
[box type=”bio”] What to Learn from this Article?[/box]
Early intervention for metallosis of implant can prevent rapid progression of cup loosening.
Case Report | Volume 7 | Issue 1 | JOCR January – February 2017 | Page 82-86| Devendra Lakhotia, Prashant Kumar. DOI: 10.13107/jocr.2250-0685.700
Authors: Devendra Lakhotia[1], Prashant Kumar[2]
[1] Department of Orthopaedics, Institute for Medical Sciences and Research Centre, Jaipur National University, Jagatpura, Jaipur, Rajasthan, India.
[2] Department of Orthopaedics, Trauma Centre, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
Address of Correspondence
Dr. Devendra Lakhotia,
Department of Orthopaedics, Institute for Medical Sciences and Research Center, Jaipur National University, Jagatpura, Jaipur, Rajasthan, India.
E-mail: drdevendra.ortho@gmail.com
Abstract
Introduction: Pseudotumor is not an uncommon complication after total hip arthroplasty (THA). This can occur in relationship to different bearing surfaces of head and liner ranging from soft to hard articulation. There is wide spectrum of presentation from asymptomatic to implant failure.
Case Report: We report a case of pseudotumor formation with acetabular cup aseptic loosening after revision ceramic on metal hip arthroplasty. The patient underwent pseudotumor excision and re-revision complex arthroplasty procedure using trabecular metal shell and buttress with ceramic on polyethylene THA.
Conclusion: The surgeon should aware of this complication during a presentation in revision cases to prevent rapid progression of cup loosening, and to intervene early to avoid complex arthroplasty procedures.
Keywords: Arthroplasty, ceramics, metals, polyethylene.
Introduction
Pseudotumor is abnormal periprosthetic soft tissue reaction [1] developed in relation to both metal-on-polyethylene total hip arthroplasty (THA) due to polyethylene debris [2] and metal-on-metal (MoM) THA due to metal debris [3,4]. These lesions are non-neoplastic lesions believe to worsen progressively and resulted in both bone and soft tissue extensive destruction [1]. Pseudotumor is increasingly associated to THA with recent studies incidence ranging from 0.27% to 5% [5, 6]. To overcome the adverse issue of metal ion release of MoM, other hard bearings with improved quality were introduced such as ceramic-on-ceramic (CoC) and ceramic-on-metal (CoM) couples to minimize bearing surface wear. CoM have had limited clinical data with short duration of follow-up with high variation in the wear performance [7, 8, 9]. We report a case of pseudotumor formation one year after revision CoM THA. At the time of initial presentation, the patient has mild discomfort with well-fixed implants. The patient underwent pseudotumor formation and rapid aseptic loosening, and managed with complex re-revision arthroplasty with pseudotumor excision. On the basis of clinical findings, imaging studies, increase serum metal ions, intraoperative findings of metallosis and histopathology, we believed pseudotumor formation in this case of revision CoM THA. The patient informed consent was taken for the purpose of publication of the case.
