth syndromes with vascular or skin malformations should be ruled out preferably by a clinical geneticist experienced in the differentiation of IH from other causes of body asymmetry [10,12,13].
Sometimes the asymmetry or overgrowth of one side can be so slight that it isn’t easily recognizable, and this leads to difficulties in determining the prevalence of isolated hemihyperplasia accurately. A study which included both isolated and syndromic forms of hemihyperplasia reported a prevalence of 1 in 13,200 live births [14]. In another larger study [15] 860,000 inpatient records were analysed and a total of 10 cases with congenital asymmetry was found, corresponding to an approximately 1 in 86,000 prevalance for hemihypertrophy. But this study had also limitations like including patients with other congenital abnormalities, such as Beckwith-Wiedemann syndrome. Also 14,430 infants were surveyed in Tokyo, where only one with hemihyperplasia was detected [16]. In our case the patient was diagnosed as hemihyperlasia at adolescent age and had undergone foot shortening operation at that age. Since than the patient was neither called for orthopedics examination follow up nor screened for musculoskeletal tumors. At the age of 64 she presented with a palpable mass in posterolateral aspect of the left lateral malleolus which turned out to be a life threatening malignant tumor.
Conclusion
IH is well known to be associated with increased incidence of some embryonal tumors like Wilms’ tumor, adrenal carcinoma and hepatoblastoma. But no such association has been reported with chondrosarcoma. In musculoskeletal masses of patients with hemihyperplasia, the possibility of malignancy must be kept in mind.
Clinical Message
It is reported that IH can coexist with embryonal tumors. However such a coexistence was not reported with chondrosarcoma until present case report. Chondrosarcoma is regarded to have different treatment and prognosis compared to embryonal tumors.
References
1. Harwood AR, Krajbich JI, Fornasier VL. Mesenchymal chondrosarcoma: a report of 17 cases. Clin Orthop Relat Res. 1981 Jul-Aug;(158):144-8.
2. El Mostarchid AB, Belhachmi A, Khaddar A, Gazzaz M, Boucetta M. Spheno-orbital mesenchymal chondrosarcoma: A rare cause of exophthalmos. Pan Arab J Neurosurg. 2010;14(1):86-89.
3. Louvet C, de Gramant A, Krulik KM, Jagueux M, Hubert D, Brissaud P, Sirinelli A, Augerau B, Tubiana JM, Debray J: Extraskeletal mesenchymal chondrosarcoma: case report and review of the literature. J Clin Oncol, 3: 858-863, 1985.
4. Chiang CJ, Fong YC, Hsu HC: Extraskeletal mesenchymal chondrosarcoma. J Chin Med Assoc, 66: 307-310, 2003.
5. Anna Rossetto, Enrico Saccomano, Aron Zompicchiatti, Claudio Avellini, Silvia Toffoli, Gianmaria Miolo, Sergio Frustaci, Alessandro Uzzau . Mesenchymalchondrosarcoma of the spleen: report of a case. Tumori 97: 4. Jul/Aug
6. Chiang CJ1, Fong YC, Hsu HC. Extraskeletal mesenchymal chondrosarcoma. J Chin Med Assoc. 2003 May;66(5):307-10.
7. Bernstein M, Perrin RG, Platts ME, Simpson WJ. Radiation induced cerebellar chondrosarcoma. Case report. J Neurosurg. 1984 Jul;61(1):174-7
8. Dang Vu Nguyen, Ahmad Sobri Muda, Yazmin Yaacob Mesenchymal Chondrosarcoma: A Case Report Malays J Med Sci. May 2013; 20(3): 71–77.
9. Huvos AG, Rosen G, Dabska M, Marcove RC: Mesenchymal chondrosarcoma: A clinicopathologic analysis of 35 patients with emphasis on treatment. Cancer, 51: 1230-1237, 1983.
10. Ballock RT, Wiesner GL, Myers MT, Thompson GH: Hemihypertrophy.Concepts and controversies. J Bone Joint Surg Am 1997,79(11):1731-8.
11. Hoyme HE, Seaver LH, Jones KL, Procopio F, Crooks W, Feingold M: Isolated hemihyperplasia (hemihypertrophy): report of aprospective multicenter study of the incidence of neoplasiaand review. Am J Med Genet 1998, 79(4):274-8.
12. Carol L. Clericuzio, MD, Rick A. Martin, MD. Diagnostic criteria and tumor screening for individuals with isolated hemihyperplasia. Genet Med. Mar 2009; 11(3): 220 -222.
13. Heilstedt HA, Bacino CA. A case of familial isolated hemihyperplasia. BMC Med Genet. 2004 Feb 2;5:1.
14. Leck I, Record RG, McKeown T, Edwards JH: The incidence of malformations in Birmingham, England, 1950–1959. Teratology1968, 1(3):263-80.
15. Parker DASkalko RG: Congenital asymmetry: report of 10cases with associated developmental abnormalities. Pediatrics 1969, 44(4):584-9.
16. Higurashi M, Iijima K, Sugimoto Y, Ishikawa N, Hoshina H, Watanabe N, Yoneyama K: The birth prevalence of malformation syndromes in Tokyo infants: a survey of 14,430 newborn infants.Am J Med Genet 1980,6(3):189-94.
| How to Cite This Article: Demirkiran ND, Akdeniz O, Hapa O, Havitçioglu H. Coexistence of Extraskeletal Mesenchymal Chondrosarcoma and Isolated Hemihyperplasia: A Case Report. Journal of Orthopaedic Case Reports 2016 April-June;6(2): 28-30. Available from: https://www.jocr.co.in/wp/2016/04/01/2250-0685-416-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


