
[box type=”bio”] What to Learn from this Article?[/box]
Simultaneous bilateral neck of femur fractures following electric shock injury is rare, however co-existence of hypovitaminosis-D in the Indian population seems to be probably an emerging threat to the treating orthopaedic surgeon and has to be addressed promptly and effectively.
Case Report | Volume 6 | Issue 3 | JOCR July-Aug 2016 | Page 70-72 | Supreeth Nekkanti, Vijay C, Sujana Theja JS, RaviShankar R, Sumit Raj. DOI: 10.13107/jocr.2250-0685.514
Authors: Supreeth Nekkanti[1], Vijay C[1], Sujana Theja[1], RaviShankar R[1], Sumit Raj[1]
[1]Department of Orthopaedics, JSS Hospital, Mysore, India.
Address of Correspondence
Dr. Supreeth Nekkanti,
No 160, 11th cross, 5th main, 1st stage, NGEF Layout, Nrupatunganagar, Nagarbhavi, Bangalore, Karnataka-560072. India.
E-mail: drsupreethn@gmail.com
Abstract
Introduction: Simultaneous bilateral fractures of the neck of femur is rare. Hypocalcemia, epilepsy, osteoporosis and electrical injuries are known to cause similar injuries.
Case Report: We report a case of a 43-year-old male who sustained an electrical shock injury following which he fell from a height of around 4 feet. Radiological studies confirmed bilateral transcervical neck of femur fracture. Laboratory investigations revealed the patient had extremely low levels of vitamin D (11.1ng/ml). Patient was treated with three 6.5 mm cannulated cancellous screws on each side. Patient had good functional outcome at the end of one year.
Conclusion: We report this case as a rare etiological combination of hypovitaminosis D and electrical injury causing bilateral neck of femur fracture. Such injuries should be diagnosed at the earliest and goal of treatment should be to preserve both the hip joints. Early management would avoid potential complications like non-union and avascular necrosis.
Keywords: bilateral neck of femur fracture, electrocution injury, hypovitaminosis-D
Introduction
Simultaneous bilateral fractures of neck of femur are rare. The reasons behind such injuries are varied. Electrical shock forms an exceedingly rare cause of bilateral neck of femur fracture. Less than ten cases have been reported in our review of literature [1]. The reason for such an injury is due to violent unopposed muscle contractions rather than the trauma of fall per se. We report a case of simultaneous bilateral fractures of neck of femur occurring due to a rare etiological combination of hypovitaminosis-D and electrical shock injury.
Case Report
A 43-year-old male patient presented to the emergency department with a fall from a height of 4 feet. He gave a history of charging his mobile, standing on a shelf of four feet height following which he suffered an electrocution injury. He fell down from the shelf, after which he was unable to stand up on his feet or move his legs due to pain. On examination, his bilateral lower limbs were externally rotated and both hip movements were extremely painful. Radiographic studies confirmed the diagnosis of bilateral transcervical neck of femur (Fig. 1). Investigations revealed his vitamin D levels were low (11.1ng/ml). The patient was taken up for surgery, closed reduction and internal fixation by 6.5 mm cannulated cancellous screws.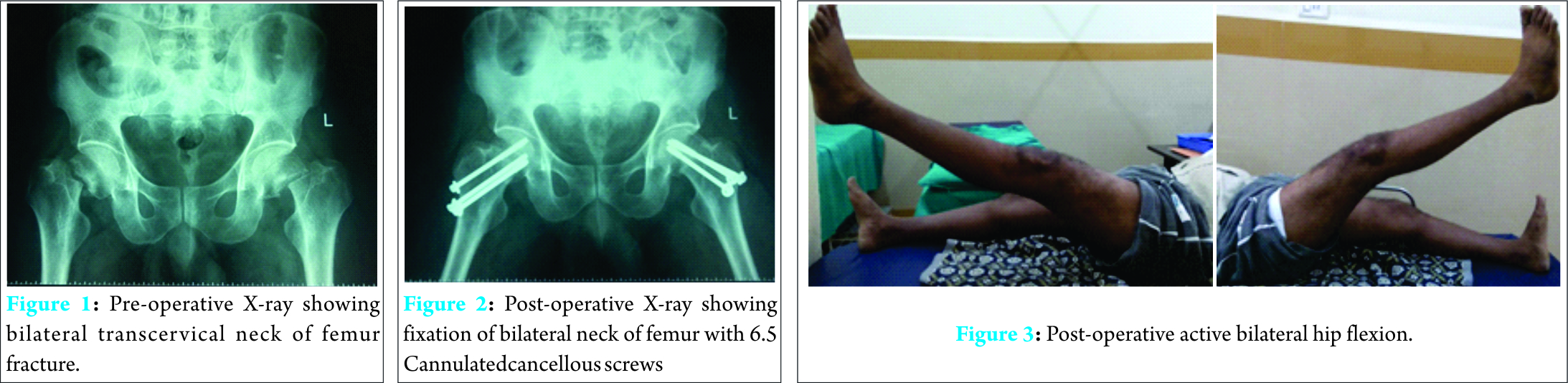
Surgical technique:
