
[box type=”bio”] What to Learn from this Article?[/box]
Treatment of large bone defect primarily or following infected non-union is no more a nightmare as induced membrane prevents the resorption of autograft.
Case Report | Volume 6 | Issue 3 | JOCR July-Aug 2016 | Page 59-62 | R Sivakumar, M Gulam Mohideen, M Chidambaram, T Vinoth, Prahalad Kumar Singhi, V Somashekar. DOI: 10.13107/jocr.2250-0685.508
Authors: R Sivakumar[1], M Gulam Mohideen[2], M Chidambaram[1], T Vinoth[1], Prahalad Kumar Singhi[1], V Somashekar[1]
[1]Department of Orthopaedics, Preethi Hospitals Pvt Ltd, Madurai. 625007. India.
[2]Department of Orthopaedics, Thanjavur medical college, Thanjavur. India.
Address of Correspondence
Dr. T Vinoth, MS Ortho
Consultant Surgeon; PRIOR, Preethi Hospitals Pvt Ltd, Madurai. 625007.
E-mail: drvinoththangamani@gmail.com
Abstract
Introduction: Management of the large gap in long bone fractures is a challenging problem after compound injuries. A novel technique called as Masquelet’s technique of “induced membrane formation”, is used to bridge a gap of more than 5 cm using bone cement as a spacer in first stage and autologous cancellous bone graft to fill the gap in second stage.
Case presentation: We present two different and difficult cases with bone defects after open injuries associated with long bone fractures in this paper. First case is a 50-year-old lady with grade IIIa open fracture right distal femur with intra-articular extension and bone loss. She underwent wound debriment, stabilization of the fracture with locking compression plate along with antibiotic cement spacer, which is removed latter and underwent bone grafting. Another is a 15-year-old boy with open grade IIIb fracture tibia and fibula (mid-distal third junction) of right leg, wound debridement and ankle spanning triangular external fixation was applied on same day and after two months, external fixation was removed due to florid infection and plaster of Paris was applied. Instead of the tedious and demanding treatment options like Ilizarov, a new technique described by Masquelet is used here. It uses bone cement as a spacer to fill the cavity to form pseudo-membrane around it and in the second stage autologous cancellous bone graft fills the gap of even more than 5 cm, to achieve union.
Conclusion: The membrane also secretes vascular and osteo-inductive factors to stimulate bone regeneration and also prevents resorption of the bone graft and achieves early fracture healing avoiding tedious options like bone transport in external fixator. By this two staged technique, union occurred clinically and radiologically in these two cases.
Keywords: bone defect, bone cement, induced pseudo-membrane, Masquelet, cancellous bone graft
Introduction
Management of the gap in long bone fractures is a challenging problem after compound injuries. For this, the treatment options are limited to external fixation like Ilizarov or LRS (limb reconstruction system) with bone transport, vascularised bone graft, fibular strut graft, etc. These techniques are associated with their morbidity and complications and require expertise. Vascularised grafts may not be useful in the presence of infection. A novel technique called as Masquelet’s technique of “induced membrane formation” [1-3], is used to bridge a gap of more than 5 cm using bone cement as a spacer in first stage and autologous cancellous bone graft to fill the gap in second stage.
Materials And Method
Two open fractures (one distal femur and another open and infected distal tibia) with bone defect treated with antibiotic bone cement in first stage followed by definite bone graft of the defects. Initially wound debridement/sequestrectomy and stabilization of fracture with internal or external fixation with bone cement spacer done. The bone cement is kept in place for 4-6 weeks and in second sitting it is removed and the pseudo-membrane cavity is filled with autologous cancellous bone graft.
