
[box type=”bio”] Learning Points for this Article: [/box]
Complete femur replacement is a rare procedure, and this case report tries to provide a guideline about the correct procedure to be followed during this complicated procedure
Case Report | Volume 7 | Issue 4 | JOCR July – August 2017 | Page 44-47| Aniruddh Agrawal, Vinod Agrawal, Sandeepkumar Yadav, Shushil K Soni, Sawan Kumar Pawar. DOI: 10.13107/jocr.2250-0685.844
Authors: Aniruddh Agrawal[1], Vinod Agrawal[2], Sandeepkumar Yadav[2], Shushil K Soni[2], Sawan Kumar Pawar[2]
[1] Ark Hospital, Andheri West, Mumbai, Maharashtra. India.
[2] Department of Orthopedics, Lilavati Hospital, Bandra Reclamation, Mumbai, Maharashtra. India.
Address of Correspondence
Dr. Aniruddh Agrawal,
Ark Hospital, 401 Sony House, CD Barfiwala Road, Andheri (W), Mumbai – 400 056, Maharashtra. India.
E-mail: anirudhagrawal25@gmail.com
Abstract
Introduction: Total femur arthroplasty (TFA) is a rare salvage limb procedure which serves as an effective alternative to limb amputation. Most commonly, it is indicated for oncologic orthopedic cases, and very few cases of a purely traumatic history for TFA have been documented. The decision to perform this complex procedure involves paying careful attention to reconstructive needs and functional expectations of the patient. Alternatives to this procedure are quite detrimental and include hip disarticulation and above-the-knee amputation.
Case Report: A 66-year-old woman with a history of hypertension, and parkinsonism was brought into the outpatient department of a tertiary care hospital. She has undergone a procedure for proximal femur nailing on her left hip in 2013 due to a trauma-related fracture. However, after the development of a series of complications, she underwent revision surgery on her left hip 6 times by different surgeons. This included surgeries for implant removal and fixation of a custom-made bipolar hemi-replacement hip, followed by a cemented bipolar hip hemi-replacement with plating and cerclage wires followed by infection, the treatment of which entailed implant removal and placement of an antibiotic cement. This was followed by a long stem constrained cemented total hip arthroplasty which also failed. The surgeon then made the decision to perform a TFA. 12-month follow-up post-operatively showed neither peri-prosthetic infection or inflammation nor any leg length discrepancy. The functional outcome on lower extremity function scale showed improvement from 0 pre-operatively to 31 at 12-month follow-up.
Conclusion: TFA serves as a viable technique for salvage of the lower extremity in cases of infected non-unions. However, a thorough evaluation of the particular case in the hand should be made before reaching a conclusion.
Keywords: Complete femur arthroplasty, revision surgery, multiple surgery failure, dual incision technique
Introduction
Total femur arthroplasty (TFA) is a complex limb salvage procedure that is used as an alternative to lower extremity amputation. It is indicated mainly in cases of orthopedic oncology [1, 2], but the evidence of cases performed following traumatic incidence and failure of ipsilateral total hip and total knee arthroplasties remains low [3]. TFA has shown to continually evolve since its first documented case in the mid-20th century and has shown to restore femoral integrity and allow patients to restore ambulation [4]. Mechanical limitations of the implant design and the complexity associated with surgical technique have contributed to most of these cases being reported as isolated case studies [4, 5] with only a few documented case series [6, 7]. The decision to perform this complex procedure involves paying careful attention to reconstructive needs and functional expectations of the patient. Alternatives to this procedure are quite detrimental and include hip disarticulation and above-the-knee amputation. It is necessary for surgeons to weigh in all clinical factors to ensure that the surgical goal of long-term ambulatory effect is met. As in the case being presented in this article, there seems to be a rise in the number of revision arthroplasties which could correspond to an increase in salvage arthroplasty [8]. Multiple revision surgeries predispose the patient to the excessive bone loss which warrants partial or complete resection and replacement of the affected bone, in this case, the femur [9]. However, the literature reporting a favorable outcome for TFA has been on the rise. Clement et al. [10] reported an implant survival rate of 86% at a 10-year follow-up for patients who underwent TFA for extensively comminuted peri-prosthetic fractures. Amanatullah et al. [11] reported a 70% implant survival rate at 5-year follow-up in 20 patients, whereas Berend et al. [3] reported a 65% implant survival rate in 59 patients at a 5-year follow-up. However, certain drawbacks of complete femur replacement include prolonged operative time which can increase the risk of intraoperative wound contamination with subsequent development of peri-prosthetic infection [12]. The extensive dissection required for the procedure would also result in increased volume of blood loss. However, reports have indicated that sub-peritoneal dissection would help to minimize the bleeding [7]. It is important that a surgeon considers these drawbacks while evaluating a patient for a TFA surgery.
