
[box type=”bio”] What to Learn from this Article?[/box]
Total knee arthroplasty in elderly patients with history of diabetes, and multiple steroid injections can lead to a complication of patellar tendon rupture. Timely recognition and primary repair with augmentation is prudent to manage this situation.
Case Report | Volume 6 | Issue 2 | JOCR April-June 2016 | Page 75-77 | Amyn Rajani, Kumar Kaushik Dash, Neetin P Mahajan, Ritesh Kumar. DOI: 10.13107/jocr.2250-0685.444
Authors: Amyn Rajani[1], Kumar Kaushik Dash[1], Neetin P Mahajan[1], Ritesh Kumar[2]
[1]Department of Orthopaedic Surgery, 2nd Floor, Grant Government Medical College & Sir JJ Group of Hospitals, Byculla, Mumbai. India.
[2]Department of Orthopaedics, Hindurao Hospital and NDMC Medical College, Delhi. India.
Address of Correspondence
Dr. Kumar Kaushik Dash,
Assistant Professor, Department of Orthopaedics, Grant Government Medical College & Sir J.J. Group of Hospitals, Byculla, Mumbai. India.
E-mail: kaushikkem@gmail.com
Abstract
Introduction: Patellar tendon rupture can occur due to multiple causes ranging from inflammatory pathologies to episodes of trauma. Extensor mechanism rupture is a rare complication of total knee arthroplasty (TKA). In most of these cases, the failure occurs as avulsion of patellar tendon from tibial tuberosity. We report a rare case with bilateral mid-substance patellar tendon rupture one month after bilateral total knee arthroplasty.
Case Presentation: A 69-year-old male was operated for bilateral grade 4 osteoarthritis. On day 30 post-operative, he sustained bilateral patellar tendon rupture while getting up from toilet. He had a history of multiple steroid injections in the knee, which could have affected the tendon. The other etiologies could be inherent weakness of tendon due to diabetes and old age and micro-trauma/stretch associated with sudden correction of previous deformity by TKA. The management in our case was done by primary repair along with augmentation by autologous semitendinosus graft and suture anchor.
Conclusion: The operating surgeon must be aware of the possibility of patellar tendon rupture following total knee arthroplasty. This will help the surgeon in early recognition and preparedness to handle such complications, should they arise. Surgeons may consider advising caution to both patient and rehabilitation team in cases with old age, chronic diabetes mellitus, and with a history of steroid injections.
Keywords: Total Knee Arthroplasty, Extensor Mechanism, Patellar Tendon Rupture.
Introduction
In advanced osteoarthritis of knee with unremitting pain, total knee arthroplasty (TKA) is the procedure of choice. Disruption of extensor mechanism is a rare and devastating complication of TKA. Extensor mechanism consists of quadriceps muscles, patella, patellar retinaculum, adjacent soft tissues, patellar tendon, and tibial tubercle [1]. Failure usually occurs in one of the three places – quadriceps tendon,p fracture or patellar tendon. The incidence of patellar tendon rupture in total knee arthroplasty is very low (<1%) [2, 3]. In most of these cases, patellar tendon fails at tibial tubercle (avulsion). We present a case with bilateral, spontaneous, mid-substance patellar tendon rupture following bilateral total knee arthroplasty.
