
[box type=”bio”] What to Learn from this Article?[/box]
Hip dislocation is an orthopedic emergency and its treatment is challenging if associated with ipsilateral fractures.
Case Report | Volume 6 | Issue 5 | JOCR November-December 2016 | Page 44-46 | Abduljabbar Alhammoud, Masson Alnouri, Mahmood Ali Arbash, Abdul Moeen Baco DOI: 10.13107/jocr.2250-0685.624
Authors: Abduljabbar Alhammoud[1], Masson Alnouri[1], Mahmood Ali Arbash[1], Abdul Moeen Baco[1]
[1]Department of Orthopedics, Hamad Medical Corporation, Doha, Qatar.
Address of Correspondence
Dr. Abduljabbar Alhammoud,
Orthopedics Surgery Resident, Hamad Medical Corporation, P.O. Box. 3050, Doha, Qatar.
E-mail: aghammoud85@hotmail.com
Abstract
Introduction: Complex fractures are increasing because of various traumatic mechanisms. They drift from standard classifications, and their treatment is controversial. Of such cases are hip dislocations with associated fractures of the ipsilateral femur.
Case Presentation: This case report describes the condition of a 30-year-old man involved in a motor vehicle collision. Clinical examination, X-rays, and computed tomography scan revealed a posterior hip dislocation with an ipsilateral femoral head and mid-shaft fractures. The patient was treated by closed reduction of hip dislocation using a temporarily applied external fixator followed by intramedullary nailing of the femoral shaft. Achieving a closed reduction is a challenge with ipsilateral fractures but it should be favored over open reduction due to a lower risk of complications. The type of femoral head fracture, in this case, may have aided in an easier reduction.
Conclusion: Hip dislocation is an orthopedic emergency and its treatment is challenging if associated with ipsilateral fractures. The decision of a closed versus an open approach should be made after considering the management plans of other injuries.
Keywords: Hip dislocation, Ipsilateral femur fractures, external fixator.
Introduction