Case Report
A 50-year-old female, department store salesperson by profession, with idiopathic bilateral avascular necrosis, underwent primary left hip THA in 2003 at an outside institution 3 years before evaluation at our hospital presented with worsening right hip pain. Radiographs demonstrated secondary osteoarthritis right hip for which cementless ceramic on polyethylene (CoP) THA was done. On the left side, there was well functioning THA without evidence of any loosening. Review of operative record identified components as cementless metal-on-polyethylene (MoP) THA on left side. The posterolateral incision at left hip was well healed with no evidence of any infection. In 2011, the patient started gradual onset of pain in the left hip. Radiographs and computed tomography (CT) scan demonstrated polyethylene wearing with aseptic loosening of both acetabular and femoral components. The patient underwent revision cementless CoM THA left side in 2011 using 54 mm pinnacle acetabular shell, cobalt chromium metal liner, 36 mm Biolox delta ceramic head, S-ROM titanium alloy femoral stem with titanium sintered proximal sleeve (Depuy, Jhonson and Jhonson co., Warsaw, IN). On the acetabular side allo chip bone graft was used for osteolytic lesions, encirclage wiring done for greater trochanter. Intraoperative findings were loosening of femoral stem and acetabular cup along with mild metallosis on acetabulum and femoral side. Postoperative period was eventless with substantial improvement in function. Acetabular cup inclination and anteversion angle were 45° and 20° respectively estimated from plain radiograph. Femoral anterversion was 15° with normal stem alignment. At 6-week follow-up, the patient was made partial weight bearing increasing to full weight bearing with an assistive device and active abduction over a 6-week period.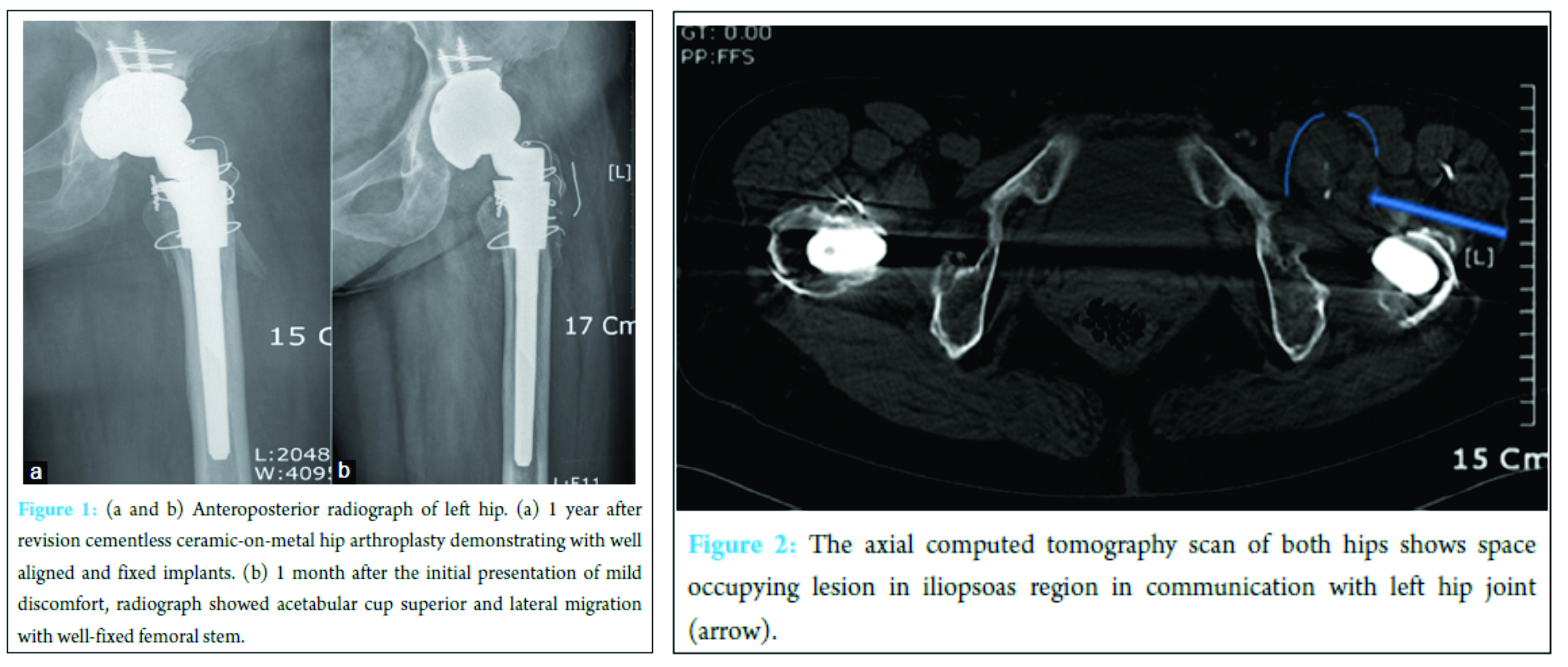
After 1 year of follow-up in 2012, patient complaint of mild discomfort in the groin in the left inguinal region. On examination soft swelling, non-tender, 2 cm × 3 cm size with no signs of inflammation was present in inguinal region. Radiographs showed normal alignment and position of hip prosthesis with no signs of loosening (Fig. 1a). Ultrasonography suggestive of cystic lesion in illiopsoas area in the left anterior hip (3.76 cm × 3.12 cm × 2.95 cm) suspected to be iliopsoas bursitis. Serum inflammatory markers and complete blood counts were within normal limits. Clinical examination showed a painless normal range of motion at left hip. The patient was kept under observation after refusal for ultrasonography-guided aspiration.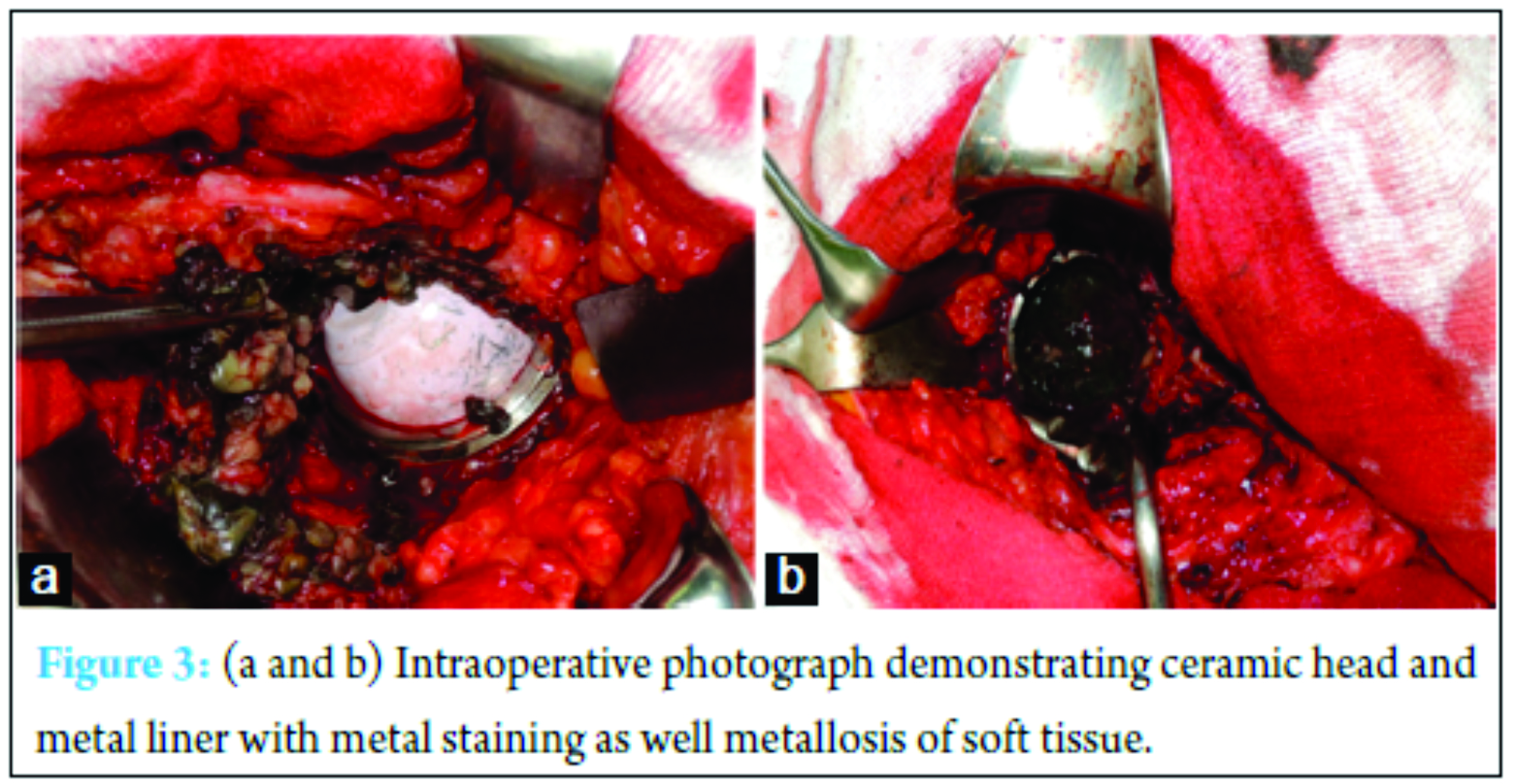
