
[box type=”bio”] What to Learn from this Article?[/box]
Usually lateral meniscus cyst is common and mostly congenital but in our case patient had history of trauma and pain onmedial meniscus. So while evaluating patient traumatic history should always be ruled out.
Case Report | Volume 6 | Issue 3 | JOCR July-Aug 2016 | Page 7-9 | Prafulla Herode, Abhijeet Shroff, Vishal Mandlewala, Amit Chaudhary. DOI: 10.13107/jocr.2250-0685.474
Authors: Prafulla Herode[1], Abhijeet Shroff[1], Vishal Mandlewala[1], Amit Chaudhary[1]
[1] Department of Orthopaedics, Dr. D.Y.Patil medical college and research centre, Pune. Maharashtra. India.
Address of Correspondence
Dr. Prafulla Herode,
Dr. D.Y.Patil medical College and Research Centre, Orthopaedic Department, Pune – 411018. Maharashtra. India.
E-mail: pgherode@yahoo.co.in
Abstract
Introduction: Meniscal cysts are rare, in that cysts of lateral meniscus are 3 times to 10 times more common than those of medial meniscus. Etiology of meniscal cysts includes trauma which results in contusion and haemorrage within the substance of meniscus leading to mucoid degeneration. Degeneration with age results in local necrosis and mucoid degeneration into a cyst, developmental inclusion of synovial cells within the substance of the meniscus and often are a result of extrusion of synovial fluid through a tear of the meniscus, resulting in a one-way valve effect of the tear. Arthroscopic partial menisectomy followed by cyst decompression is currently recommended for treatment of a meniscal cyst.
Case Presentation: We present a case of 18-year-old female with c/o pain and swelling in right knee had h/o trauma 3 yrs back. On examination, swelling 1×2 cm on medial tibial condyle, firm in consistency fixed to bone. MRI suggests grade 3 horizontal tear in posterior horn of medial meniscus and parameniscal cyst adjacent to medial meniscus. In this report, medial parameniscal cyst was resected using an arthroscopic posterior trans-septal approach. There have been no recurrences to date, and patient returned to her previous level of activity.
Conclusion: A posterior trans-septal approach is useful for resection of a meniscal cyst arising from the posterior horn of the medial meniscus.
Keywords: meniscal cyst, parameniscalsyst, meniscectomy, arthroscopic meniscectomy, trans-septal approach
Introduction
Meniscal cysts are rare. Cyst of lateral meniscus is 3 times to 10 times more common than cyst of medial meniscus. Etiology of meniscal cysts includes trauma which results in contusion and haemorrage within the substance of meniscus leading to mucoid degeneration, degeneration with age which results in local necrosis and mucoid degeneration into a cyst, developmental inclusion of synovial cells within the substance of the meniscus and often are a result of extrusion of synovial fluid through a tear of the meniscus, resulting in a one-way valve effect of the tear. Arthroscopic partial menisectomy followed by cyst decompression is currently recommended for treatment of a meniscal cyst.
Case Presentation
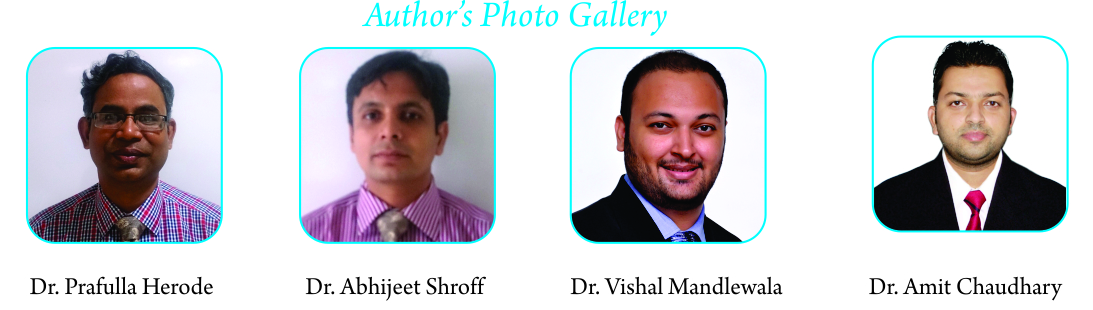
We present a case of 18-year-old female with complains of pain and swelling in right knee and had a history of trauma 3 years back. Pain was insidious in onset, and mild in intensity. Swelling was not present initially, but developed 1 1/2 year back. The patient experienced locking of knee while walking. On examination, there was a swelling 1×2 cm on medial tibial condyle, firm in consistency. It was fixed to bone. Plain X-ray of knee in the antero-posterior and lateral view didn’t show any abnormality. Magnetic resonance imaging showed grade 3 horizontal tear in posterior horn of medial meniscus and parameniscal cyst adjacent to medial meniscus. Patient was posted for medial parameniscal cyst resection using an arthroscopic posterior trans-septal approach. Arthroscopic surgery was performed under spinal anesthesia without a pneumotourniquet. The knee was flexed at more than 90 degrees on the operating table using a foot stopper. Anterior cruciate ligament, posterior cruciate ligament and both lateral and medial meniscus was intact under