There has been a significant increase in the complexity of fractures due to the increasing variety of traumatic mechanisms such as high-speed collisions, falls from heights, construction related high-energy injuries, and more. These fractures tend to drift from the standard classification systems, and their treatment is usually controversial because of varying outcomes. One such example is hip dislocations associated with head [1], neck [2], intertrochanteric [3], shaft [4], distal femur fractures [5], or knee dislocation [6]. In this report, we study the case of a 30-year-old man who sustained a posterior hip dislocation with concomitant ipsilateral femur head and shaft fractures. Only one similar case was previously published in the literature [7], and there were some differences noted between the two cases.
Case Report
A 30-year-old man presented to the emergency trauma room following a motor vehicle collision in which he was the front-seat unrestrained passenger. At the time of presentation, the patient was vitally stable, conscious, alert, oriented with a Glasgow Coma Scale 15/15 [8]. A cervical collar and spinal board were applied by the paramedics at the scene. The trauma surgery team assessed the patient initially and implemented the advanced trauma life support protocol [9]; he was deemed to be hemodynamically stable with no other systemic injuries. The patient was, however, complaining of moderate left hip and thigh sharp pain as well as left shoulder pain. On examination, he was noted to have abducted, shortened and internally rotated left lower limb. Active and passive movements of the left thigh were not possible due to pain with no neurovascular deficits detected distally. There were no significant examination findings of the left shoulder and upper limb. X-rays of the pelvis and left femur revealed a posterior fracture dislocation of left femoral head with an ipsilateral femoral mid-shaft fracture and a computed tomography (CT) scan of the pelvis showed large and small fracture fragments within the acetabulum originating from the medial aspect of the femoral head (Fig. 1). A shoulder X-ray also revealed a non-displaced left scapular body fracture. An attempt of left hip closed reduction was made while the patient was still in the emergency department and it was, however, unsuccessful.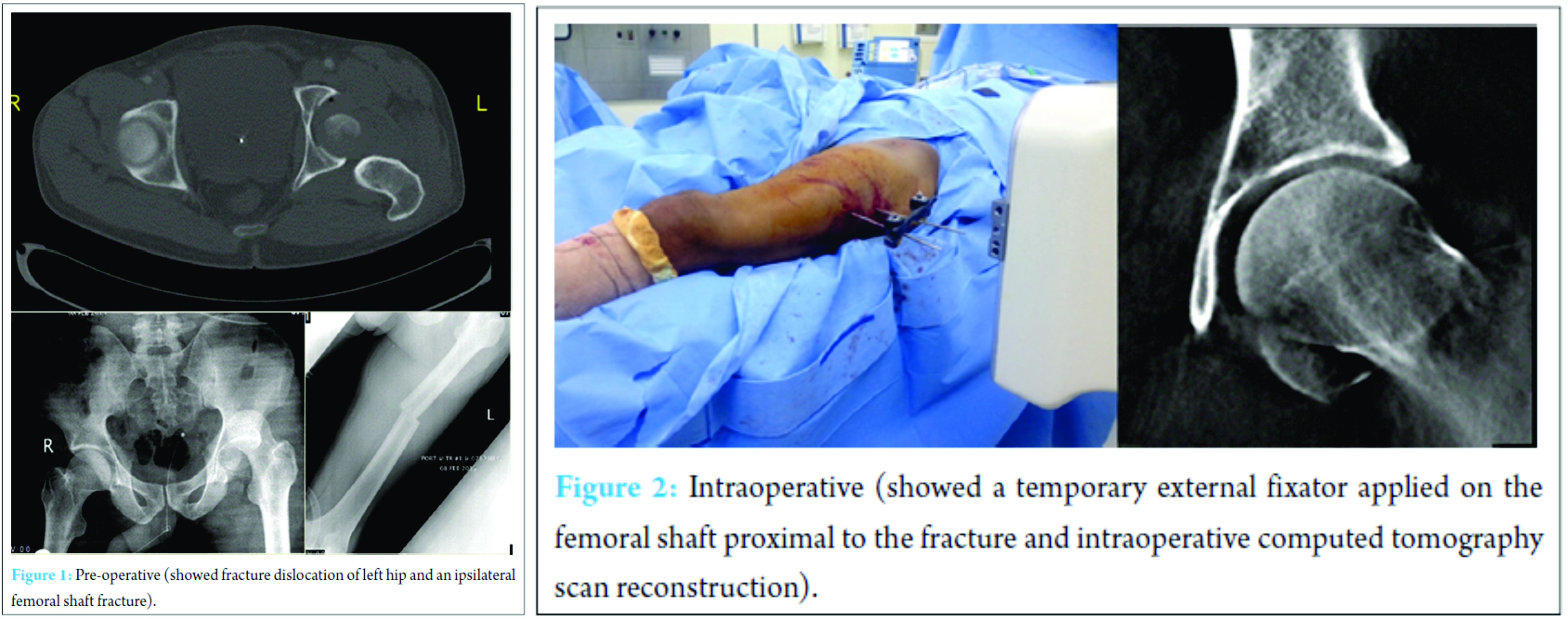
