
[box type=”bio”] What to Learn from this Article?[/box]
Surgeon should be consider in mind the diagnosis of Pseudoaneurysm after open reduction and internal fixation or also after plate removal when the patient refer by swelling, hearing bruit or decreases pulse.
Case Report | Volume 6 | Issue 3 | JOCR July-Aug 2016 | Page 46-49 | Salman Ghaffari, Hossein Farsavian, Seyed Mohamad Mehdi Daneshpoor, Masoud Shayesteh Azar. DOI: 10.13107/jocr.2250-0685.500
Authors: Salman Ghaffari[1], Hossein Farsavian[1], Seyed Mohamad Mehdi Daneshpoor[1], Masoud Shayesteh Azar[1]
[1] Department of Orthopaedics, Orthopaedic Research Center, Mazandaran University of Medical Science, Sari, Iran.
Address of Correspondence
Dr. Hossein Farsavian,
Department of Orthopaedics, Orthopaedic Research Center, Mazandaran University of Medical Science, Sari, Iran.
E-mail: h.farsavian@yahoo.com
Abstract
Introduction: Pseudoaneurysm is a rare complication reported after any surgery such as ORIF of fracture, plate removal, ankle or knee arthroscopy, or arthroplasty. To our knowledge, pseudoaneurysms of the posterior tibial artery after tibial plate removal are a rare phenomenon. We report a case of an18 year-old male patient who had pseudoaneurysm of posterior tibial artery following plate removal.
Case Presentation: An 18-year-old male was referred to our outpatient clinic because of mass-like lesion in his left calf. He had a history of car accident and left isolated tibia fracture 30 months ago that was treated by open reduction and internal fixation with DCP plate. After union in radiograph, the plate was removed 7 months ago on the patient request. Four weeks after surgery, the patient had complaints of pain and swelling. Finally, pseudoaneurysm was diagnosed and was repaired in a common surgery with a vascular surgeon without any difficulty.
Conclusion: Pseudoaneurysms of the posterior tibial artery after tibial plate removal are an extremely rare phenomenon. This complication in most cases follows penetrating injuries but it has been reported following blunt trauma. In fact, in most of these patients the diagnosis was initially missed because the large hematoma concealed the underlying pseudoaneurysm and its pulsations. Thus, a delay in the diagnosis is common in this phenomenon. Hence, the surgeon should be suspicious to this complication following plate removal when he/she is doubtful about the sign and symptoms.
Keywords: Pseudoaneurysm, tibia fracture, plate removal, complication.
Introduction
Implant removal in orthopaedic procedures have more frequently been a subject of controversy [1, 2]. Some surgeons prefer to remove the implant routinely in skeletally immature patients and also in adults, others do this by patient’s request or when complications such as infection, pain, breakage, malunion, delayed or nonunion occurs [3]. We present a 18-year-old male patient with isolated pseudoaneurysm of the posterior tibial artery (proximal third) after plate removal in tibia. The patient presented to our outpatient department with complaints of a firm, pulseless, non-tender swelling on the posterior aspect of the leg which gradually increased in size by overtime. This patient was successfully treated with hematoma evacuation and resection of pseudoaneurysm.