After one month, she complains left groin and thigh pain, limping followed by impaired ambulation in few days. The patient showed an increase in size of iliopsoas cystic lesion. Follow-up radiographs showed signs of acetabular cup superior and lateral migration, increased inclination angle with evidence of loosening and well-fixed femoral stem (Fig. 1b). CT scan showed well circumscribed cystic lesion around the left hip with an expansion of in iliopsoas region (Fig. 2). CT scan also showed the superior segmental defect in the acetabulum along with loosening of acetabular cup. Positive radioisotope bone scan indicates acetabular loosening. Serum C-reactive protein was 0.6 mg/Dl, and erythrocyte sedimentation rate was 28 mm/h. Her complete blood count was normal. Serum cobalt and chromium was significantly raised (serum Co = 2.4 µg/L, serum Cr = 22.5 µg/L).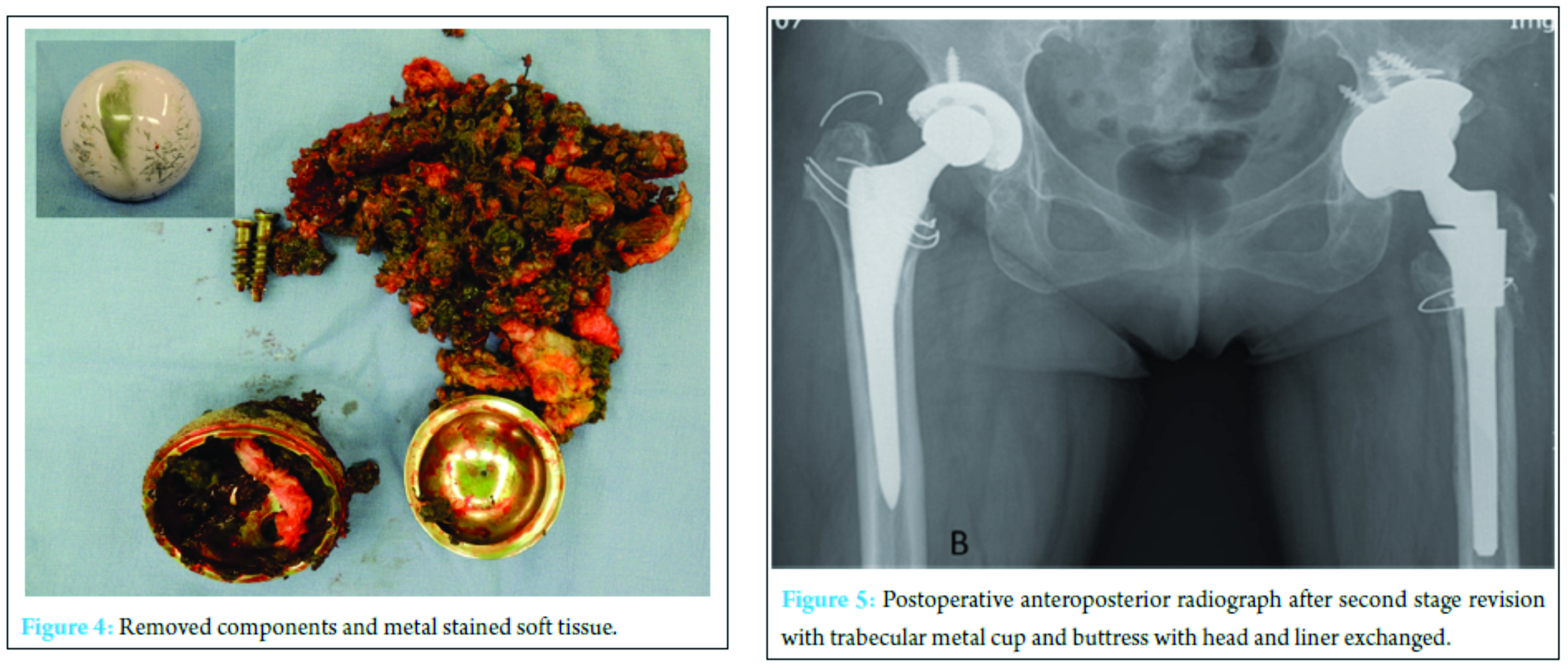
Given the clinical and imaging findings, combined with a history of CoM THA, it was felt that patients symptoms were likely aseptic loosening of acetabular cup with local soft tissue response due to elevated serum metal ions. Surgical exploration with revision THA for loosened implant was