Case Report
A 66-year-old woman with a history of hypertension and parkinsonism was brought into the outpatient department of a tertiary care hospital. She had a surgical history of 6 procedures performed in the lower left extremity due to trauma-related fracture. Initial surgery was performed due to the appearance of inter- and sub-trochanteric extension fracture of the left femur as a result of trauma related to a fall at her residence. This surgery entailed the placement of proximal femur nailing (PFN) in August 2013 (Fig. 1).4-month post-operatively, it was determined that the PFN surgery had failed (Fig. 2), and therefore, the patient underwent a second surgery for implant removal and fixation of a custom-made bipolar hemi-replacement hip (Fig. 3). Post-operatively, the patient had a fall and incurred a peri-prosthetic fracture and bending of the implant, which was later treated with a cemented bipolar hip hemi-replacement with plating and cerclage wires (Fig. 4). 6-month post-operatively, the implant got infected (Fig. 5) and culture showed Gram-positive cocci which proved to be very difficult to eliminate, and hence, the patient underwent surgery for the fourth time, which entailed implant removal and placement of an antibiotic cement spacer to ensure clearance of the infection (Fig. 6).
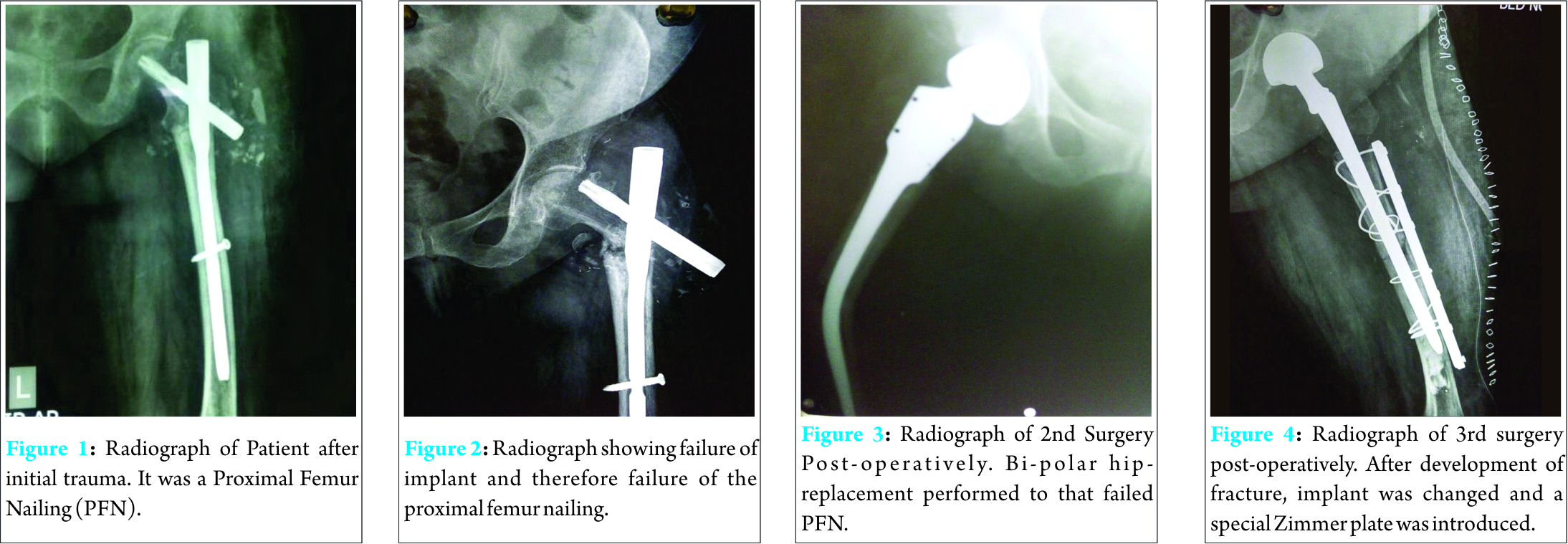 Post-operatively, the patient required one debridement procedure and further intravenous antibiotic coverage for 2 months. After testing, blood culture was shown to be negative, and inflammatory markers including complete blood count, erythrocyte sedimentation rate, C-reactive protein, and procalcitonin were in their normal physiological range. These tests allowed surgeons to carry out the sixth surgery which entailed long stem constrained cemented total hip arthroplasty (Fig. 7). After this surgery, no signs of inflammation or infection were observed. The surgeon determined that the range of movement was satisfactory and the patient had found it comfortable to perform daily routine activities such as sitting on the chair and standing and walking without any support. However, post-operatively after 8 months, the patient started complaining of pain in the left thigh, there was apparent swelling in the mid-thigh region, and she was unable to bear her full weight on that leg. On clinical examination, a bony protuberance was observed in the middle of the left thigh, and the patient complained of painful movement. Radiographic examination showed cemented femoral stem and severe bone loss (Fig. 8).