Case report
An 18-year-old male patient was referred to our outpatient clinic because of mass-like lesion in his left calf. He had a history of car accident and left isolated and closed tibia fracture 30 months ago that was treated by open reduction and internal fixation with 4.5mm broad DCP plate (Fig. 1, 2). The surgical approach was through 1 cm lateral to tibial crest and plate was in lateral aspect of tibia. In this period, the patient was fully asymptomatic and had no complaint in routine follow-up. The patient had no significant past medical history. After 2 years, union was obvious in AP and lateral radiographs, and removal of tibial plate was decided. The plate had been removed 7 months ago on patient’s request. At the time of surgery, we used the previous incision and found that the bone was completely united. Plate and screw removal was done without any complication (eg, plate or screw break down). After the operation, the bone in radiograph was completely united and the patient was discharged when we find near 50-100 cc collection in the drain at the second day post operation.(Fig. 3). Examination at this time showed he was intact in neurovascular examination. At the first post operation visit, he was asymptomatic and progressive part weight bearing had been described. About 4 weeks after plate removal, he came back with mild paresthesia in the left foot at the plantar surface. Also, he had firm, pulse less and non-tender swelling with unclear border on the posterior aspect of the leg which gradually increased over time. Position of ankle was plantigrade. In vascular examination, we found the dorsalis pedis and the posterior tibialis pulses were equal to the opposite leg. We followed this patient without further investigation. At about 3 months after plate removal, paresthesia became persistant. We prescribe EMG/NCV for the patient. This assessment showed tibial nerve axonal injury pattern. Thus, we thought that paresthesia was due to iatrogenic tibial nerve injury (eg, bennet tip). Approximately 5 months after surgery, he returned with calf muscle firmness and occasional spasm like pain. Paresthesia remained mild and distal pulses were normal and swelling was more firm and fixed.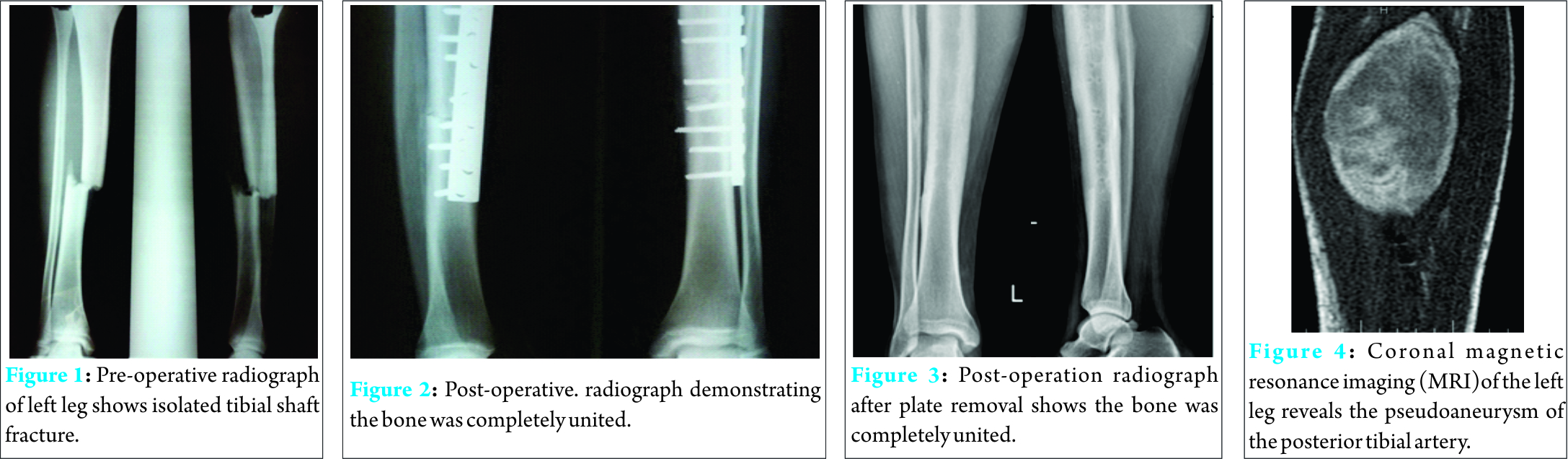
In physical exam, the skin over the mass was intact and we didn’t see ecchymosis or discoloration in this area. We found no lymphadenopathy. We found no tenderness at the fracture site and patient didn’t compliant from pain similar the previous fracture. Neurologic examination revealed normal force but decreased sensation in this mentioned area. We heard bruit over the surface of this mass.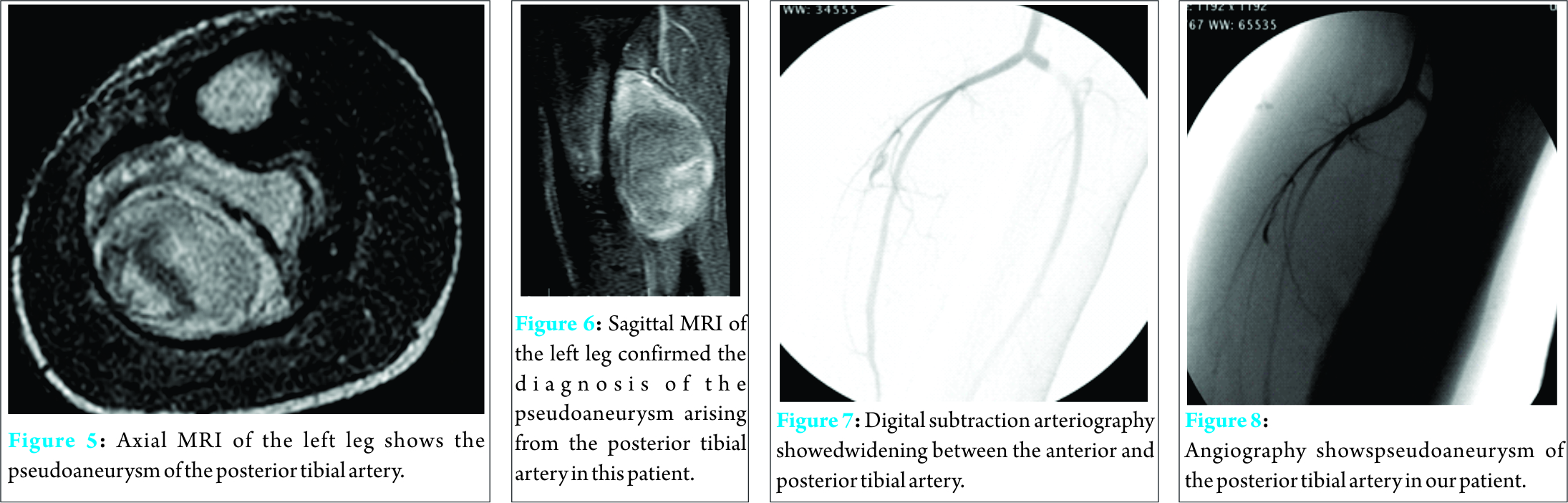