First case: A 50-year-lady was hit by a car while riding a bike and presented with a grade IIIa open fracture right distal femur with intra-articular extension and bone loss. After stabilization and assessing her injuries, she was taken up for stabilization of fracture. Through lateral approach the distal femur was exposed and the fracture was found to be just bag of bones (Fig. 1) with lots of free bone fragments. These were removed and wound debridement completed. The fracture was stabilized with distal femur locking compression plate (Fig. 2).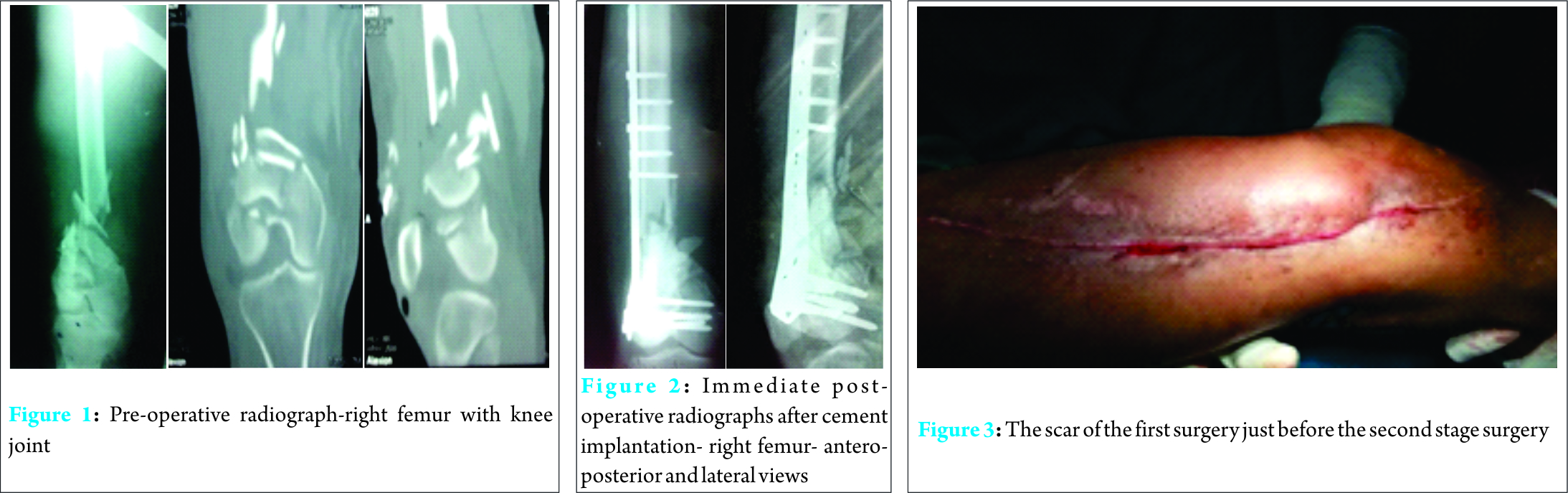 The bone gap created was measured to be 6 cm and is filled with 40g bone cement with 2g Vancomycin as spacer made on the table with a measure from the cavity, using a technique of gauze rolls described [4]. Vancomycin is used because it is heat-resistant. The wound closed over draining tube. Post-operative intravenous antibiotics were given for 2 weeks and oral antibiotics for 1 month. Post-operative period was uneventful. Six weeks later, she was taken to second stage surgery for removal of the cement spacer and grafting. Through incision scar of the previous surgery, the membrane formed around the spacer (Fig. 6) was sharply incised and the cement was extracted out (Fig. 5). Autologous iliac crest cancellous bone graft is harvested (Fig. 7) and the defect is filled and wound closed. Intravenous antibiotics were given for two weeks. At the end of two weeks the wound was healthy and suture was removed. The patient was discharged. The patient was reviewed regularly on 1st, 3rd, 6th and 12th months. Functionally and radio graphically the graft had incorporated into the bone and the continuity was restored at the fracture site (Fig. 2, 8, 9).The range of movement was 0 degree to 90 degree of flexion with full extension.
