
Hamulus stress fracture is an uncommon sports injury and hasn’t been reported in a cricketer till date; if the clinician is not aware of this entity, then it is very easy to miss the diagnosis or to misdiagnose it!
Dr. Rakesh John,
Department of Orthopaedics, Postgraduate Institute of Medical Education & Research, Sector 12, Chandigarh – 160 012, India.
E-mail: rakeshjohn23@gmail.com
Introduction: Hamulus fractures are uncommon injuries constituting 2-4% of carpal fractures and are usually reported in athletes. Stress fractures of hamulus are even rarer and very few cases have been reported till date. In this case report, we present the first documented case of stress fracture of hamulus in a cricket batsman and review the existing literature on hamulus fractures, both acute and stress fractures, in sportspersons in general.
Case Report: A 23-year-old, right-handed, cricket batsman presented with pain in the hypothenar region of his left hand of 7 weeks duration. The pain typically worsened during batting, and he had difficulty in gripping the bat. Plain radiographs were largely inconclusive; magnetic resonance images, however, demonstrated a stress fracture of the hamate hook. The patient was put on conservative management, and his bat grip was modified. He recovered completely within 12 weeks and went back to playing professional cricket.
Conclusions: Hamulus stress fractures should be considered in cricketers presenting with chronic, non-traumatic, and ulnar-sided hand pain. The nonleading hand is more likely to be involved in a batter, as seen in other sports with a double haSnd grip. Nonoperative treatment, change of grip and adequate rehabilitation give good outcomes in most cases.
Keywords: Hamulus, stress fracture, cricket, batsman.
Stress fracture of the hamulus (hook of hamate) is extremely rare with only a few cases having been reported in literature [1,2,3,4]. We present a rare case of stress fracture of the hamulus in a right-handed, club cricket batsman. To the best of our knowledge, this is the first case report of a stress fracture of hamulus in cricketer players till date.
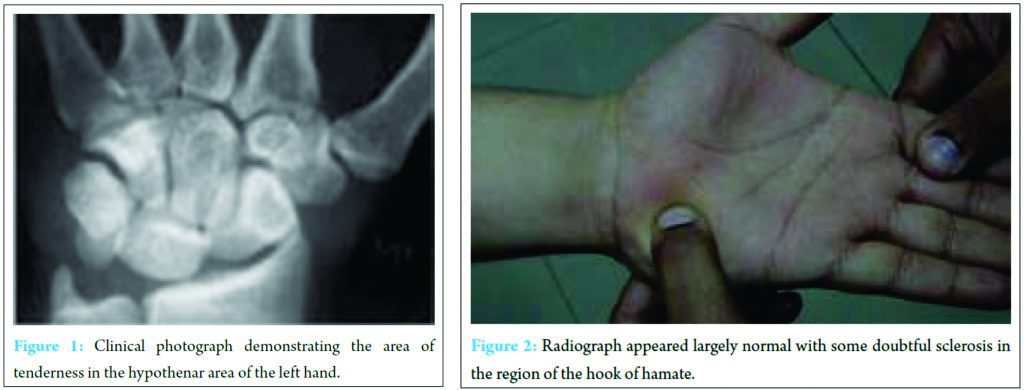
A 23-year-old club team cricketer, who was a right-handed batsman, presented to us with pain in the ulnar side of the left wrist and in the hypothenar area (nondominant hand) since 7 weeks; this was insidious in onset and gradually progressive in intensity. He had no definite history of any acute trauma to this region. Pain typically worsened during batting, and he had difficulty in gripping the bat, and could not execute powerful strokes. On clinical examination, he had deep point tenderness over the hook of the hamate region (Fig. 1). There was no swelling in the region; but grip strength was reduced compared to the opposite side. No symptoms of ulnar nerve compression were elicited. Plain radiographs revealed a sclerotic area in the hamate but were largely inconclusive (Fig. 2).
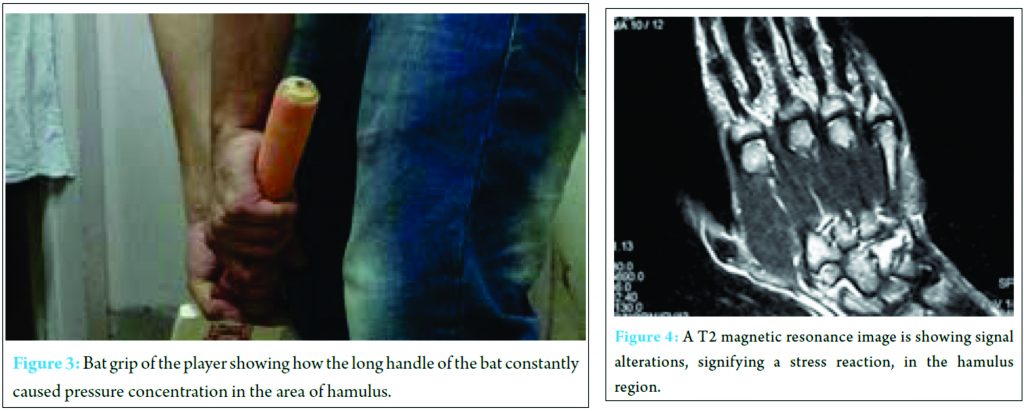
We asked the patient to bring the cricket bats he used to the clinic and his batting stance and handle grip was examined. We noted that the player used a cricket bat with an extra long handle, and the butt of the handle impinged against the ulnar side of the left wrist and the hypothenar area during batting, reproducing his symptoms (Fig. 3).