discussed with patient. The patient underwent revision surgery using posterolateral approach. The pseudotumor and surrounding inflamed synovitis sac was excised. The cystic soft tissue extended to hip joint was stained with features suggestive of metallosis (Fig. 3). Hip was dislocated and loosened acetabular cup along with cobalt-chromium liner was removed. There is corrosive wear at the metal liner with large “black stripe” across the top of retrieved ceramic femoral head (Fig. 4). The proximal femoral sleeve and the femoral taper showed no corrosion or wear. The femoral stem with proximal sleeve was well fixed with no evidence of corrosion.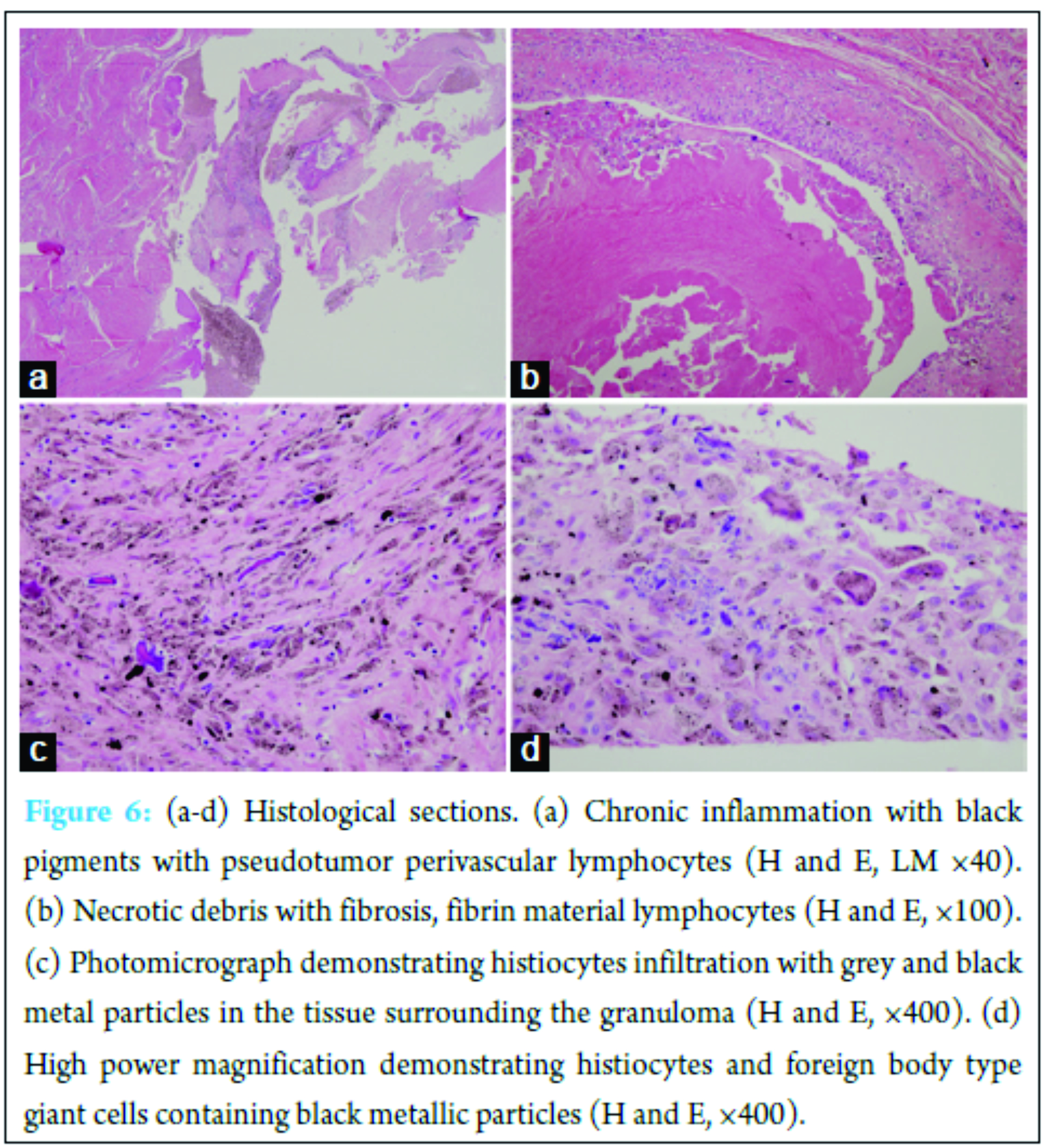
The intraoperative frozen section of mass showed less than 5 polymorphonuclear leukocytes per high-power field in all the three specimens. Intraoperative dark gray colored fluid analysis was done with 58% polymorphonuclear, 39% lymphocytic, and 3% mononuclear cells. After aggressive debridement of metallic and necrotic tissue, acetabular cavitary defects were filled with mixed autogenous bone graft and allograft bone chips bone. On the acetabular side, the patient was revised with 52 mm trabecular metal shell (52 mm) with metal buttress (Fig. 5) to address the superior bone defect (zimmer, warsaw, Indiana, USA). Highly cross-linked polyethylene liner was applied with 32 mm biolox delta ceramic femoral head (Depuy, Jhonson and Jhonson co., Warsaw, IN).
Operative cultures for soft tissue and fluid were both negative for infection. Histopathology was consistent with metallosis. For each tissue fragment, sections were routinely stained with hematoxylin and eosin and examined with light microscopy. On microscopic examination, the inner surface covered with eosinophilic fibrinoid material with local fibrotic tissue. The histopathology analysis supports morphology consistent with the metallosis as an inflammatory response to metal particles. It revealed abundant lymphocytes, histiocytes, occasional plasma cells, foreign body type giant cells, and black metal particles (Fig. 6a-d). After 6 weeks of partial weight bearing, the patient was fully mobilized with full weight bearing over 6-week period. At 6 month repeat serum metal ion analysis showed decrease level with cobalt and chromium levels of 1.3, 2.54 µg/L, respectively. The recent cobalt and chromium measurements were 0.66 and 0.42 µg/L, respectively. The patient with continued improvements in function with full weight bearing walking at last follow-up with Harris hip score of 87 compared with 58 preoperatively.