Case Report
A 69-year-old male underwent bilateral sequential knee arthroplasty with patellar resurfacing for grade 4 osteoarthritis with bilateral fixed flexion feformity of 30-40 degrees. He was also diabetic and had cardiac ejection fraction of only 20%. Surgery was uneventful with good post-operative recovery. He had normal patellar position on post operative radiographs (Fig. 1). Post TKA, rehabilitation protocols were initiated and he was able to achieve limited indoor ambulation within three days. He continued with range of motion and strengthening exercises along with proprioceptive training. Surgical drains were removed on the 2nd post-operative day and he was discharged on 7th post-operative day. By this time, his range of motion (ROM) was more than 90 degrees and muscle strength in quadriceps was MRC grade 4/5. On 30th post operative day, he experienced buckling and excruciating pain in both knees while getting up from a low lying toilet chair and he was unable to stand. He could not extend his knees, which were swollen. He required assistance from family member for mobility. After that incident, he was unable to walk without support due to severe pain and the knees giving way on weight bearing. He sought medical advice after 2 days when the pain and swelling did not improve. On enquiry, there was history of three intraarticular steroid injections within a period of one-year. This was two years before the patient presented to us for knee arthroplasty. Upon examination, both knee joint were warm, tender and swollen. Swelling and skin discolouration were suggestive of hematoma formation. He was unable to actively extend his knee joint and the range of motion was painful. The patella was mobile and high riding on clinical examination. X-ray of the knee joint revealed patella alta (Fig. 2 and Fig. 3) while rest of the joint was normal. MRI of the both knee was done and it revealed bilateral patella midsubstance tendon rupture. Bilateral patellar tendons were repaired with augmentation by semitendinosus graft and anchors over tibial tuberosity (Fig. 4-6 ).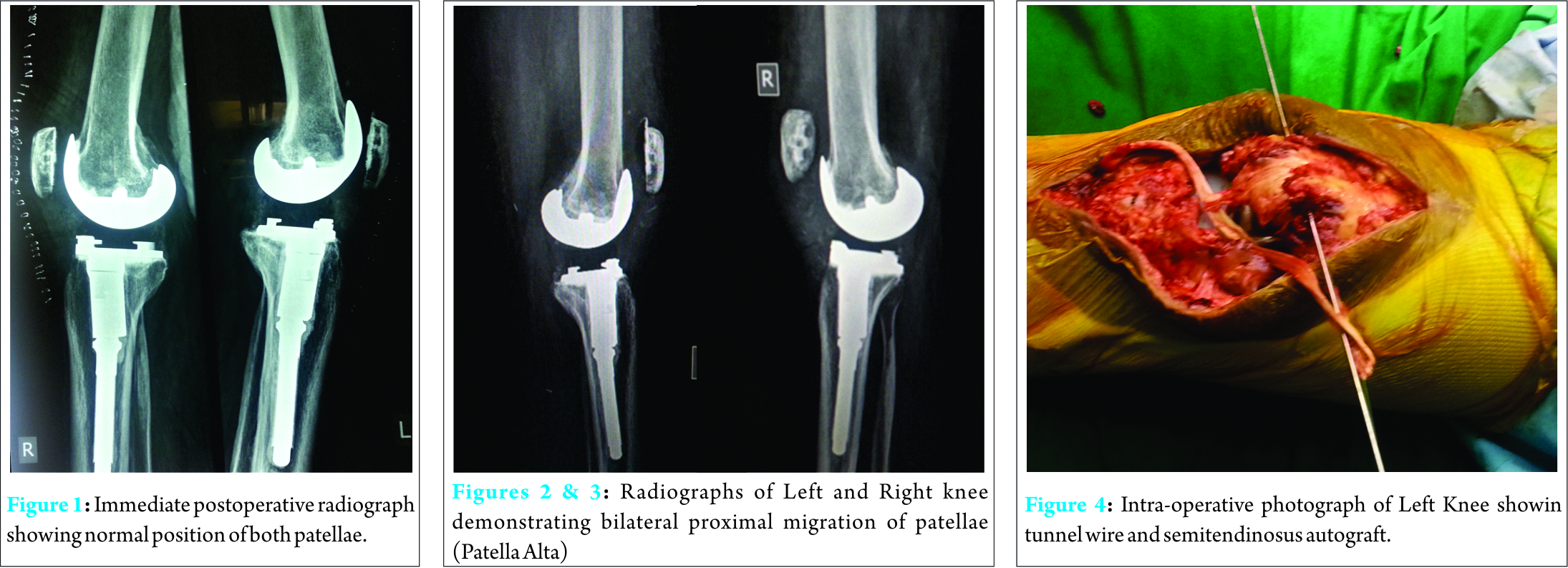 After repair, knee was immobilised in extension for 6 weeks, followed by subsequent mobilisation and rehabilitation. Within 2 weeks of mobilisation, patient was able to achieve ROM upto 60 degree,grade 4/5 (MRC) power in quadriceps and extensor mechanism. There was no extensor lag. At 12 weeks of follow up, patient was able to walk independently with cane and achieved range of motion of 0 – 110 degrees. At 2-years follow-up at present, patient walks without support and has no activity limitations.