arthroscopic examination. The posteromedial compartment was examined from the anterolateral portal through the intercondylar space. The surface of the posterior horn of the medial meniscus was intact and cyst-like lesion was found on the edge of the posterior segment of the medial meniscus. While starting of the procedure for making a trans-septal portal, the posteromedial and posterolateral portals was created according to the approach reported by Ahn et al. After making a posterolateral portal, a rod with a sheath was inserted through the posterolateral portal to the septum. Pushing the sheath into the septum, the arthroscope was then inserted into the posteromedial portal. While maintaining the view of the medial side of a septum, a 3.0 mm Kirschner wire was pushed into the septum through the sheath from the posterolateral portal and then the septum was perforated. The Kirschner wire was pushed 2 or 3 times into the septum to enlarge the initial hole so that the switching rod could easily pass through the septum. Then, the switching rod was inserted from the posterolateral portal to the posteromedial portal via the trans-septal portal. Once the trans-septal portal was created, the arthroscope and instruments are easily interchangeable through the two posterior portals according to the posterior “back and forth” approach presented by Louisia et al. Viewing from the posteromedial portal, proliferated synovial tissues expanding from the posterior horn of the medial meniscus to the posterior septum was found. The cyst and posterior septum was resected by a punch and a motorized shaver inserted from the posterolateral portal while viewing from the posteromedial portal. When the cyst ruptured, a clear mutinous fluid seeped from the cyst cavity. A meniscal tear was not found although the posterior edge of the medial meniscus was carefully examined by a probe after cyst resection. The patient’s pain disappeared completely during the 10-month follow-up period and there is no recurrences till date.
Discussion
Medial parameniscal cysts of the knee are typically 0.3 to 9mm in diameter [1] .Previously, 4 cases have been documented for medial meniscal cyst. Furthermore, in all 4 cases, the meniscal cysts were openly excised. Open excisions of meniscal cysts pose greater risks of infection, inadvertent damage to the meniscus and surrounding structures during surgery, and longer time to recovery and return to mobility for the patient. This case highlights the management of a posterior horn of medial meniscus and parameniscal cyst adjacent to medial meniscus that was managed arthroscopically with good post-operative recovery.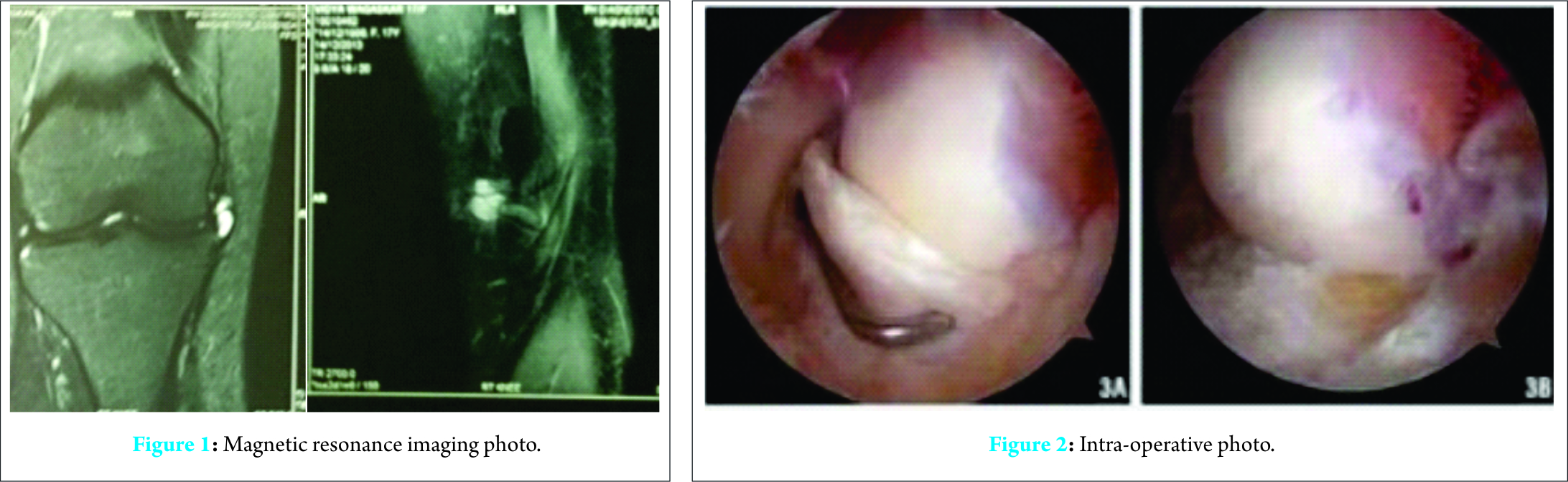
Resection of a meniscal cyst involving the septum is difficult by the intercondylar approach from two anterior portals even with a posteromedial portal in addition for managing the procedure. Although the use of a 70-degree arthroscope can help the visualization of the posterior compartment, the whole area of the septum cannot be visualized since the camera head of an arthroscope is too close to the septum from an anterior intercondylar approach. Although the septum can be viewed clearly from the posteromedial portal, it is cumbersome to manage the instruments to excise the cyst from anterior portals or from an additional high posteromedial portal. In our case, a posterior trans-septal approach was employed for the resection of the meniscal cyst as this approach allows an operator to identify the posterior edge of the medial meniscus, the septum and PCL and to treat the lesions involving those structures easily. A trans-septal approach was initially reported by Kim et al. in 1996 [2]. This technique is quite useful for accessing the posterior compartment of the knee, however the operator should bear in mind the risk of popliteal neurovascular injury when making a trans-septal portal. Hence, the use of pneumotourniquet should be avoided. Almost all meniscal cysts are accompanied by some meniscal tear, including grade 3 lesions judged by MRI, although it is not obvious on the surface of the meniscus. In such case as ours, an open cystectomy