
[box type=”bio”] What to Learn from this Article?[/box]
Careful pre and post operative assessment is important in identifying such a rare and life threatening complication, which allows treating them early and preventing any morbidity or even mortality.
Case Report | Volume 6 | Issue 2 | JOCR April-June 2016 | Page 100-102 | Bayan Ghalimah1, Amre Hamdi1. DOI: 10.13107/jocr.2250-0685.460
Authors: Bayan Ghalimah[1], Amre Hamdi[1]
[1] Department Of Orthopaedic, King Abdulaziz University. Jeddah. Saudi Arabia.
Address of Correspondence
Dr. Bayan Ghalimah,
Teaching Assistant, Orthopaedic Surgery Department, King Abdulaziz University, P.O box 140325, Jeddah 21333.
E-mail: bayantash.bt@gmail.com
Abstract
Introduction: Infection poses a substantial challenge after joint replacement.
Case Presentation: We report a 53-year-old female with multiple co-morbidities, who underwent unilateral total knee arthroplasty. Her post-operative course was complicated by acute cholecystitis necessitating cholecystectomy.
Conclusion: In patients who require joint replacement surgery, careful and detailed preoperative assessment is important to identify those at risk for this complication in order to provide timely treatment.
Keywords: Acute cholecystitis infection, total knee replacement, total hip replacement, joint replacement, postoperative complication.
Introduction
Acute cholecystitis is an important post-operative complication and is considered a surgical emergency [1]. Although not uncommon, it is relatively unknown to orthopedic surgeons and only a few cases have been reported in the orthopedic literature. Postoperative cholecystitis should be promptly recognized because it is a life-threatening complication [2], with mortality ranging from 10% to 50% [3]. The development of right upper quadrant abdominal pain associated with fever, tachycardia, and signs of peritoneal irritation after any major orthopedic procedures like: arthroplasty, spinal fusions and others should alert the surgeon to the possibility of postoperative cholecystitis [2]. Cholecystectomy is the treatment of choice considering the high incidence of gangrene and perforation of the gallbladder [2]. Here, we present a patient who underwent unilateral total knee arthroplasty and subsequently developed acute cholecystitis, necessitating urgent surgical intervention.
Case Presentation
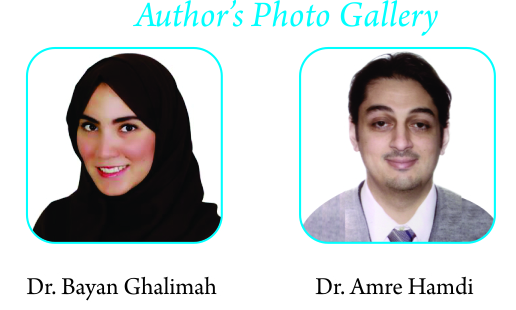
This is a 53-year-old woman with a history of hypertension, hypothyroidism, and hypercholesterolemia. She presented to the orthopedic outpatient department complaining of chronic progressive bilateral knee pain for more than ten years. The pain was worse on the right side. This pain was relieved by daily analgesics and aggravated by activity. There was no evidence of neurological, gastrointestinal, immunological, or hematological dysfunction, or underlying malignancy on systematic review. Her surgical history was remarkable as she had undergone two cesarean sections, tonsillectomy, colonoscopy, and a gastric bypass surgery. General physical examination showed her body mass index as 33.2 kg/m2 , weight as 84 kg and her height was 160 cm. Further examination showed a mild varus deformity of both knees, with no flexion contracture. Her gait was normal and no varus thrust was noted. The active and passive range of motion of her right knee was from 0 to 100 degrees and her ligamentous exam was stable. Radiological studies demonstrated bilateral tricompartmental osteoarthritis (Fig. 1). Routine preoperative laboratory tests, including complete blood count, electrolytes, and coagulation profile were normal. The patient underwent uncomplicated elective right total knee replacement (TKR) (Fig. 2), which was performed under epidural anesthesia. The perioperative antibiotic regimen included administration of 1 g of intravenous cefazolin before incision and 1 g continued every eight hours