The bone gap created was measured to be 6 cm and is filled with 40g bone cement with 2g Vancomycin as spacer made on the table with a measure from the cavity, using a technique of gauze rolls described [4]. Vancomycin is used because it is heat-resistant. The wound closed over draining tube. Post-operative intravenous antibiotics were given for 2 weeks and oral antibiotics for 1 month. Post-operative period was uneventful. Six weeks later, she was taken to second stage surgery for removal of the cement spacer and grafting. Through incision scar of the previous surgery, the membrane formed around the spacer (Fig. 6) was sharply incised and the cement was extracted out (Fig. 5). Autologous iliac crest cancellous bone graft is harvested (Fig. 7) and the defect is filled and wound closed. Intravenous antibiotics were given for two weeks. At the end of two weeks the wound was healthy and suture was removed. The patient was discharged. The patient was reviewed regularly on 1st, 3rd, 6th and 12th months. Functionally and radio graphically the graft had incorporated into the bone and the continuity was restored at the fracture site (Fig. 2, 8, 9).The range of movement was 0 degree to 90 degree of flexion with full extension.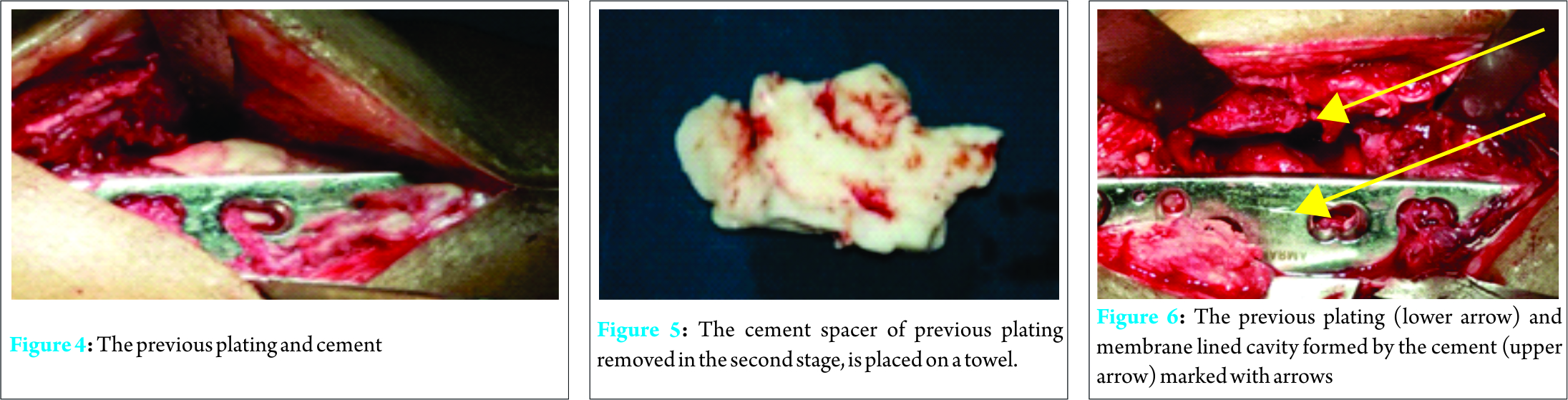
Case 2: 15-year-old boy with grade IIIb open fracture tibia and fibula (mid-distal third junction) of right leg along with closed fracture of the sub-trochanteric region of left femur. The left femur was immobilised in traction and three weeks later was fixed with DCS (dynamic condylar screw).