is recommended according to the therapeutic options for meniscal cysts [3]. However, substantial damages in the surrounding soft tissue, especially damage to the posterior capsule, at the popliteal fossa could be unavoidable by an open procedure since the lesion is deep under the skin. Recently, all arthroscopic procedures for selective menisectomy with cyst decompression or cyst drainage with suture of the torn meniscus were reported to preserve or restore a meniscal function [4, 5, 6]. Howe et al. demonstrated excellent results for a long follow-up period by creating a small channel at the capsule adjacent to the cyst for decompression of the cyst into the joint without causing harm to the healthy meniscus [7]. Small parameniscal cysts are rarely symptomatic, larger cysts located posteriorly may present with pain and persistent swelling due to pressure on surrounding structures. Our patient experienced pain, swelling and locking over a period of 3 years. A voluminous posterior medial meniscal cyst could present in the popliteal fossa, and coupled with its size, may be misdiagnosed as a Baker’s cyst. Distinguishing a meniscal cyst from a Baker’s cyst is important as Baker’s cysts are usually associated with osteoarthritis of the knee. They may often resolve spontaneously and hence should be treated conservatively [8]. However, arthroscopic repair or debridement of a meniscal tear with the aim of preventing recurrence is the usual treatment for a meniscal cyst [9]. MRI and arthroscopy are useful in distinguishing a perimeniscal cyst from a Baker’s cyst in such a scenario. Most meniscal cysts (91%) occur immediately adjacent to the meniscal tear (98% horizontal cleavage tears, 49% anterolateral), with the tear communicating directly with the cysts, and produce a homogenous signal on MRI [10, 11]. Furthermore, demonstration of the origin of a Baker’s cyst between the muscles of the medial gastrocnemius and semi membranosus allows for differentiation from a meniscal cyst.
Conclusion
A posterior trans-septal approach is useful for resection of a meniscal cyst arising from the posterior horn of the medial meniscus, especially in the case where the lesion involves the posterior septum. This is only a case report further cases are awaited.
Clinical Message
Post traumatic knee pain should not be neglected even though all clinical signs are negative. Rare causes like meniscal cyst can also cause pain.
References
1.Barrie HJ. Pathogenesis and significance of meniscal cysts. J Bone Joint Surg Br 1979; 61(2): 184-9.
2. Kim JM: Direct posterior-posterior triangulation of the knee joint. Arthroscopy 1996; 13:262-264
3. Pedowitz RA, Feagin JA, Rajagopalan S. A surgical algorithm for treatment of cystic degeneration of the meniscus. Arthroscopy 1996;12:209-212.
4. Lonner JH, Parisien JS. Arthroscopic treatment of meniscal cysts. Operative Techniques in Orthopaedics 1995;5:72-77.
5. Ahn JH, Wang JH, Yoo JC, Kim SK, Park JH, Park JW. The modified outside-in suture: vertical repair of the anterior horn of the meniscus after decompression of a large meniscal cyst. Knee Surg Sports TraumatolArthrosc 2006;14:1288-1291.
6. Lu KH. Arthroscopic meniscal repair and needle aspiration for meniscal tear with meniscal cyst. Arthroscopy 2006;22:1367, e1-4.
7. Howe TS, Koh JS. Arthroscopic internal marsupialization of meniscal cysts. Knee 2007;14:408-410.
8. Kocher MS, Klingele K, Rassman SO. Meniscal disorders: normal, discoid, and cysts.OrthopClin North Am 2003;34(3): 329-40
9. Sheah K, Png MA. Meniscal cyst causing periarticulartibial erosion. Singapore Med J 2005; 46(3): 137-9
10.Tyson LL, Daughters TC Jr, Ryu RK, Crues JV 3 rd . MRI appearance of meniscal cysts. Skeletal Radiol 1995;24(6): 421-4.
11. Mountney J, Thomas NP. When is a meniscal cyst not a meniscal cyst? Knee 2004; 11(2): 133-6.
| How to Cite This Article: Herode P, Shroff A, Mandlewala V, Chaudhary A. Post-traumatic Medial Meniscal Cyst in young: A case report. Journal of Orthopaedic Case Reports 2016 July-Aug;6(3):7-9. Available from: https://www.jocr.co.in/wp/2016/07/10/2250-0685-474-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