After repair, knee was immobilised in extension for 6 weeks, followed by subsequent mobilisation and rehabilitation. Within 2 weeks of mobilisation, patient was able to achieve ROM upto 60 degree,grade 4/5 (MRC) power in quadriceps and extensor mechanism. There was no extensor lag. At 12 weeks of follow up, patient was able to walk independently with cane and achieved range of motion of 0 – 110 degrees. At 2-years follow-up at present, patient walks without support and has no activity limitations.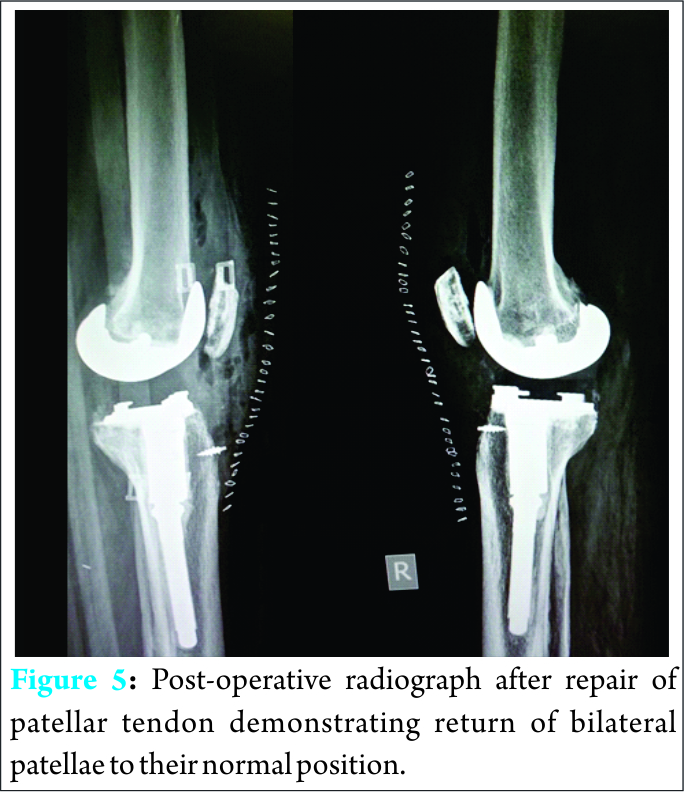
Discussion
Extensor mechanism disruption from quadriceps tendon rupture, patellar fracture, or patellar tendon rupture is an uncommon complication of TKR. It can cause significant functional limitations for a successful joint arthroplasty. The reported incidence of patellar ligament rupture is 0.22-0.55% [4]. Patellar tendon rupture can be due to improper surgical technique resulting in compromised blood supply to the tendon during surgery, micro trauma during surgery, increased stretch for good exposure, damage to the pad of fat or poor joint alignment [5]. It may also be due to inherent weakness of the tendon or damage to the tendon during or after surgery. Sudden jerky movements of the knee especially in the squatting position can also cause tremendous load on quadriceps leading to rupture of the patellar tendon. Cadambi and Engh [6] reported in their case series that six out of seven ruptures occurred intra operatively or immediately afterwards. While Gustillo and Thompson found patellar tendon ruptures to occur later [7, 8]. The possible cause of patellar tendon rupture in our case could be attributed to the many possible causes; namely, (a) inherent weakness of the tendon due to old age, (b) frequent intrarticular steroid injection, and (c) microtrauma and increased stretch associated with abrupt correction of severe varus and flexion deformity by total knee arthroplasty. Finally the sudden jerky movement to get up from a low lying toilet chair leading to violent contraction of quadriceps might have been the main reason for the subsequent rupture. The management of patellar tendon rupture is difficult and the prognosis is not good. Primary repair is successful in the early cases but grafting is required in late and complicated cases. Semitendinosis and Achilles tendon allograft are commonly used. For partial tears, cast immobilization and the use of brace is the treatment of choice. Reconstruction options include direct surgical repair, local autologous graft, distant autologous graft, synthetic graft, or various types of allograft [9]. The management depends upon the level of the rupture. Patellar pole rupture and mid substance tears are treated with simple tension band suturing and immobilization while tibial tuberosity avulsions are pinned with screw. Calcaneal and Achilles tendon grafts are used in some cases [6]. Cadambi and Engh [6] used the semitendinosus tendon. In two of their seven patients, the repair was augmented by using the gracilis tendon and passing it through the patella drill hole. Knee range of motion was restored in all patients. Extensor mechanism allograft was used by Emerson in a series of 15 patients with a rupture of the patella tendon in association with a total knee arthroplasty [10]. The allograft consisted of the tibial tubercle, patellar tendon, patella, and quadriceps tendon that were freeze dried or fresh frozen. The graft was secured to the tibia with distally and quadriceps tendon proximally. Zanotti et al. [10] have reported successful treatment of a patellar tendon-deficient knee in a single patient with the use of a bone-patellar tendon-bone allograft. They used an irradiated, freeze-dried patellartendon-proximal tibial allograft from a fresh cadaver. The repair was protected postoperatively in a cast for 3 months, and progressed to ambulation with a knee ankle foot orthosis. They reported the graft to be healed with full active extension at 2-years follow-up. An alternative surgical technique of reconstruction of the patellar tendon using a semitendinosus gracilis (STG) graft with an interference screw and a staple fixation enabling an immediate mobilization was described by Järvelä in a case report [11]. Recently, use of synthetic mesh to reconstruct a disrupted patellar tendon after TKR was successfully reported. Patients had significant improvement in the mean Knee Society scores for pain and function and the synthetic mesh was significantly less expensive than the allograft [12]. In our case, repair with semitendonosus graft with suture anchors was chosen due to the level and extent of tendon rupture along with surgeon’s preference and expertise in the procedure. In old patients with already weak and compromised musculoskeletal system, great care should be taken in the immediate post operative period to avoid extreme stress on the tendon and joints, aggressive physiotherapy should be avoided and post operative mobility protocols should be tailored to the age and fitness level of the patient to prevent tendon rupture.