For the right leg wound, wound debridement and ankle spanning triangular external fixation was applied on the same day of injury (Fig. 10). The patient has persistent discharge in his leg wound for next two months. His leg radiographs showed large sequestrum (Fig. 10, 11, 12). External fixation was removed due to florid infection and plaster of Paris was applied (Fig. 11).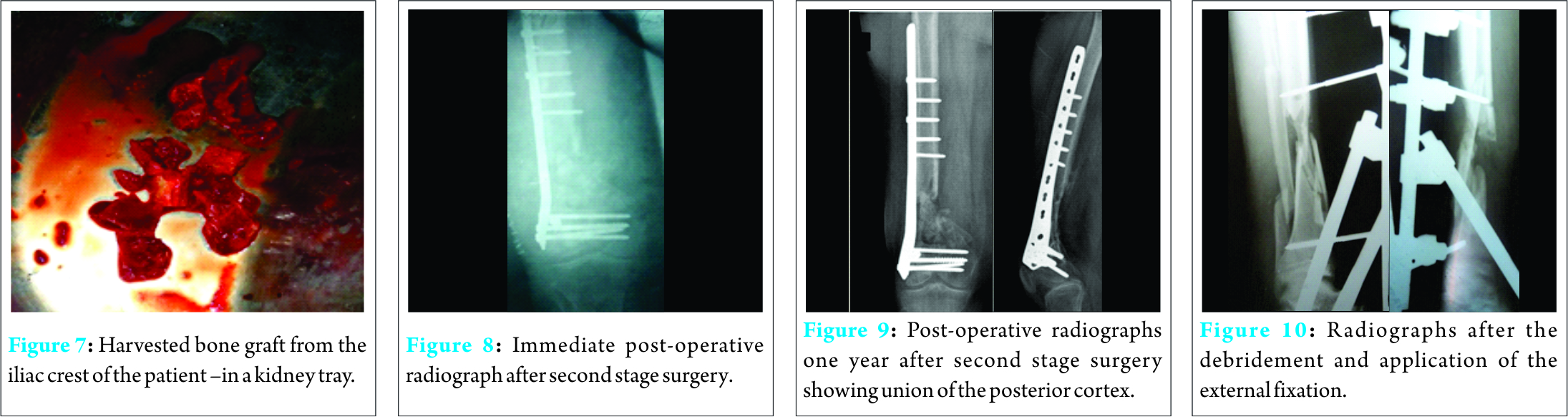
Later sequestrectomy followed by limb reconstruction system (LRS) was applied to stabilise the fracture (Fig. 12).
The large defect of 7 cm created following sequestrectomy was filled with 40g bone cement with 2g Vancomycin (Fig. 12). Postoperatively intravenous antibiotics were given for 2 weeks and oral antibiotics for 1 month. Post-operative period was uneventful. Six weeks after the sequestrectomy and cement application, he was taken to second stage of surgery for bone grafting.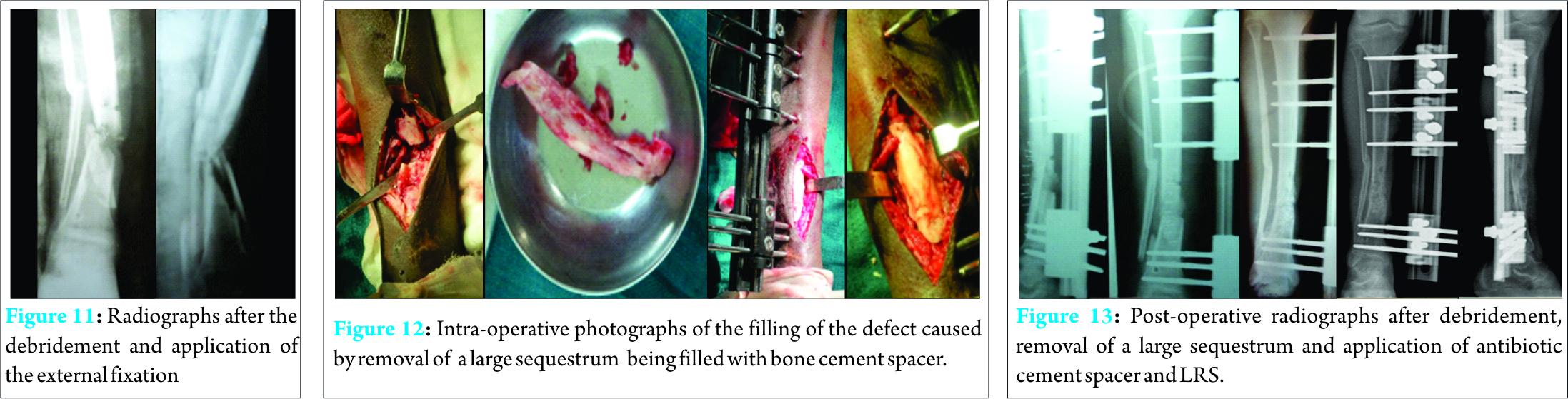
Through previous scar, the membrane formed around the spacer was sharply incised and the cement was extracted out. Autologous iliac crest cancellous bone graft is harvested to fill the gap and wound closed. Intravenous antibiotics was given for two weeks. At the end of two weeks the wound was healthy and suture was removed. The LRS was kept for 2 months following bone graft and replaced by plaster of Paris for one more month. The patient was reviewed regularly on 1st, 3rd, 6th and 12th months (Fig. 13). Functionally and radiographically the graft had incorporated into the bone and the continuity was restored at the fracture site.