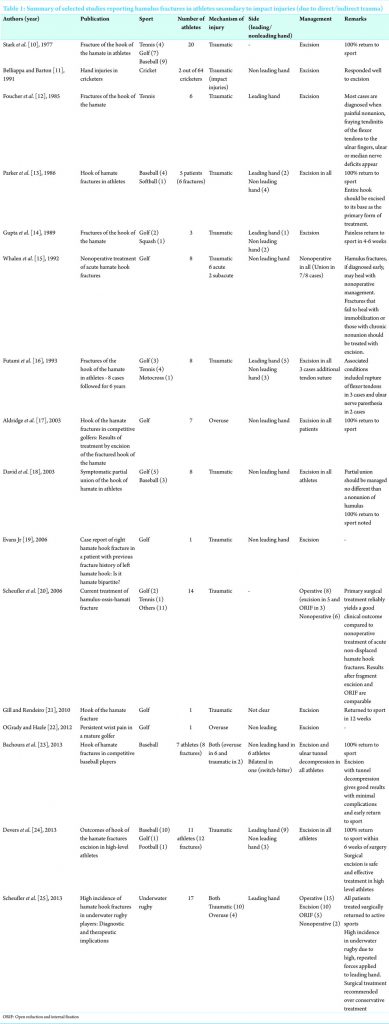
Magnetic resonance imaging demonstrated a stress fracture of the hook of the hamate; however, the fracture was not complete, and there was no evidence of any avascular necrosis of the hamate (Fig. 4). He was immobilized in a wrist brace for 4 weeks and put on a rehabilitation protocol; his bat handle and bat grip were modified to minimize pressure over the hamate region. He went back to playing the game within 12 weeks after the initiation of treatment and at 2 years follow-up, he is playing cricket at a club level without any symptoms.
Hamulus (hook of hamate) fractures comprise 2-4% of carpal fractures [5,6,7]. These fractures are usually seen in sportspersons. First described by Milch [8] in 1934, many subsequent articles in literature detail the incidence, diagnosis, management, and complications of this fracture in different sports (Table 1) [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25]. Hamulus fractures are usually seen in sports such as baseball, golf, and tennis where a bat or racquet is used by the athlete [7]. The nondominant hand is reportedly injured by swinging a baseball bat or golf club, whereas the dominant hand tends to be more at risk in tennis and other racquet sports [26].
In the sport of cricket, only 1 article has reported hamulus fractures so far [11]. Belliappa and Barton [11] reported 2 hamulus fractures in a case series of 64 hand injuries in 55 cricketers; however, these hamulus fractures were secondary to acute trauma (i.e., the impact of the upper end of the bat handle on the hand) and were not stress injuries. The mechanism of injury leading to an acute hamulus fracture continues to be controversial. Most hamulus fractures are secondary to impact injuries either due to direct trauma (caused by abutment of the hook of hamate on an object or a fall on outstretched hands) or due to an indirect trauma (due to a shearing force applied by the flexor tendon of the small and ring fingers) [9,10,13,16,17,18]. Stress fractures, on the other hand, are caused by repetitive microtrauma, most often due to the caused by racquet/bat/club and not due to a single traumatic impact injury [1]. Guha and Marynissen [1] and Van Demark et al. [4] reported stress fractures in 2 tennis players secondary to repetitive stress injury caused by the leading edge of the tennis racquet in the dominant hand which were treated conservatively; both athletes responded well to nonoperative treatment and eventually returned to tennis. Scheufler et al. [2] reported 3 stress fractures in 2 golfers and 1 tennis player (both in the leading hand) in a series of 14 hamulus fractures. Bayer and Schweizer [3] reported a case in a rock climber who repeatedly attempted dynamic swing moves in high-intensity rock bouldering (Table 2). In the case presented above, there was no definite history of any traumatic event, and the pain was insidious in onset, gradually progressed in intensity and typically was aggravated during batting sessions. Furthermore, the fact that the pain responded to rest and alterations in bat grip are retrospectively supportive of a stress injury secondary to repetitive microtrauma due to the free edge of the long bat handle impinging on the hypothenar area while executing batting strokes. Stress fractures if picked up early and treated by immobilization usually heal well allowing early return to sport [1]. If the diagnosis is delayed, the results of nonoperative treatment deteriorate, and the patient is more likely to need surgical treatment (either excision or open reduction and internal fixation [ORIF]) [2].