After being cleared by the trauma team, the patient was admitted to the orthopedic service with a working diagnosis of left posterior hip dislocation with a Pipkin Type 1 ipsilateral femoral head fracture [10] and an ipsilateral femoral shaft fracture. The patient was taken to the operating theater for closed versus open reduction and intramedullary nailing of the left femur. Within 5 h of his injury, the patient underwent closed reduction of the left hip with the aid of a temporary external fixator applied on the femoral shaft proximal to the fracture (Fig. 2).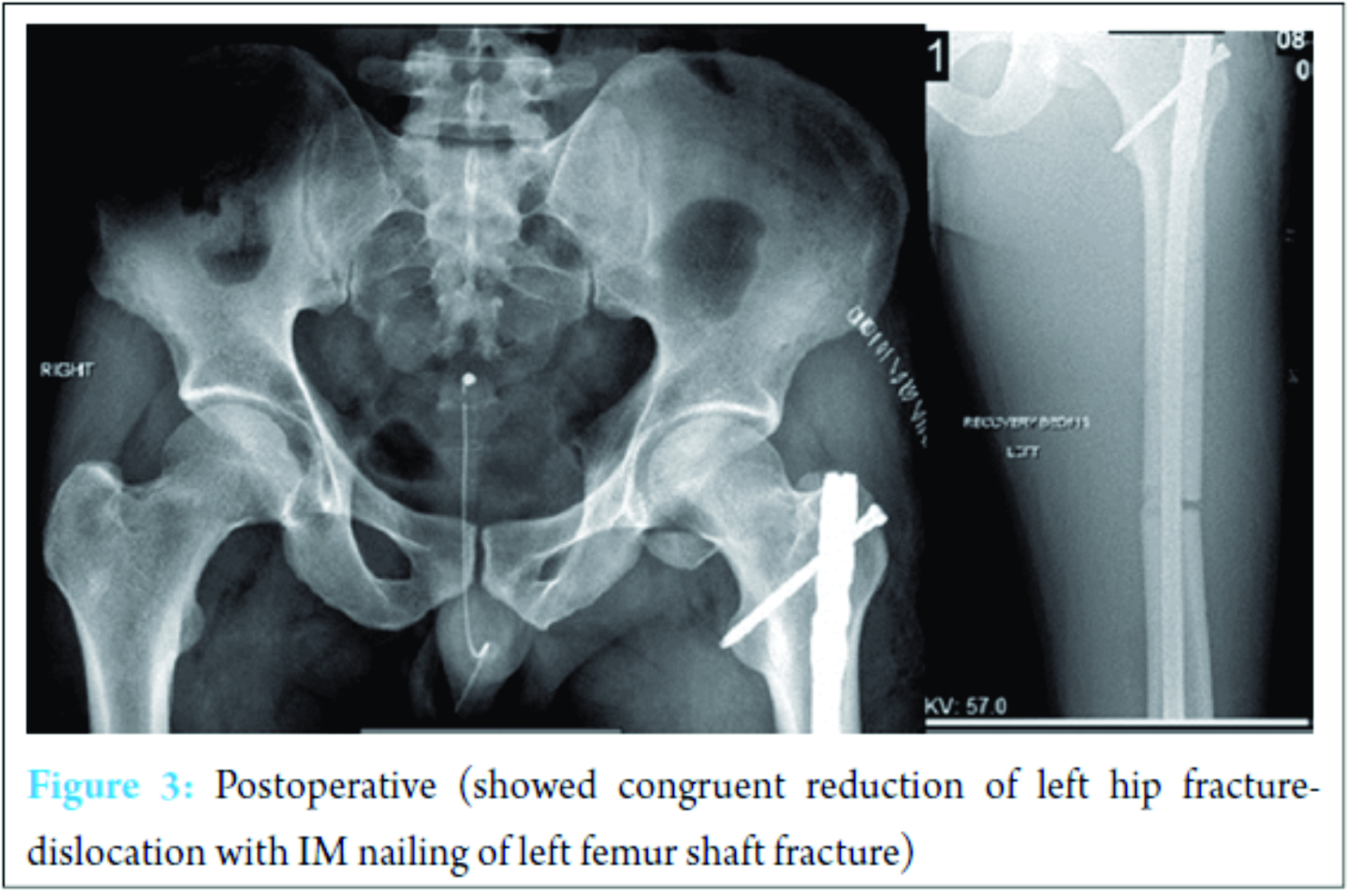 The external fixator rod was used as a handle, and the reduction was successful after the first attempt, as confirmed by the C-arm and CT reconstruction (Fig. 2). Subsequently, the external fixator was removed, and intramedullary nailing of the left femur was carried out. After completion of the procedure, the left hip was examined and found to be stable with the femoral head fragment not affecting the movement. The patient was discharged after 3 days with a clean, dry wound and full weight bearing ambulation as tolerated. Unfortunately, he was lost to follow-up and attempts to contact the patient were unsuccessful.
The external fixator rod was used as a handle, and the reduction was successful after the first attempt, as confirmed by the C-arm and CT reconstruction (Fig. 2). Subsequently, the external fixator was removed, and intramedullary nailing of the left femur was carried out. After completion of the procedure, the left hip was examined and found to be stable with the femoral head fragment not affecting the movement. The patient was discharged after 3 days with a clean, dry wound and full weight bearing ambulation as tolerated. Unfortunately, he was lost to follow-up and attempts to contact the patient were unsuccessful.