Discussion
The management of segmental long bone defects is a challenge. Techniques available are difficult and have complications. Smaller defects can be treated with autologous bone graft and rigid fixation, but not when the defect size exceeds 5 cm. The significant bone defect is described by Key et al in 1953 is 1 ½ times the diameter of the bone at the place of the defect in the host bone. Because beyond 4-5 cm defect, the bone graft gets resorbed [1] and the defect remains. Even though cancellous bone graft have higher osteo-conductive and osteo-inductive capacities [1, 5, 6]. Larger defects can be treated by vascularised bone transfer or distraction histiogenesis. The transfer of vascularised bone is limited by pedicle length and training of microsurgical anastomose technique[7]. Distraction histiogenesis helps to bridge the bone gap but requires training, long learning curve and has complications. The technique of “induced membrane formation and bone grafting” was first described by Masquelet of France in 1986 [1]. This method was used to bridge the diaphyseal defects of up to 25 cm in length. As used in our cases, poly methyl methacrylate cement spacer kept in the cavity forms a membrane lined cavity forming a nidus (biological chamber) for the later grafting. These membranes have a rich capillary network and secretes growth factors (VEGF and TGF-beta 1) and osteoinductive factor (BMP-2) as early as 2 weeks [8, 9, 10]. The surface facing the cement is a synovium-like epithelium and the outer surface consist of fibroblast, myo-fibroblast and collagen. Last but not the least, according to Masquelet, membrane extracts were shown to stimulate bone marrow cell proliferation and differentiation to osteoblastic lineage [1]. If the cavity is large, the membrane prevents resorption of the cancellous bone graft in the vascular environment. The membrane promotes vascularisation and corticalisation of the cancellous bone [7,8]. The membrane also secretes osteoinductive factors [10].
The cement space tends to acts as a filler –spacer material maintaining the space erstwhile occupied by the bone, so that the length of the bone and the potential space of the removed necrotic bone is later filled by secondary autologous bone grafting [11]. This is done by not allowing the soft tissue around the bone to collapse at the fracture site [9]. Induced membrane in our case was documented by intra-operative photographs (Fig. 6) of the fracture gap after removal of cement spacer. Established infection present in the second patient (tibia) was managed with the instillation of the antibiotic laden acrylic cement .The heat-resistant antibiotic vancomycin is used. Antibiotic laden acrylic cement is already used in infections of implants and in osteomyelitis[12]. Philosophically it is told that the genesis of life takes place in a veiled environment be it a womb of another or a seed in the soil which germinates to produce a whole crop [13]. In our series the two cases were followed for an average period of 12 months after second procedure and in 12 weeks’ time, bony union occurred radiologically .This was followed by removal of the external fixation and plaster of Paris application for one more month in the tibia patient. Weight bearing was allowed after 16 weeks .In the femoral fracture patient, the patient was allowed to weight bear after 20 weeks. Both our cases went for complete acceptable union. The staged procedures are especially useful in infected lesions or when the viability of the segment is not initially known in a fool proof manner. The procedure is so useful that one need not choose vascularised bone transfers in such emergency infected conditions. The induced membrane technique of bone reconstruction first proposed by Masquelet for long bone defects can be used for hand and wrist defects also [1]. The induced membrane technique can address and allow early fracture healing in larger sizes of the defects. The only option which can come near is the Ilizarov method of bone transport which is tedious and needs more expertise.