Management of hamulus fractures
Hamulus fractures can be treated nonoperatively with cast immobilization or operatively by ORIF (with Kirschner wires or screws) or fragment excision [6].
A high, unidentified number of hamulus fractures remain asymptomatic and either do not require or seek treatment. However, nonoperative management may lead to secondary complications such as painful nonunion, flexor digitorum profundus or superficialis tenosynovitis, and tendon rupture and is also associated with a long period of immobilization. Milek et al. reported a 15% incidence of tendon ruptures (18/257 cases) in hamulus fracture cases treated nonoperatively [27].
Excision of the hamulus is currently the preferred surgery of choice for most hand surgeons as evidenced by our literature review (Table 1); however, it leads to a reported 11% decrease in the flexor tendon excursion due to geometric factors [28]. There are also chances of residual pain,impaired sensation, and weakening of grip strength [2]. Scheufer et al. reported no significant difference in the grip strength between patients who received ORIF and those who received hamulus excision, although the grip strength values are slightly higher in the ORIF group. They hypothesized that in the young, active population who work under strenuous conditions, ORIF with screws should be preferred over hamulus excision and also over ORIF with K-wires; the reasons being better grasp, anatomic restoration of the pulley mechanism for the 4th and 5th longflexor tendons and shorter immobilization time (around 2 weeks) in ORIF with screws group [2].
Ulnar-sided pain and tenderness in players of racquet sports or those using clubs/bats have to be carefully evaluated. The dominant hand in tennis or sports involving single hand grip, and the nondominant hand in double grip sports may be the site of ulnar-sided stress concentration, leading to a stress fracture. MRI should be used to evaluate the wrist in all such cases. Nonoperative treatment, change of grip and adequate rehabilitation give good outcomes in almost all cases.
Hamulus stress fractures can occur in the non-leading hand of a cricket batsman as in other sports with a double-hand grip. The stress fracture is usually secondary to a long bat handle which leads to repeated impingement on the hook of the hamulus. Plain radiographs are usually inconclusive; MRI or bone scan is necessary to clinch the diagnosis. Non-operative treatment along with a change in the bat grip usually leads to fracture union and a good functional outcome with return to active sport. Excision of the hamate or ORIF may be needed in chronic/recalcitrant cases.
References
- 1. Guha AR, Marynissen H. Stress fracture of the hook of the hamate. Br J Sports Med 2002;36(3):224-225.1. Guha AR, Marynissen H. Stress fracture of the hook of the hamate. Br J Sports Med 2002;36(3):224-225. [Google Scholar] [PubMed]
- 2. Scheufler O, Andresen R, Radmer S, Erdmann D, Exner K, Germann G. Hook of hamate fractures: Critical evaluation of different therapeutic procedures. Plast Reconstr Surg 2005;115(2):488-497. [Google Scholar] [PubMed]
- 3. Bayer T, Schweizer A. Stress fracture of the hook of the hamate as a result of intensive climbing. J Hand Surg Eur Vol 2009;34(2):276-277. [Google Scholar] [PubMed]
- 4. Van Demark RE Jr, Van Demark RE, Helsper E. Stress fracture of the hook of the hamate: A case report. S D Med 2015;68(4):157-159, 161. [Google Scholar] [PubMed]
- 5. Bowen TL. Injuries of the hamate bone. Hand 1973;5(3):235-238. [Google Scholar] [PubMed]
- 6. Bishop AT, Beckenbaugh RD. Fracture of the hamate hook. J Hand Surg 1987;13A:135-139. [Google Scholar] [PubMed]
- 7. Rettig AC. Athletic injuries of the wrist and hand. Part I: Traumatic injuries of the wrist. Am J Sports Med 2003;31(6):1038-1048. [Google Scholar] [PubMed]
- 8. Milch H. Fracture of the hamate bone. J Bone Joint Surg 1934;16:459-462. [Google Scholar] [PubMed]
- 9. Carter PR, Eaton RG, Littler JW. Ununited fracture of the hook of the hamate. J Bone Joint Surg Am 1977;59(5):583-588. [Google Scholar] [PubMed]