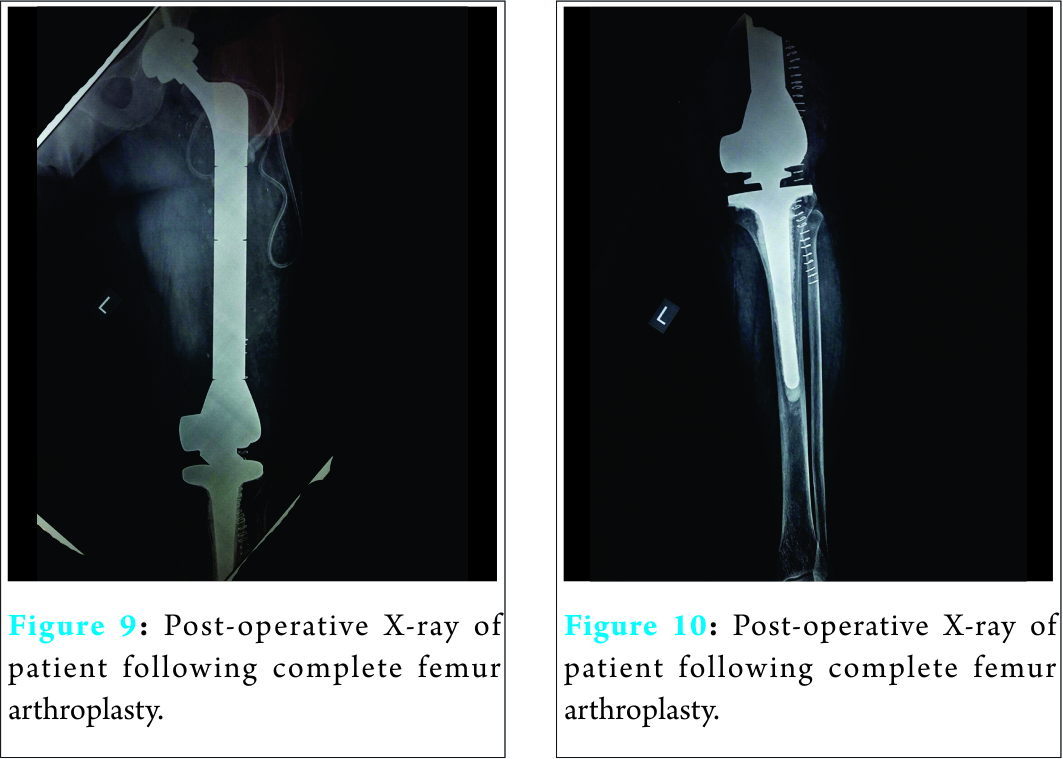
Post-operatively, the patient required one debridement procedure and further intravenous antibiotic coverage for 2 months. After testing, blood culture was shown to be negative, and inflammatory markers including complete blood count, erythrocyte sedimentation rate, C-reactive protein, and procalcitonin were in their normal physiological range. These tests allowed surgeons to carry out the sixth surgery which entailed long stem constrained cemented total hip arthroplasty (Fig. 7). After this surgery, no signs of inflammation or infection were observed. The surgeon determined that the range of movement was satisfactory and the patient had found it comfortable to perform daily routine activities such as sitting on the chair and standing and walking without any support. However, post-operatively after 8 months, the patient started complaining of pain in the left thigh, there was apparent swelling in the mid-thigh region, and she was unable to bear her full weight on that leg. On clinical examination, a bony protuberance was observed in the middle of the left thigh, and the patient complained of painful movement. Radiographic examination showed cemented femoral stem and severe bone loss (Fig. 8).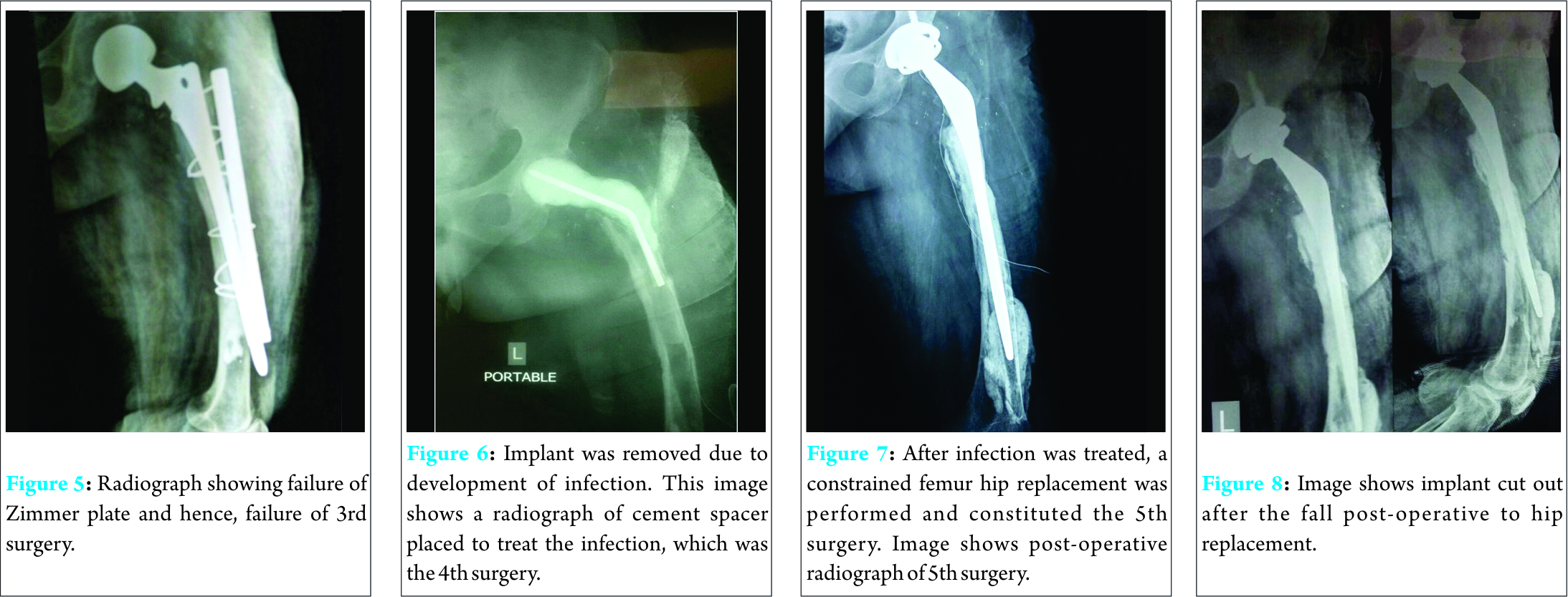 A test for blood inflammatory markers was performed again and was shown to be normal. The patient was also advised above knee amputation or disarticulation of the hip joint. At this time, the author of this paper determined that the patient required a seventh surgery and after careful deliberation determined that it would be a TFA. Although the surgical technique involving a direct lateral approach which is used to expose the entire femur and proximal tibia, utilizing a lateral parapatellar approach at the knee and the posterior approach at the hip has been demonstrated, the author preferred to use the dual approach which involves a medial parapatellar approach at the knee and a choice of extendable approach at the hip (Fig. 9, 10) [7].