over the next 24 hours. Postoperative medications, in addition to the antibiotics included analgesics, an anticoagulant, and her regular medications. The patient was started on a liquid diet four hours postoperatively and, because of her poor appetite, she continued on a soft diet for one week before resuming with solid food. From the second postoperative day, she started complaining of an intermittent mild right lower quadrant back pain which was radiating to her right flank. This pain was relieved by analgesics. Her postoperative physiotherapy progressed uneventfully. She was discharged on the sixth postoperative day. On day 13 postoperatively, the patient complained of severe colicky right upper quadrant pain that radiated to the back. It was associated with fever, nausea, and vomiting. The pain was not relieved by conservative treatment. The patient reported no history of a similar attack previously or gallbladder disease. The patient was admitted to the hospital through the emergency department and her examination showed that she was febrile, with no knee findings, and her laboratory investigations yielded these results: white blood cell (WBC) count 16.19 ×109/L (reference range 4.5–11×109/L); total bilirubin 22 µmol/L (reference range 3–17 µmol/L); direct bilirubin 12 µmol/L (reference range 0–5 µmol/L); albumin 23 g/L (reference range 35–50 g/L); total protein 61 g/L (reference range 60–80 g/L); aspartate aminotransferase 12 IU/L (reference range 3–30 IU/L); ALP 120 IU/L (reference range 50–163 IU/L);and amylase 8 IU/L (reference range 25–115 IU/L) while other liver enzymes were within normal ranges. An abdominal ultrasound was consistent with an acute cholecystitis. Her gallbladder was markedly distended, with a thick and edematous wall measuring 1.15 cm. Ultrasound also showed two mobile stones, with the largest measuring 0.9 cm. The common bile duct (CBD) was dilated and measured 0.7 cm, with a thickened wall. The patient underwent laparoscopic cholecystectomy and her intraoperative findings revealed an acute gangrenous gallbladder and suppuration in the abdomen; which necessitated a drain insertion. The infectious disease team was consulted immediately after admission, and they started her on intravenous piperacillin/tazobactam 4,500 mg every six hours, which had to be maintained for seven days until culture results were available, the drain was clear, and no collection was identified by ultrasound. Cultures were positive for gram-positive cocci and gram-negative bacilli (Enterococcus species, extended spectrum beta-lactamase-producing Enterobacteriaceae, and Escherichia coli), and piperacillin/tazobactam was consequently substituted for intravenous imipenem 500 mg every six hours plus intravenous ampicillin 500 mg every six hours based on the sensitivity results. The drain was removed on the second postoperative day, as it only had a small amount of serous fluid.
On the fourth postoperative day, the patient started complaining of generalized abdominal pain, which was associated with an increase in WBC. Computed tomography (CT) of the abdomen and pelvis was done to rule out intestinal obstruction, and it showed no signs of intestinal perforation, no leak of oral contrast or collection. On day 10 post-op, the patient was discharged on oral antibiotics (oral ciprofloxacin 500 mg every eight hours for seven days). She was followed in the outpatient clinic after discharge and, on her last visit to the clinic (four weeks post-laparoscopic cholecystectomy), she was free of abdominal symptoms. The patient did not have any new complaints in regard to her TKR.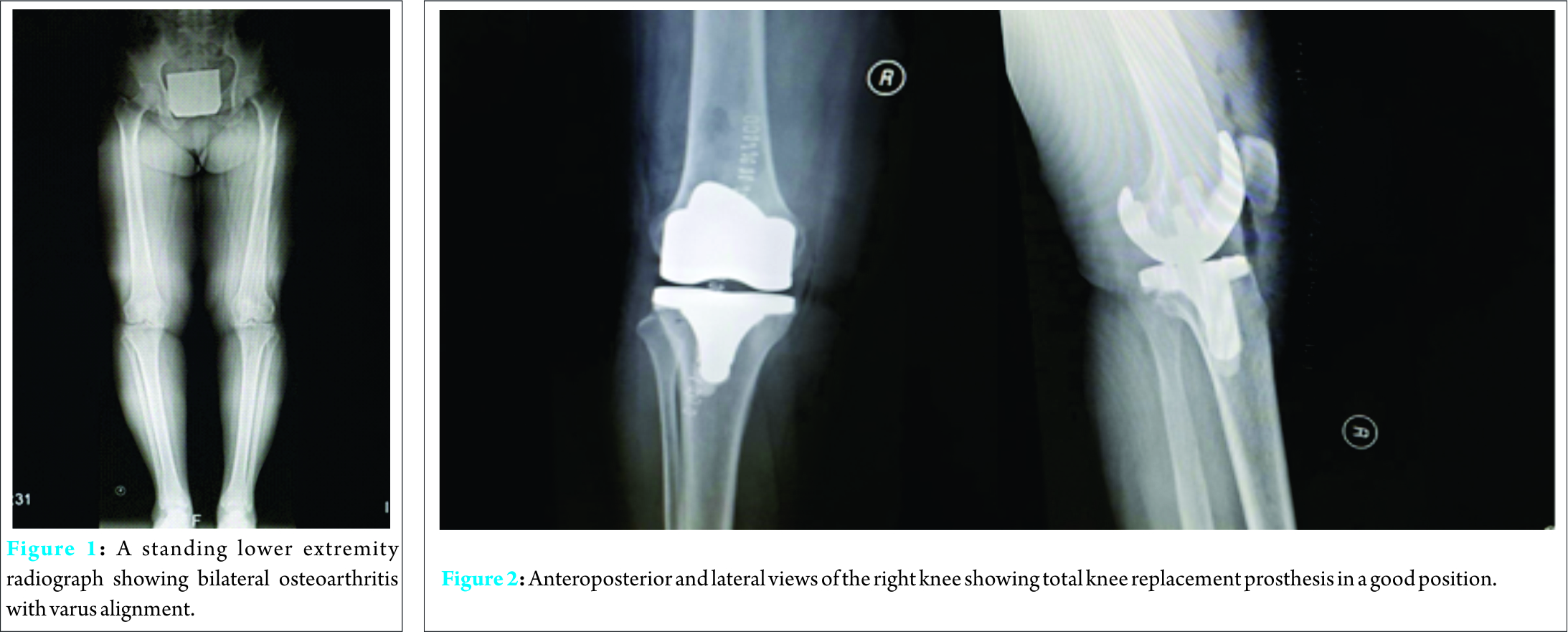
Discussion
We present an uncommon postoperative complication following an elective TKR in a 53-year-old woman who developed acute cholecystitis 13 days post TKR, which was treated by laparoscopic cholecystectomy and intravenous antibiotics.