Discussion
The primary challenge, in this case, was achieving closed reduction of the hip dislocation; this was particularly difficult due to the inability to transmit the force needed for reduction through to the hip and the difficulty controlling the thigh. Both of these problems were caused by the concomitant fracture in the femoral shaft. This necessitated the use of other indirect methods of reduction like the temporary external fixator (Fig. 3). These challenges were also faced by other treating surgeons in similar cases, and each team was able to achieve the reduction by closed manipulation or manual traction maneuvers [11], indirect reduction with the aid of external tools such as a loop [4] and open reduction [7]. Early reduction of the dislocation is important to prevent significant complications associated with late reduction like osteonecrosis and subsequent hip arthritis [12]. Moreover, closed or indirect reduction is favored over open reduction especially if there is no plan for internal fixation of the acetabulum or proximal femur because of the significant risks involved with open surgery which include but is not limited to: Sciatic nerve palsy, heterotopic ossification, avascular necrosis, blood loss and infection [10]. It is worth noting that in the similar case described by Galois et al.; the femoral head fracture was suprafoveal Pipkin Type 2 [7] while in our case it was infra foveal Pipkin Type 1. The latter type may have contributed to an easier reduction which is possible through closed methods, while in the former case the fractured fragment may have necessitated open reduction, due to a mechanical block inhibiting reductions by closed methods, and internal fixation to restore and maintain the articular congruency and the weight bearing surface of the hip.
Conclusion
Traumatic hip dislocation is a significant orthopedic emergency and its treatment is more challenging if the dislocation is associated with other concomitant ipsilateral fractures. Management should start with emergent reduction, and the treating orthopedic surgeon should make the decision of a closed versus an open approach after taking into consideration the other injuries and fractures and considering their definitive management plan.
Clinical message
Hip dislocation is an orthopedics emergency and requires urgent reduction. It can be challenging when coupled with an ipsilateral femur fracture. The use of indirect reduction instrument, such as an external fixator, may preclude an open procedure which will prevent surgical complications.
References
1. Stannard JP, Harris HW, Volgas DA, Alonso JE. Functional outcome of patients with femoral head fractures associated with hip dislocations. Clin Orthop Relat Res 2000;(377):44-56.
2. Dummer RE, Sanzana ES. Case report hip dislocations associated with ipsilateral femoral neck fracture. Int Orthop 1999;1:353-354.
3. Jamshidi MH, Mirkazemi M, Birjandinejad A. Posterior hip fracture-dislocation associated with ipsilateral intertrochantric fracture; A rare case report. Arch Bone Joint Surg 2014;2(1):75-78.
4. Verdonk R, de Smet L. Hip dislocation combined with femoral shaft fracture. Two cases treated with the Lardennois hoop. Acta Orthop Scand 1984;55(2):185-186.
5. Zhen P. Traumatic posterior hip dislocation with an ipsilateral comminuted femoral intertrochanteric fracture: a case report. Orthop Surg 2013;5(3):219-221.
6. DuBois B, Montgomery WH Jr, Dunbar RP, Chapman J. Simultaneous ipsilateral posterior knee and hip dislocations: case report, including a technique for closed reduction of the hip. J Orthop Trauma 2006;20(3):216-219.
7. Galois L, Pauchot J, Pfeffer F, Kermarrec I, Traversari R, Mainard D, et al. Modified shoelace technique for delayed primary closure of the thigh after acute compartment syndrome. Acta Orthop Belg 2002;68(1):63-67.
8. Matis G, Birbilis T. The – A brief review. Past, present, future. Acta Neurol Belg 2008;108(3):75-89.
9. Radvinsky DS, Yoon RS, Schmitt PJ, Prestigiacomo CJ, Swan KG, Liporace FA. Evolution and development of the advanced trauma life support (ATLS) protocol: A historical perspective. Orthopedics 2012;35(4):305-311.
10. PIPKIN G. Treatment of grade IV fracture-dislocation of the hip. J Bone Joint Surg Am 1957;39-A(5):1027-1042.
11. Alho A. Concurrent ipsilateral fractures of the hip and femoral shaft: a meta-analysis of 659 cases. Acta Orthop Scand 1996;67(1):19-28.
12. Sanders S, Tejwani N, Egol KA. Traumatic hip dislocation – A review. Bull NYU Hosp Jt Dis 2010;68(2):91-96.
| How to Cite This Article: Alhammoud A, Alnouri M, Arbash MA, Baco AM. Posterior Hip Dislocation with Ipsilateral Femoral Head and Shaft Fracture – Using a Temporary External Fixator as a Method for Closed Reduction. Journal of Orthopaedic Case Reports 2016 Nov-Dec;6(5):44-46. Available from: https://www.jocr.co.in/wp/2016/11/10/2250-0685-624-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