Conclusion
Although rare, patellar tendon rupture is a devastating complication following total knee arthroplasty. Awareness and timely recognition is crucial to appropriate management. In situations with poor tendon quality, augmentation of repair with semitendinosus autograft provides good result. Surgeons may consider advising caution to both patient and rehabilitation team in cases with old age, chronic diabetes mellitus, and history of steroid injections.
Clinical Message
Arthroplasty surgeon must be aware of possibility of patellar tendon rupture following total knee arthroplasty. This will help the surgeon in early recognition and preparedness to handle such complications, should they arise.
References
1. Nam D, The Management of Extensor Mechanism Complications in Total Knee Arthroplasty J Bone Joint Surg Am. 2014;96:e47(1-9)
2. Parker DA, Dunbar MJ, Rorabeck CH. Extensor mechanism failure associated with total knee arthroplasty: prevention and management. J Am Acad Orthop Surg. 2003;11(4):238-47.
3. Mont MA, Yoon TR, Krackow KA, Hungerford DS. Eliminating patellofemoral complications in total knee arthroplasty: clinical and radiographic results of 121 consecutive cases using the Duracon system. J Arthroplasty. 1999;14(4):446-55.
4. Hsu RW. The management of the patella in total knee arthroplasty. Chang Gung Med J 2006;29:448-457.
5. Rand JA, Morrey BF, Bryan RS.Patellar tendon rupture after total knee arthroplasty. Clin Orthop Relat Res 1989;244:233-238.
6. Cadambi A, Engh GAUse of a semitendinosus tendon autogenous graft for rupture of the patellar ligament after total knee arthroplasty. A report of seven cases. J Bone Joint Surg Am 1992;74:974-979.
7. Gustillo RB, Thompson R.Quadriceps and patellar tendon ruptures following total knee arthroplasty. Total Arthroplasty of the Knee. Rockville, Maryland 1938;41-47.
8. Emerson RH, Head WC, Malinin TI. Reconstruction of patellar tendon rupture after total knee arthroplasty with an extensor mechanism allograft. Clin Orthop Relat Res 1990;154-161.
9. Crossett LS, Sinha RK, Sechriest VF, Rubash HE.Reconstruction of a ruptured patellar tendon with achilles tendon allograft following total knee arthroplasty. J Bone Joint Surg Am. 2002 Aug;84-A(8):1354-61.
10. Zanotti RM, Freiberg AA, Matthews LS.Use of patellar allograft to reconstruct a patellar tendon-deficient knee after total joint arthroplasty. J Arthroplasty 1995;10:271-274.
11. Järvelä T, Halonen P, Järvelä K, Moilanen T.Reconstruction of ruptured patellar tendon after total knee arthroplasty: a case report and a description of an alternative fixation method. Knee 2005;12:139-143.
12. Browne JA, Hanssen AD. Reconstruction of patellar tendon disruption after total knee arthroplasty: results of a new technique utilizing synthetic mesh. J Bone Joint Surg Am 2011;93:1137-1143.
| How to Cite This Article: Dash KK, Rajani A, Mahajan NP, Kumar R. Bilateral Spontaneous Midsubstance Patellar Tendon Rupture after Bilateral Total Knee Arthroplasty. Journal of Orthopaedic Case Reports 2016 April – June;6(2): 75-77. Available from: https://www.jocr.co.in/wp/2016/04/01/2250-0685-444-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