The patient was operated on the same day. The fracture was reduced by Leadbetter’s technique and reduction was maintained using traction table. Using the lateral approach, the tensor fascia lata was dissected and the area 2.5 cm distal to the vastus ridge was chosen for inserting three 6.5 mm cannulated cancellous screws with washers. After screws were inserted, reduction was checked again with the aid of C-arm. The traction was released before final tightening of the screws. The left hip was fixed by the inverted triangle pattern of screw fixation, whereas the right hip was fixed with upright triangle pattern of fixation (Fig. 2)
The post-operative period was uneventful. The patient was taught static quadriceps exercises and active knee and ankle range of movements 5 days after surgery. Active hip movements were initiated six weeks after surgery. Patient was ambulated using a four stand walker at the end of 12 weeks. At the end of 16 weeks, patient was independently ambulatory and had good range of movements of both the hips (Fig. 3, 4, 5)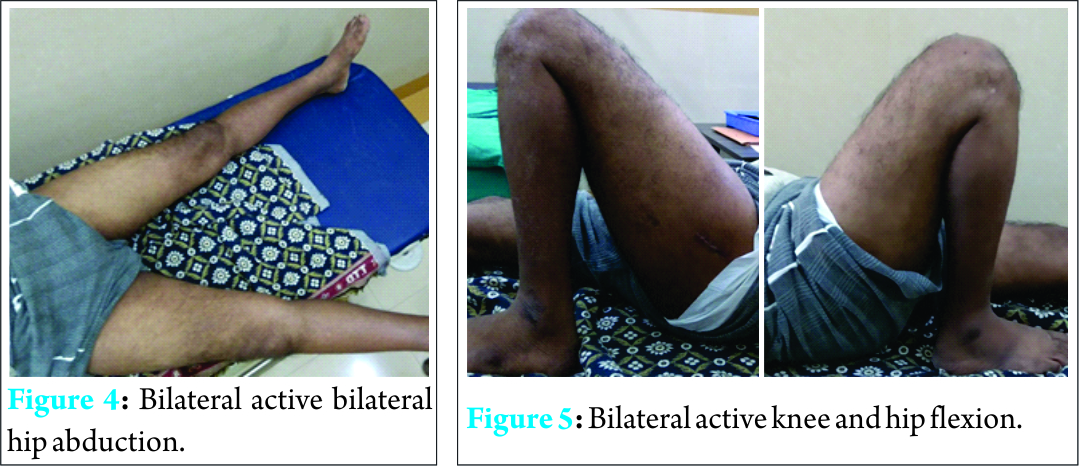
Discussion
Simultaneous bilateral fractures of neck of femur, are extremely rare injuries. Less than ten cases have been reported in our review of literature [1-6]. Most authors equivocally attribute this unique injury due to unopposed violent contractions of the musclesrather than the fall per se. In 1960, Powell explained that the fractures occur specifically during the tonic phase of contractions of the muscles [7]. This is evident by the fact that our patient fell from a height of less than 4 feet. This is not a sufficient force to cause fracture of bilateral neck of femur. In 1956, Andreini suggested that simultaneous contraction of pelvi-trochanteric muscles is the main cause of fractures around the hip following an electrical shock injury [7]. He explained that only these muscles can apply their force irrespective of the position of pelvis and femur. He went on to conclude that if a person sustains an electrical injury when his legs are adducted, it would lead to central dislocation of bilateral hip joints. When the legs are abducted, it would lead to bilateral neck of femur fractures. In 1938, Satta suggested that men are more prone to bilateral neck of femur fractures following an electrical shock due to the fact that muscles are stronger and well-toned as compared to women [7]. Bone is the poorest conductor of electric current among all the living tissues in our body. Consequently, it provides the greatest resistance to flow of electric current resulting in it absorbing all the energy of the conducted current. In experimental studies, it has been observed that muscle contractions result from direct current of at least 20mAand alternating current of 10mA [8]. Authors have suggested that electroconvulsive therapy, drug induced epilepsy, chronic renal failure and metabolic conditions like hypocalcemia, osteomalacia are other causes of similar injuries in order of their frequency of presentation [8-15]. In 1947, Santagali explained that bilateral neck of femur fractures tend to occur in metabolic conditions like osteomalacia and osteoporosis [7]. Our patient had very low levels of serum vitamin D, which could also contribute to the grievous nature of the injury. Accidental electrical injuries are rare and often the patient is unconscious or in a confused state of mind. Initial sequelae of electric shock include thermal myonecrosis which leads to acute renal failure which complicates to cardiac arrest or cardiac arrhythmias. Hence, in