Discussion
The use of MoM bearing is associated with elevated levels of serum metal ions [3, 10] with local effects (metallosis and local soft tissue reaction) [6] and systemic effects [11]. The use of MoM articulations has decreased, and other hard on hard bearings such as CoC and CoM have been increasingly used. Although CoC is associated with low wear rates but breakage and squeaking are still a concern. The in vitro studies showed reduce in wear in CoM bearing surface [12, 13]. At the same time, there is the difference in literature between wear and metal ion release in CoM with limited clinical data [8, 9, 14]. Few reports showed relation between head – neck, modular neck, and stem-sleeve corrosion with the increased incidence of metal hypersensitivity reactions [15, 16]. Patient-related factor like female [17] and surgeon related factor like suboptimal component positioning [18] more often involved in the pseudotumor. However, all the three hard bearing (CoC, CoM, MoM) showed increased wear with edge loading, CoM bearings demonstrated lower wear compared with MoM [12]. Two case reports describe the pseudotumor formation around the CoM bearing after primary arthroplasty with abnormal acetabular cup positioning [19, 20]. To best of our knowledge, our case report is first to describe pseudotumor formation with rapid loosening, after well aligned and positioned revision CoM THA; and managed with complex re-revision arthroplasty. Initial presentation of symptoms in our case occurred one year after the revision surgery. This duration is short in comparison to soft tissue reaction in MoP bearing ranging from 3 to 26 years [21]. However, we observed excessive acetabular inclination, superior and lateral migration of cup, and loosening correlated with the increase symptoms of pain and increase of soft tissue swelling in inguinal region. We observed superior acetabular segmental defect in CT scan. The initiating factor in our case would be pseudotumor followed by rapid loosening. After loosening there was an increase in edge loading. The symptoms increase rapidly followed by increased in size of pseudotumor indicating vicious cycle of rapid loosening and metallosis. In the management of pseudotumor, non-metal bearing is indicated during revision surgery [5] and we revised our case with CoP. But still, the presence of modular titanium alloy stem with sleeve, porous trabecular metal shell and metal buttress [22], patient with the serum metal ions need close follow-up. This CoM bearing needs to be studied more thoroughly and testing with emphasis on design and material of the bearing surface. The clinical data with component position and serum metals level in the long-term follow-up are necessary.
Conclusion
Pseudotumor is not an uncommon complication after THA. This can occur in relationship to different bearing surfaces of head and liner. Treating physician should be aware of this condition so that prompt diagnosis and treatment can be carried out. Patients with index revision surgery due to aseptic loosening may require subsequent re-revision due to loosening. Loosening in such cases will increase edge loading, hence more severe metallosis and rapid loosening requiring complex arthroplasty procedure.
Clinical Message
Even mild signs and symptoms of soft tissue reaction should be aggressively investigated for metallosis of implant in the absence of any radiographic loosening. The surgeon should aware of this complication during a presentation in revision cases to prevent rapid progression of cup loosening.
References
1. Daniel J, Holland J, Quigley L, Sprague S, Bhandari M. Pseudotumors associated with total hip arthroplasty. J Bone Joint Surg Am 2012;94(1):86-93.
2. Griffiths HJ, Burke J, Bonfiglio TA. Granulomatous pseudotumors in total joint replacement. Skeletal Radiol 1987;16(12):146-152.
3. Pandit H, Glyn-Jones S, McLardy-Smith P, Gundle R, Whitwell D, Gibbons CL, et al. Pseudotumours associated with metal-on-metal hip resurfacings. J Bone Joint Surg Br 2008;90(7):847-851.
4. Madan S, Jowett RL, Goodwin MI. Recurrent intrapelvic cyst complicating metal-on-metal cemented total hip arthroplasty. Arch Orthop Trauma Surg 2000;120(9):508-510.
5. Campbell P, Shimmin A, Walter L, Solomon M. Metal sensitivity as a cause of groin pain in metal-on-metal hip resurfacing. J Arthroplasty 2008;23(7):1080-1085.
6. Kwon YM, Ostlere SJ, McLardy-Smith P, Athanasou NA, Gill HS, Murray DW. “Asymptomatic” pseudotumors after metal-on-metal hip resurfacing arthroplasty: prevalence and metal ion study. J Arthroplasty 2011;26(4):511-518.