Conclusion
Masquelet’s technique of induced membrane formation is effective in infected defects of long bones achieving a conductive milieu to allow graft consolidation that is applied in the second stage. The suggestion that the membrane also secretes vascular and osteoinductive factors to stimulate bone regeneration encourage the use of the procedure.
Clinical Message
Novel method of induced membrane formation by Masquelet’s cut short the prolonged time of bone formation in large gap by bone transport as needed in Ilizarov and limb reconstruction procedure. It also avoids the co-morbidities of long term external fixation.
References
1. Masquelet AC, Obert L. Induced membrane technique for bone defects in hand and wrist. Chir Main. 2010;29 (suppl1):S221-S224.
2. Masquelet AC, Begue T. The concept of induced membrane for reconstruction of long bone defects. Orthop Clin North Am.2010;41:27-37.
3. Klauke K, Knothe U, Rampoldi E, Masquelet AC, Perren SM. Biological implementation of ‘‘in situ‘‘ induced autologous foreign body membranes in consolidation of massive cancellous bone grafts. Orthopaedic proceedings. J Bone Joint Surg. 1993;79B (suppl 3):236.
4. Natarajan M, Dhanapal R, Kumaravel S, Hussain J, Selvaraj R, Yuvaraj. Indian J Orthop. 2003;37:15. The use of bovine calcium hydroxyapatite in filling defects following curettage of benign bone tumours.
5. Romana MC, Masquelet AC. Vascularised periosteum associated with cancellous bone graft: an experimental study. Plast Reconstr Surg. 1990; 85:587-592.
6. Masquelet AC, Fitoussi F, Begue T, Muller GP. Reconstruction des os longs par membrane induite et autogreffe spongieuse.Ann Chir Plast Esthet. 2000; 45:346-353.
7. Woon CY, Chong KW, Wong MK. Induced membranes e a staged technique of bone grafting for segmental bone loss: a report of two cases and a literature review. J Bone Joint Surg Am. 2010; 92:196-201.
8. Pelissier P, Masquelet AC, Bareille R, Mathoulin-Pelissier S, Amedee J. Induced membranes secretes growth factors including vascular and osteoinductive factors and could stimulate bone regeneration. J Orthop Res. 2004; 22:73-79.
9. Pelissier P, Martin D, Baudet J, Lepreux S, Masquelet AC. Behaviour of cancellous bone graft placed in induced membranes. Br J Plast Surg. 2002; 55:596-598.
10. Spinella-Jaegle S, Roman S, Faucheu C, et al. Opposite effects of BMP-2 and TGF beta-1 on osteoblast differentiation. Bone.1998; 29:323-330.
11. Chong KW, Woon CY, Wong MK. Induced membranes e a staged technique of bone grafting for segmental bone loss: surgical technique. J Bone Joint Surg Am. 2011; 93(suppl1):85-91.
12. Wininger D A, Fass R J, Antibiotic-impregnated cement and beads for orthopaedic infection. Antimicrobial agents chemotherapy. 1996; 40(12)2675-2679.
13. Shameem Ahmad, Mukesh Karla, Mariappan Selvamari. Induced membrane formation in a case of infected gap nonunion of radius: case report. Journal of clinical Orthop and trauma 4(2013)147-150.
| How to Cite This Article: R Sivakumar, M Gulam Mohideen, M Chidambaram, T Vinoth, Prahalad Kumar Singhi, V Somashekar. Management of Large Bone Defects in Diaphyseal Fractures by Induced Membrane Formation by Masquelet’s Technique . Journal of Orthopaedic Case Reports 2016 July-Aug;6(3): . Available from: https://www.jocr.co.in/wp/2016/07/10/2250-0685-508-fulltext/ |

[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


