
[box type=”bio”] What to Learn from this Article?[/box]
Plate fixation and bone grafting can lead to success even in rare, very old, complex and multifocal non- unions.
Case Report | Volume 6 | Issue 3 | JOCR July-Aug 2016 | Page 82-84 | Vikas Padha, Bhanu Awasthi, Dhananjay Singh, Sandeep Kalia. DOI: 10.13107/jocr.2250-0685.524
Authors: Vikas Padha[1], Bhanu Awasthi[1], Dhananjay Singh[1], Sandeep Kalia[1]
[1]Department of Orthopaedics, Dr RPGMC, Tanda, Kangra, Himachal Pradesh. India.
Address of Correspondence
Dr. Vikas Padha,
Assistant Professor, Department of Orthopeadics, Dr RPGMC Kangra At Tanda, Himachal Pradesh. India.
E-mail: drvikaspadha@gmail.com
Abstract
Introduction: A bifocal non-union of shaft of radius associated with ipsilateral non-union shaft of ulna in an adult has not been reported in the literature till date to the best of our knowledge, though few similar cases of fresh fractures have been reported. The case being reported by us is the first of its kind.
Case Presentation: We report a case of bifocal non-union of shaft radius with non-union ipsilateral shaft of ulna in a 48-year-old right handed male along with discussion of alternative treatment options.
Conclusion: We describe an extremely rare and complicated non-union in which our patient got excellent results along with satisfactory functional recovery as a result of appropriate surgical treatment.
Keywords: Bifocal, Non-union, forearm, plating, bone grafting
Introduction
In clinical practice, non-union in fractures of forearm bones is commonly encountered but non-union of bifocal fracture of shaft of radius is rare. We report a case of bifocal non-union of fracture shaft of radius along with non-union of ipsilateral shaft of ulna (with implant failure in case of non-union of fracture ulna). We couldn’t find evidence of any previous reports relating to the surgical treatment of such a non-union in our review of scientific literature. Only the cases like one involving management of fresh trifocal fractures of radius along with fracture mid shaft ulna, two cases of management of fresh segmental fractures of radius and shaft of ulna and one case of management of fresh trifocal ulna fracture with bifocal radius fracture with supracondylar humerus fracture in a child have been reported in the past.
Case Presentation
A 48-year-old right handed male presented to us in the orthopaedics out patient department with chief complaints of deformity in the left forearm and loss of function of left forearm for the last two months. Patient had been earlier operated for bifocal fracture shaft of radius and fracture shaft of ulna by open reduction and internal fixation with square nails 4 years back. According to the patient, the square nail for radius was removed one year after primary surgery because of impingement but no record was available with the patient. Patient, a bus driver by occupation complained of progressive increase in forearm deformity that got aggravated for the last two months prior to seeking consultation in our institution. On examination, there was gross deformity of left forearm with marked wasting and old healed surgical scar marks on dorsum and ulnar border on inspection (Fig. 1 and 2). On palpation, there was painless abnormal mobility at all three fracture sites (two in radius and one in ulna). There was no distal neurovascular deficit. Radiographs revealed bifocal atrophic non-union of radius with non-union of ulnar shaft fracture with broken square nail for ulna in situ (Fig. 3). Patient was subsequently planned for the surgery after the complete workup.
Under regional block, ulna was approached through direct subcutaneous approach. Broken square nail was removed followed by freshening of fracture ends and fixation with 7 Hole 3.5 mm Locking Compression Plate with bone grafting using blocks of cortico-cancellous graft harvested from the iliac crest. Using Thompson’s approach, radial non-unions were exposed, fracture ends at both the non-union sites were freshened followed by fixation with single 10 Hole 3.5 mm Locking Compression Plate after filling the gaps in between fracture ends with blocks of cortico-cancellous bone taken from the iliac crest. Wounds were closed on negative suction drains and above elbow back slab was applied (Fig. 4 and 5). Patient was closely observed for the signs of compartment syndrome but the post operative period was uneventful. After two weeks, skin staples and back slab was removed and patient was put on physiotherapy in the form of wrist and elbow range of motion exercises. At 6 weeks follow up, fracture started showing signs of union and patient was allowed limited activity. At 12 weeks post-operatively, full activities were allowed as fracture had united. At one year follow up, the patient who could not hold anything in his left hand at the time of presenting to us, had resumed his occupation as a bus driver and was now holding steering wheel of bus using same left hand and had good functional and cosmetic results (Fig. 7, 8 and 9), with radiographs showing good consolidation of the fractures (Fig. 6).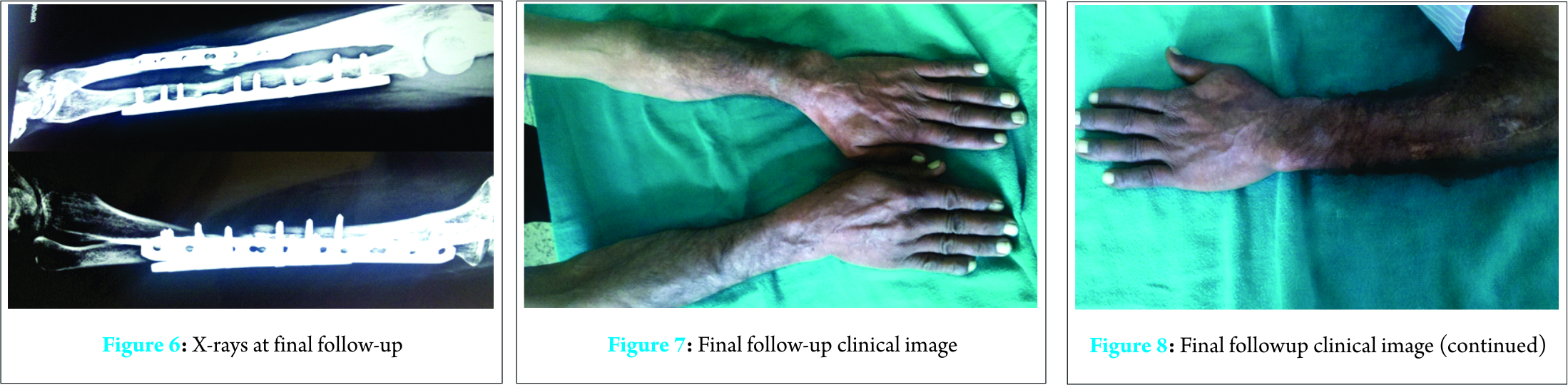