MRI was requested for this patient for calf muscle evaluation. At 1 month after MRI request, the patient came back and discovered a large (5 × 7 cm) soft tissue mass that was enhanced with probable diagnosis of hemotoma or pseudoaneurysm (Fig. 4-6). Ultrasonography showed the pseudoaneurysm and an angiography was planned. After the patient was systemically heparinized with 5000 units of unfractionated heparin, angiography showed the widening between the anterior and posterior tibial artery which confirmed the pseudoaneurysm of the posterior tibial artery (Fig. 7, 8). Thus, we proceeded for a common surgery with a vascular surgeon. During the common surgery, clots and hemotoma was evacuated and the posterior tibial artery perforation was repaired (Fig. 9, 10).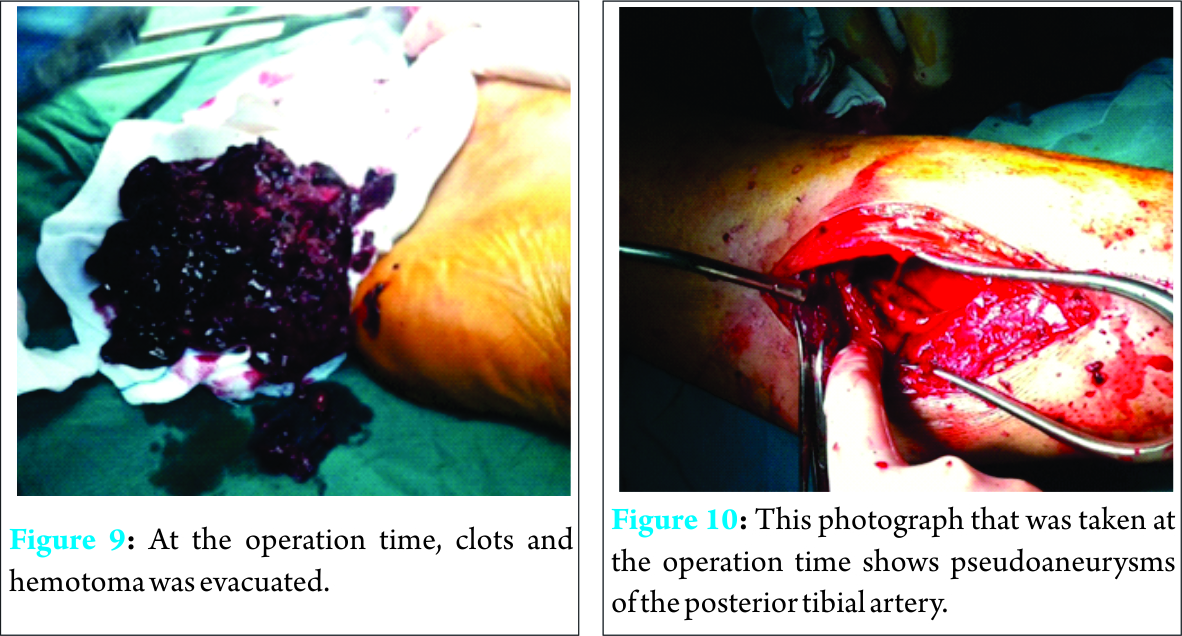
Discussion
To our knowledge, pseudoaneurysms of the posterior tibial artery after tibial plate removal are too rare phenomenon [4, 5]. This branch of popliteal artery begins at the lower border of the Popliteus, descends obliquely and supplies the posterior compartment of the leg and plantar surface of the foot. Along its course, it accompanied by the posterior tibial vein [6, 7]. Pseudoaneurysms in most cases follow penetrating injuries but in our case it has been reported following blunt trauma [8, 9]. Indeed, the literature showed that in most of these patients the diagnosis was initially missed because the large hematoma concealed the underlying pseudoaneurysm and its pulsations. Thus, delay in the diagnosis is usual in this phenomenon [8, 10]. Maxwell-Armstrong and his co-author reported pseudoaneurysm of the anterior tibial artery following removal of tibial plate [11]. Fung and his co-authors also reported pseudoaneurysm of the radial artery following plate removal in radius[12]. Although this complication can be seen after fixation of leg, distal radius, clavicle and femur fracture with plate, total knee arthroplasty, the overall pseudoaneurysm incidence after plate removal is unknown but in our knowledge it is too rare [13-17]. In this manuscript, we present an 18-year-old male patient with a mass in his left calf that was diagnosed pseudoaneurysm of the posterior tibial artery. The time for the diagnosis of pseudoaneurysm in the literature is seen to vary from hours to years, depending on the location of pseudoaneurysm and clinical signs and symptoms. The signs and symptoms include a pulsatile mass, pain, swelling, bruit, blood and neurologic deficit. Repair of tibial artery pseudoaneurysm can be challenging and a different surgical operation was described in the recent manuscripts such as direct arterial