The first reported case of acute cholecystitis as a postoperative complication was in 1844 by Duncan, which followed a femoral hernia repair [4]. In 1933, Fisher was first to document a case after an orthopedic procedure in a nineteen-year-old football player after an open reduction of his scaphoid bone. By 1953, thirty-nine cases were added and five occurred after a variety of orthopedic operations. More orthopedic cases complicated by acute cholecystitis were reported later. Those occurred mainly after hip operations (trauma and arthroplasty) and, to a lesser extent, hemipelvctomy, spinal fusion, and others [4]. J Abrahamsson et al.’s review of the literature revealed that gastrointestinal and abdominal operations were procedures most frequently associated with acute cholecystitis (40%) and that orthopedic operations (16.5%) were the second most common [4]. Acute cholecystitis after a major joint replacement is not uncommon. A lot of factors may lead to this postoperative complication, including stasis of highly viscid bile induced by dehydration, hypovolemia, fever, obstruction at the sphincter of Oddi following starvation, narcotics, and anesthesia [4]. Other factors are pigment load following blood transfusion, sympathetic stimulation, impaired circulation to the gallbladder, and septicemia with septic emboli reaching the gallbladder [4]. A study reported the incidence of acute cholecystitis in twenty patients (14 males and 6 females) while recovering from other surgical procedures (nine orthopedic procedures, six of them for fractures, four gastrointestinal procedures, three urological procedures, and two underwent thoracotomy) [1]. Tenderness and pain were the most common clinical sign and symptom and presentation ranged between 3 and 29 days postoperatively, with an average of 16 days [1]. In another study, complications occurred 3–10 days after different orthopedic operations (elective primary hip replacements, hip revisions, and open reduction internal fixation of hip fractures) [5]. As we reported here, our patient experienced a severe attack of gallbladder inflammation two weeks post total knee replacement. This was diagnosed clinically and radiographically and then confirmed by the pathology report as “Acute Gangrenous Cholecystitis”. A case report from the Cleveland Clinic, Ohio, documented a 64-year-old patient, whose general physical health was excellent and past medical history and systematic review negative for any conditions or risk factors. This patient progressed to acute cholecystitis requiring cholecystectomy after total knee arthroplasty for tricompartmental osteoarthritis [6]. On his sixth postoperative day, the patient was clinically jaundiced and on the ninth day he was diagnosed with acute cholecystitis in the operating room while performing laparotomy (they found inflamed GB with multiple stones). Camer [7] reported a total of 25 patients who developed acute cholecystitis after a major total joint surgery. Clinical characteristics of significance are reported as age greater than 60 years, prolonged limited oral intake (resulting in poor gallbladder emptying, bile stasis, and cystic duct obstruction), and the onset of symptoms soon after the resumption of food intake [7]. Our patient was placed on a liquid diet for only two days postoperatively and she was not able to resume a solid diet for one week due to her decreased appetite. In our case, cholecystitis ran an acute, progressive course over a period of two days, similar to that reported among most patients in Camer’s study [7], where 23 patients required emergency laparotomy for the “unusual fulminant course” of their acute cholecystitis. He therefore recommended prophylactic surgical treatment for patients with a history of symptomatic gallstones prior to major joint arthroplasty to avert the three-fold increase in morbidity and the ten-fold increase in mortality associated with emergency versus elective cholecystectomy. The risk of acute cholecystitis can be evaluated by a preoperative oral cholecystogram or ultrasound examination [8]. However, these examinations are not routinely performed preoperatively without a prior history of significant symptomatology [6]. Our patient did not have a history of gastrointestinal symptoms that would suggest underlying gallbladder disease.