Discussion
Mazin Ibrahim et al [1] reported a fresh case of unilateral, trifocal diaphyseal fracture of radius with mid shaft ulna fracture managed by fixation of bifocal radius fractures with two Titanium Dynamic Compression Plates using Henry’s volar approach to radius and fixation of ulna with Titanium Dynamic Compression Plate as well. In our case, Thompson’s dorsal approach was used for fixation of non-unions of radius to prevent devascularisation of volar aspect of radius and to use old healed surgical scars on dorsum of forearm from previous surgery. We used single long plate instead of two plates to avoid stress shielding. Our further search revealed few more similar cases of fresh trauma .Rafiq et al [2] reported the management of a case of an ipsilateral diaphyseal fracture of radius, ulna and radial head managed with plating of forearm fractures along with radial head replacement. Harsh Raval et al [3] reported management of two fresh cases of segmental complex radius fractures with mid shaft ulna successfully treated by combination of nailing, plating and K-wire fixation. Ravi Mittal and Vijay Sharma [4] reported the management of case of ipsilateral fracture supracondylar humerus with trifocal ulna and bifocal radius. Mseddi et al [5] and Goa et al [6] reported good results with intramedullary devices but in our case, intramedullary fixation had failed and hence plating was preferred. Ring et al [7], in their study of 38 cases of fracture radius and ulna reported successful treatment with plating and autologous cancellous bone grafting. A similar management was carried out in our case. Through this case report, we have highlighted successful management of rare non-union with good functional outcome.
Conclusion
The present case report is the first of its kind emphasizing the fact that the rigid fixation and autologous cortico-cancellous bone grafting should bethe preferred modality of treatment even in such complex non-unions yielding successful outcome.
Clinical Message
Intramedullary implants have high rate of failure in forearm fractures and should be preferentially treated with plating in adults. Non-unions, and especially segmental non-union as seen in our case poses a greater challenge and needs fixation with locking plates with adequate bone grafting. Single plate avoids stress shielding and using same approach as used earlier avoids circumferential periosteal stripping.
References
1. Ibrahim M, Cwilewicz J, Khan OH, Gibbon A. Unilateral, trifocal, diaphyseal fracture of radius with ipsilateral mid-shaft ulna fracture in an adult: A case report. J Med Case Rep 2011; 5:123.
2. Rafiq I, Kumar K, Sutherland KG. Ipsilateral diaphyseal fracture of radius, ulna and radial head: a case report. Internet J OrthopaedicSurg 2006;3:1.
3. Raval H, Panse JB, Amin P, Pandit J. Unilateral, multifocal fracture of radial with ipsilateral mid shaft ulna fracture-Two such unusual and rarely reported cases. JOCR 2015;5(3):22-24.
4. Mittal R, Sharma V. Ipsilateral supracondylar humeral and segmental both bones forearm fracture in a child: a case report .Middle East J Emerg Med 2005;1:3.
5. Mseddi MB , Manicom O, Filippini P, Demoura A, et al. Intramedullary pinning of diaphyseal fractures of both bones forearm in adults: 46 cases. Rev ChirOrthopReparatriceAppar Mot 2008;94:160-167.
6. Goa H, Luo CF, Zhang CQ, Shi HP, et al. Internal fixation of diaphyseal fractures of the forearm by interlocking intramedullary nail: short term results in eighteen patients. J Orthop Trauma 2005;19:384-391.
7. Ring D, Allende C, Jafarnia K, Allende BT, et al. Ununited diaphyseal forearm fractures with segmental defects: plate fixation and autologous cancellous bone grafting. J Bone Joint Surg Am 2004;86(A): 2440-2445.
| How to Cite This Article: Padha V, Awasthi B, Singh D, Kalia S. A very rare Presentation of Bifocal Non Union Radius with Ipsilateral Ulnar Shaft Non Union: Case Report. Journal of Orthopaedic Case Reports 2016 July-Aug;6(3): 82-84. Available from: https://www.jocr.co.in/wp/2016/07/10/2250-0685-524-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