repair, interposition grafting or arterial ligation, duplex-guided compression and finally endovascular intervention [17-19]. During surgery, left leg is elevated for 2 minutes and then the tourniquet turned on and inflated to 280 mm Hg. The present surgery was done through the incision over the line that had greatest firmness. After blunt dissection between muscles, we found the mass included hemotoma. This was near the upper border of plate. Clots were removed and irrigation performed. A perforation was found in posterior tibial artery at the proximal third which was repaired with prolin 5-0 (Fig. b9, 10). In this patient, it was not obvious whether this injury was caused by direct tearing of the artery or due to plate removal, but it’s important to note that we should turn off the tourniquet and carefully find bleeding origin in any operation in the proximity of major vessels. Another point that we should say is this complication may be a pulsless mass, thus pulslessness couldn’t rule out the pseudoaneurysm. We suggest having this complication in mind and being familiar with the presentation of the signs and symptoms. It seemed vital to release the tourniquet before closing the wound to prevent this complication rate.
Conclusion
Pseudoaneurysm is a rare complication caused by a vascular injury. In our knowledge, incidence of this complication is unknown, but has been reported after any surgery such as ORIF of fracture, plate removal, ankle or knee arthroscopy, or following arthroplasty. Although in most cases we find a pulsatile soft tissue mass, but we should know that the mass may be pulseless which may cause misunderstanding and delay in the diagnosis. In most cases, the diagnosis is delayed initially owing to slow progression in sign and symptoms. An important key in the diagnosis is that the surgeon should have a high degree of suspicion when the patient compliants of a mass, with paresthesia and pain that was inappropriate to the operation and soft tissue swelling. Further assessment should be carried out carefully. When the diagnosis is confirmed, patient should be referred to a vascular surgeon. At a final result, we should release the tourniquet before wound closure for accurate hemostasis and decrease this complication rate.
Clinical Message
Diagnosing of this complication can be challenging , especially after plate removal. Orthopaedic surgeon should consider pseudoaneurysm in his/her mind even if this complication is too rare after plate removal.
References
1. Mue DD,Yongu WT, Elachi IC, Salihu MN. Surgeons’ Perceptions about Removal of Orthopaedic Implants in Nigeria. IOSR Journal of Dental and Medical Sciences 2014;13(9):08-13.