the emergency room (ER), the patient must be critically screened for cardiac and renal anomalies. Electrocardiogram with renal function tests with 24 hour monitoring is usually sufficient to rule out such complications [18, 19, 20]. Screening of pelvis, spine and shoulder is essential in order to avoid missing these rare injuries [8,16, 17]. In our review of literature, posterior shoulder dislocations, fractures of the proximal humerus and fracture of scapula have been reported following electric shock injuries due to vigorous muscle contractions around the shoulder[18, 21, 22]. In the forearm, galeazzi and distal radius fractures have been reported [ 18, 23, 24]. In the spine, L4 burst fractures and transient spinal quadraperesis has been reported [18, 25, 26]. If the patient is conscious, a thorough clinical examination should suffice to rule out the above mentioned injuries. In our case, the patient was conscious and unable to lift both legs with painful range of movement of both hips. Hence, it was relatively easy to confirm the diagnosis after radiological studies. If the patient is not conscious, it becomes critical to screen the spine, pelvis and shoulders. Bilateral neck of femur fractures are difficult to treat if not diagnosed early. Hip preservation should be the goal of treatment in young patients such as in our case. We took a decision of fixing both the femurs with three cannulated cancellous screws each. Dynamic hip screw can also be used as an alternative to treat such injuries. In older patients with a sedentary life style, bilateral hemiarthroplasty can be performed as a salvage procedure [7]. Anesthetic complications like difficult intubation due to spasm or persisting cardiac abnormalities like arrhythmias are usually encountered. In such cases, surgery is deferred until the patient is stabilized. In our case no such complication was encountered. Complications like non-union and avascular necrosis are very common if neglected and hence the need to diagnose such injuries at the earliest [7, 8]. Our patient was free of complications at the end of one year follow up. He was ambulatory and had good range of movements of the hip, knee and ankle to continue his normal life.
Conclusion
We report this case as a rare etiological combination of hypovitaminosis D and electrical injury causing bilateral neck of femur fracture. Such injuries should be diagnosed at the earliest and goal of treatment should be to preserve both the hip joints. Early management would avoid potential complications like non-union and avascular necrosis
Clinical Message
The goal of the treatment should be to preserve both the hip joints with prior importance in treating Hypovitaminosis-D, which would help in early healing of fracture and also prevent further pathlogical fractures following trivial trauma.
References
1. Gehlen JMLG, Hoofwijk AGM. Femoral neck fracture after electrical shock injury. Eur J Trauma Emerg Surg 2010;36:491–493.
2. Atkinson RE, Kinnett G, Arnold WD. Simultaneous fractures of both femoral necks, review of the literature and report of two cases. ClinOrthop. 1980;152:284–7.
3. Tompkins GS, Henderson RC, Peterson HD. Bilateral simultaneous fractures of the femoral neck: a case report. J. Trauma1990;30(11):1415–6.
4. Slater RR Jr, Peterson HD. Bilateral femoral neck fractures after electrical injury: a case report and literature review. J Burn Care Rehabil. 1990;11(3):240–3.