A four-year case control study was conducted at the Konstantopoulio General Hospital in Athens, Greece, in which the study group consisted of 100 patients who experienced an infection following orthopedic surgery while 100 controls were randomly selected among patients who had undergone orthopedic surgery without a subsequent infection [9]. They evaluated the risk factors associated with infection after the orthopedic procedures, such as fracture osteosynthesis, joint replacement, spinal surgery, and others [9]. Surgical site infection (SSI), urinary tract infection (UTI) and pneumonia developed in the majority of cases, whereas only one patient had acute cholecystitis. Coagulase-negative Staphylococci and E. coli were the most common organisms identified in their study, whereas in our patient the organisms were Enterococcus, Enterobacteriaceae and Escherichia coli. The authors also found that age, obesity, ASA score, the duration of urinary catheterization, the anatomical location of the surgical procedure, the type of anesthesia, and the kind of chemoprophylaxis regimen were risk factors for postoperative infections [9]. In hip surgeries specifically, although it is rare, abdominal complications do occur and are associated with unfavorable outcomes. In a study from Romania [4], they aimed to identify and describe the severe and different types of abdominal complications following elective or traumatic hip surgery. A four-year retrospective electronic database search identified 408 elective primary hip arthroplasty, 51 hip revisions, and 1040 intra and extracapsular proximal femur fractures. Out of these, three males and four females between the ages of 64 and 84 years were identified to have acute abdominal complications following their operation. These were: perforated acute ulcer (3 patients), acute cholecystitis (2 patients), volvulus (1 patient), toxic megacolon with peritonitis (1 patient), and acute colonic pseudo-obstruction (1 patient). Another case reported from Haifa Medical Centre documented a 69-year-old man who had undergone a left total hip replacement for osteoarthritis under general anesthesia. He had no previous history of GI complaints [4]. On his 21st postoperative day he lost his appetite and complained of fatigue, nausea, and colicky epigastric pain associated with fever. On physical examination, there was tenderness in the right hypochondrium. A necrotic calculus gallbladder was resected from his operation (4).
Conclusion
Careful and detailed preoperative patient evaluation is important in identifying patients at risk of developing such a rare complication and to treat them proactively. Similarly, careful postoperative follow-up of these patients can help identify these complications early and treat them in a timely fashion to prevent major complications that could lead to morbidity or even mortality.
Clinical Message
No clear consensus is present on how long these patients should be kept on antibiotics post laparoscopic cholecystectomy after TKR, but for the time being, close follow-up and appropriate investigations are warranted to detect these infections and treat them early to avoid morbidity and mortality.
References
1. Howard RJ, Delaney JP. Postoperative cholecystitis. Am J Dig Dis 1972;17(3):213-8.
2. Floman Y, Micheli LJ, Barker WD, Hall JE. Acute cholecystitis following the surgical treatment of spinal deformities in the adult: a report of three cases. ClinOrthopRelat Res 1980;(151):205-9.
3. Devine RM, Farnell MB, Mucha P. Acute Cholecystitis as a Complication in Surgical Patients. Arch Surg 1984;119(12):1389-1393.
4. Abrahamson J, Eldar S. Acute cholecystitis after orthopaedic operations. IntOrthop. 1988;12(1):93-5.
5. Deleanu B, Prejbeanu R, Vermesan D, Haragus H, Icma I, Predescu V. Acute abdominal complications following hip surgery. Chirurgia (Bucur) 2014;109(2):218-22.
6. Wilde AH, Sweeney RS, Borden LS. Hematogenously acquired infection of a total knee arthroplasty by Clostridium perfringens. ClinOrthopRelat Res. 1988; (229):228-31.
7. Camer SJ. Surgical complications in revision arthroplasty. In: Turner R, Scheller A, eds: Revision Total Hip Arthroplasty. New York:Grune and Stratton, 1982:315-27.
8. Skoff HD. Acute cholecystitis and liver failure after total hip replacement. A case report. Orthopedics. 1986;9(5):693-6.
9. Masgala, Chronopoulos E, Nikolopoulos G, et al. Risk factors affecting the incidence of infection after orthopaedic surgery: the role of chemoprophylaxis.” Cent Eure J Public Health 2012;20(4) : 252-256.
| How to Cite This Article: Ghalimah B, Hamdi A. Acute Cholecystitis Following Total Knee Replacement: A Case Report and Literature Review. Journal of Orthopaedic Case Reports 2016 April – June;6(2): 100-102. Available from: https://www.jocr.co.in/wp/2016/04/01/2250-0685-460-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