- 10. Stark HH, Jobe FW, Boyes JH, Ashworth CR. Fracture of the hook of the hamate in athletes. J Bone Joint Surg Am 1977;59(5):575-582. [Google Scholar] [PubMed]
- 11. Belliappa PP, Barton NJ. Hand injuries in cricketers. J Hand Surg Br 1991;16(2):212-214. [Google Scholar] [PubMed]
- 12. Foucher G, Schuind F, Merle M, Brunelli F. Fractures of the hook of the hamate. J Hand Surg Br 1985;10(2):205-210. [Google Scholar] [PubMed]
- 13. Parker RD, Berkowitz MS, Brahms MA, Bohl WR. Hook of the hamate fractures in athletes. Am J Sports Med 1986;14(6):517-523. [Google Scholar] [PubMed]
- 14. Gupta A, Risitano G, Crawford R, Burke F. Fractures of the hook of the hamate. Injury 1989;20(5):284-286. [Google Scholar] [PubMed]
- 15. Whalen JL, Bishop AT, Linscheid RL. Nonoperative treatment of acute hamate hook fractures. J Hand Surg Am 1992;17(3):507-511. [Google Scholar] [PubMed]
- 16. Futami T, Aoki H, Tsukamoto Y. Fractures of the hook of the hamate in athletes 8 cases followed for 6 years. Acta Orthop Scand 1993;64(4):469-471. [Google Scholar] [PubMed]
- 17. Aldridge JM 3rd, Mallon WJ. Hook of the hamate fractures in competitive golfers: Results of treatment by excision of the fractured hook of the hamate. Orthopedics 2003;26(7):717-719. [Google Scholar] [PubMed]
- 18. David TS, Zemel NP, Mathews PV. Symptomatic, partial union of the hook of the hamate fracture in athletes. Am J Sports Med 2003;31(1):106-111. [Google Scholar] [PubMed]
- 19. Evans MW Jr, Gilbert ML, Norton S. Case report of right hamate hook fracture in a patient with previous fracture history of left hamate hook: Is it hamate bipartite? Chiropr Osteopat 2006;14:22. [Google Scholar] [PubMed]
- 20. Scheufler O, Radmer S, Erdmann D, Exner K, Germann G, Andresen R. Current treatment of hamate hook fractures. Handchir Mikrochir Plast Chir 2006;38(5):273-282. [Google Scholar] [PubMed]
- 21. Gill NW, Rendeiro DG. Hook of the hamate fracture. J Orthop Sports Phys Ther 2010;40(5):325. [Google Scholar] [PubMed]
- 22. O’Grady W, Hazle C. Persistent wrist pain in a mature golfer. Int J Sports Phys Ther 2012;7(4):425-432. [Google Scholar] [PubMed]
- 23. Bachoura A, Wroblewski A, Jacoby SM, Osterman AL, Culp RW. Hook of hamate fractures in competitive baseball players. Hand (N Y) 2013;8(3):302-307. [Google Scholar] [PubMed]
- 24. Devers BN, Douglas KC, Naik RD, Lee DH, Watson JT, Weikert DR. Outcomes of hook of hamate fracture excision in high-level amateur athletes. J Hand Surg Am 2013;38(1):72-76. [Google Scholar] [PubMed]
- 25. Scheufler O, Kamusella P, Tadda L, Radmer S, Russo SG, Andresen R. High incidence of hamate hook fractures in underwater rugby players: Diagnostic and therapeutic implications. Hand Surg 2013;18(3):357-363. [Google Scholar] [PubMed]
- 26. Marchessault J, Conti M, Baratz ME. Carpal fractures in athletes excluding the scaphoid. Hand Clin 2009;25(3):371-388. [Google Scholar] [PubMed]
- 27. Milek MA, Boulas HJ. Flexor tendon ruptures secondary to hamate hook fractures. J Hand Surg Am 1990;15(5):740-744. [Google Scholar] [PubMed]
- 28. Watson HK, Rogers WD. Nonunion of the hook of the hamate: An argument for bone grafting the nonunion. J Hand Surg Am 1989;14(3):486-490. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2024 Osteochondroma versus Chondrosarcoma a Diagnostic Dilemma – a Case Report
October 1, 2024 Osteochondroma versus Chondrosarcoma a Diagnostic Dilemma – a Case Report August 10, 2021 Functional Outcome of Modified Downsloping Tibial Tuberosity Osteotomy in Biplanar Opening-wedge High Tibial Osteotomy: A Case Report
August 10, 2021 Functional Outcome of Modified Downsloping Tibial Tuberosity Osteotomy in Biplanar Opening-wedge High Tibial Osteotomy: A Case Report November 10, 2018 Leiomyosarcoma of the Lower Limb Presenting as a Benign Mass: A Case Report
November 10, 2018 Leiomyosarcoma of the Lower Limb Presenting as a Benign Mass: A Case Report April 13, 2013 Traumatic Fracture in a patient of Osteopoikilosis with Review of Literature
April 13, 2013 Traumatic Fracture in a patient of Osteopoikilosis with Review of Literature