2. Onche I. I, Osagie O. E, Nuhu S. I. Removal of orthopedic implants: indication, outcome and economic implication. J West Afr Coll Surg. 2011; 1(1):101–112
3. Eastwood D. M, Sanghrajka A. P. Aspects of current management, Guided growth. J Bone Joint Surg [Br].2011;93-B:12-18.
4. Craxford S, Karuppiah SV, Milner S. Pseudoaneurysm of the Anterior Tibial Artery following Tibio-Talar-Calcaneum Fusion with a Retrograde Nail: A Rare Case and Literature Review. Case Reports in Orthopedics. Volume 2013.
5. Christofilopoulos P, Panos A, Masterson K, Abrassart S, et al. Pseudoaneurysm of the anterior tibial artery following an ankle sprain: a case report of an uncommon ankle trauma with review of the literature. Foot and Ankle Surgery 2008;14(1):40-42..
6. Moore K.L. and Dalley A.F. Clinically Oriented Anatomy, 5th Edition, Lippincott Williams & Wilkins, Toronto, 2006.
7. Gray H. Anatomy of the Human Body. Philadelphia: Lea & Febiger, 1918; Bartleby.com, 2000. www.bartleby.com/107/.
8. Joshua A, Hager E, Martin N D. Lower extremity vascular stenting for a post-traumatic pseudoaneurysm in a young trauma patient. J Emerg Trauma Shock 2011; 4(2):302–305.
9. Van Hensbroek PB, Ponsen KJ, Reekers JA, Goslings JC. Endovascular treatment of anterior tibial artery pseudoaneurysm following locking compression plating of the tibia. J Orthop Trauma 2007;;21(4):279-82.
10. Breen T, Brumback R. Posterior tibial artery pseudoaneurysm following tibial fracture. A case report. Orthopedics 1985;8(8):993-7.
11. Maxwell-Armstrong C A, Taylor A.M, Majkowski R.S, Colton C.L. False aneurysm of the anterior tibial artery following removal of tibial plate. European Journal of Vascular and Endovascular Surgery 1995;10(4):505-506.
12. Fung BKK, Ip WY. Pseudoaneurysm of the radial artery after plate removal. Hong Kong Journal of Orthopaedic Surgery 2001;5(2):138-140.
13. Dao KD, Venn-Watson E, AY. Radial artery pseudoaneurysm complication from use of AO/ASIF volar distal radius plate: A case report. The Journal of Hand Surgery 2001;26(3):448-453.
14. Bain GI, Galley IJ, Keogh AR, Durrant AW. Axillary artery pseudoaneurysm after plate osteosynthesis for a clavicle nonunion: A case report and literature review. Int J Shoulder Surg 2010;4:79-82.
15. C Sarwar, S Riaz, R Lukhadwala. Iatrogenic Pseudoaneurysm Of The Superficial Femoral Artery In A Pediatric Patient: Case Report. The Internet Journal of Orthopedic Surgery Volume 2 Number 1.
16. Agarwala S R, Mohrir G S, Dotivala S J. Posttraumatic pseudoaneurysm of popliteal artery following total knee arthroplasty. Indian Journal of Orthopaedics 2013;47(1):101-103.
17. Joglar F, Kabutey NK, Maree A, Farber A. The role of stent grafts in the management of traumatic tibial artery pseudoaneurysms: case report and review of the literature. Vasc Endovascular Surg. 2010;44(5):407-9.
18. Filho M, Domingos de, El Hosni Jr., Abdallah R, et al. Pseudoaneurysm of the posterior tibial artery after external fixation for leg fracture: case report and review of the literature. Jornal Vascular Brasileiro 2007;6(2):175-181.
19. Khoury M, Batra S, Berg R, Rama K. Duplex-guided compression of iatrogenic femoral artery pseudoaneurysms. Am Surg. 1994;60(4):234-6; discussion 236-7.
| How to Cite This Article: Ghaffari S, Farsavian H, Daneshpoor SMM, Azar MS. Pseudoaneurysm of the Posterior Tibial Artery following Removal of Tibial Plate – A Rare Case. Journal of Orthopaedic Case Reports 2016 July-Aug: 6(3):46-49 . Available from: https://www.jocr.co.in/wp/2016/07/10/2250-0685-500-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