7. Williams S, Schepers A, Isaac G, Hardaker C, Ingham E, van der Jagt D, et al. The 2007 otto aufranc award. Ceramic-on-metal hip arthroplasties: a comparative in vitro and in vivo study. Clin Orthop Relat Res 2007;465:23-32.
8. Isaac GH, Brockett C, Breckon A, van der Jagt D, Williams S, Hardaker C, et al. Ceramic-on-metal bearings in total hip replacement: whole blood metal ion levels and analysis of retrieved components. J Bone Joint Surg Br 2009;91(9):1134-1141.
9. Reinders J, Sonntag R, Heisel C, Reiner T, Vot L, Kretzer JP. Wear performance of ceramic-on-metal hip bearings. PLoS One 2013;8(8):e73252.
10. Korovessis P, Petsinis G, Repanti M, Repantis T. Metallosis after contemporary metal-on-metal total hip arthroplasty. Five to nine-year follow-up. J Bone Joint Surg Am 2006;88(6):1183-1191.
11. Tower SS. Arthroprosthetic cobaltism: neurological and cardiac manifestations in two patients with metal-on-metal arthroplasty: a case report. J Bone Joint Surg Am 2010;92(17):2847-2851.
12. Williams S, Isaac G, Porter N, Fisher J, Older J. Long-term radiographic assessment of cemented polyethylene acetabular cups. Clin Orthop Relat Res 2008;466(2):366-372.
13. Firkins PJ, Tipper JL, Ingham E, Stone MH, Farrar R, Fisher J. A novel low wearing differential hardness, ceramic-on-metal hip joint prosthesis. J Biomech 2001;34(10):1291-1298.
14. Valentí JR, Del Río J, Amillo S. Catastrophic wear in a metal-on-ceramic total hip arthroplasty. J Arthroplasty 2007;22(6):920-922.
15. Hsu AR, Gross CE, Levine BR. Pseudotumor from modular neck corrosion after ceramic-on-polyethylene total hip arthroplasty. Am J Orthop (Belle Mead NJ) 2012;41(9):422-426.
16. Huot Carlson JC, Van Citters DW, Currier JH, Bryant AM, Mayor MB, Collier JP. Femoral stem fracture and in vivo corrosion of retrieved modular femoral hips. J Arthroplasty 2012;27(7):1389-1396.e1.
17. Mont MA, Schmalzried TP. Modern metal-on-metal hip resurfacing: important observations from the first ten years. J Bone Joint Surg Am 2008;90 Suppl 3:3-11.
18. Harper GD, Bull T, Cobb AG, Bentley G. Failure of the ring polyethylene uncemented acetabular cup. J Bone Joint Surg Br 1995;77(4):557-561.
19. Deshmukh AJ, Rathod PA, Rodgers WH, Rodriguez JA. Early failure of a ceramicon metal total hip arthroplasty: A case report. JBJS Case Connect 2012;2(2):e25.
20. Koper MC, Mathijssen NM, van Ravenswaay HH, Witt F, Morlock MM, Vehmeijer SB. Pseudotumor after bilateral ceramic-on-metal total hip arthroplasty-A case report JBJS Case Connect 2014;4:e25.
21. Carli A, Reuven A, Zukor DJ, Antoniou J. Adverse soft-tissue reactions around non-metal-on-metal total hip arthroplasty – A systematic review of the literature. Bull NYU Hosp Jt Dis 2011;69 Suppl 1:S47-S51.
22. Potter HG, Ho ST, Altchek DW. Magnetic resonance imaging of the elbow. Semin Musculoskelet Radiol 2004;8(1):5-16.
| How to Cite This Article: Lakhotia D, Prashant K. Pseudotumour Complicated by Implant Loosening One Year After revision Ceramic on Metal Total Hip Arthroplasty: A Case Report. Journal of Orthopaedic Case Reports 2017 Jan-Feb ;7(1): . Available from: https://www.jocr.co.in/wp/wp-content/uploads/24.-2250-0685.700.pdf |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