5. Shaheen MA, Sabet NA. Bilateral simultaneous fracture of the femoral neck following electrical shock. Injury. 1984;16(1):13–4.
6. Nyoni L, Saunders CR, Morar AB. Bilateral fracture of the femoral neck as a direct result from electrocution shock. CentrAfr J Med.1994;40(12):355–6.
7. Powell HDW. Simultaneous bilateral fractures of the neck of the femur. J Bone Joint Surg Br 1960;42-B(2):236-52.
8. Sohal HS, Goyal D. Simultaneous bilateral femoral neck fractures after electrical shock injury: a case report. Chinese Journal of Traumatology 2013; 16(2):126-8.
9. Annan IH, Buxton RA. Bilateral stress fractures of the femoral neck associated with abnormal anatomy-a case report. Injury 1986;17(3):164-6.
10. Karapinar H, Ozedemir M, Akyol S, et al. Spontaneous bilateral femoral neck fractures in a young adult with chronic renalfailure. ActaOrthopBelg 2003;69(1):82-5.
11. Gerster JC, Charhon SA, Jaeger P, et al. Bilateral fractures of the femoral neck in patients with moderate renal failure receiving fluoride for spinal osteoporosis. Br Med J (Clin Res Ed) 1983;287(6394):723-5.
12. SchröderJ, Marti RK. Simultaneous bilateral femoral neck fractures: case report. Swiss Surg 2001;7(5):222-4.
13. Carrell B, Carrell WB. Fractures in the neck of the femur in children with particular reference to aseptic necrosis. J Bone Joint SurgAm 1941;23(2):225-39.
14. Konforti B, Chokanov K. Simultaneous bilateral nailing by two teams of surgeons in fractures of the femoral neck. Khirurgiia 1956;9(1):75-8.
15. Chadha M, Balain B, Maini L, et al. Spontaneous bilateral displaced femoral neck fractures in nutritional osteomalacia- a casereport. ActaOrthopScand 2001;72(1):94-6.
16. Evans RH, Little K. Fracture due to shock from domestic electricity supply. Injury. 1991;22(3):231–2.
17. Fish RM. Electrical injury, part II: specific injuries. J Emerg Med.2000;18(1):27–34.
18. Stone N III, Karamitopoulos M, Edelstein D, et al. Bilateral Distal Radius Fractures in a 12-Year-Old Boy after Household Electrical Shock: Case Report and Literature Summary. Case Rep Med.2014;2014: 235756
19. Solem L, Fischer RP, Strate RG. The natural history of electrical injury. Journal of Trauma 1977;17(7):487–492.
20. DiVincenti FC, Moncrief JA, Pruitt BA Jr. Electrical injuries: a review of 65 cases. Journal of Trauma. 1969;9(6):497–507.
21. Aktas I, Akgun K. Frozen shoulder development secondary to proximal humerus fracture and supraspinatus tendon tear following electrical injury. Europa Medicophysica. 2007;43(4):469–473.
22. Dumas JL, Walker N. Bilateral scapular fractures secondary to electrical shock. Archives of Orthopaedic and Trauma Surgery 1992;111(5):287–288.
23. Tucciarone L, Sabbi T, Colasanti A, Papandrea S. Colles’ fracture in a girl after fulguration. La PediatriaMedica e Chirurgica 1997;19(1):71–72. (Ita)
24. Hostetler MA, Davis CO. Galeazzi fracture resulting from electrical shock. Pediatric Emergency Care 2000;16(4):258–259
25. Van den Brink WA, van Leeuwen O. Lumbar burst fracture due to low voltage shock. A case report. ActaOrthopaedicaScandinavica. 1995;66(4):374–375.
26. Simon JP, Van Delm I, Fabry G. Comminuted fracture of the scapula following electric shock. A case report. ActaOrthopaedicaBelgica. 1991;57(4):459–460.
| How to Cite This Article: Nekkanti S, Vijay C, Sujana Theja S, RaviShankar R, Raj S. An unusual case of simultaneous bilateral neck of femur fracture following electrocution injury-A case report and review of literature. Journal of Orthopaedic Case Reports 2016 July-Aug: 6(3):70-72. Available from: https://www.jocr.co.in/wp/2016/07/10/2250-0685-514-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