A test for blood inflammatory markers was performed again and was shown to be normal. The patient was also advised above knee amputation or disarticulation of the hip joint. At this time, the author of this paper determined that the patient required a seventh surgery and after careful deliberation determined that it would be a TFA. Although the surgical technique involving a direct lateral approach which is used to expose the entire femur and proximal tibia, utilizing a lateral parapatellar approach at the knee and the posterior approach at the hip has been demonstrated, the author preferred to use the dual approach which involves a medial parapatellar approach at the knee and a choice of extendable approach at the hip (Fig. 9, 10) [7].
The patient was shifted to the intensive care unit post-operatively for cardiovascular, respiratory, neurological, and post-operative pain monitoring. The patient was kept in abduction with an abduction pillow, was allowed to remain in weight-bearing postures as tolerable, and was also allowed to walk with a long knee brace, a walker, and some assistance from the nurses. Post-operative radiographs showed no immediate complications such as fracture, dislocation, or an inappropriate alignment. 2 days post-operatively, the patient was asked to perform bed exercises with assisted knee bending of 20°-30°. 5 days post-operatively, the patient was mobilized with a long knee brace and walker. The patient progressed well and was discharged from the tertiary care hospital 9 days post-operatively. Regular follow-ups were planned for this patient. For evaluation of functional scores, the lower extremity function scale (LEFS) was used before and after the surgery [13]. Pre-operatively, the patient was confined to a wheelchair and reported a LEFS score of 0, and after 12-month follow-up, the patient reported a LEFS score of 31.
Surgical technique
Before surgery, it is essential to explain the complexity of the surgery to the patient, including alternative treatments and the risks involved, such as the need for revision of their total femur prosthesis. Patients should understand that this procedure will not return them to a normal status and that they may require an assistive device, such as a walker or crutch for the remainder of their lives. Before surgery, it is necessary to perform a pre-operative evaluation to medically optimize the patient for surgery. The patient positioned in semi-lateral position. Begin the surgery with midline incision over the knee for knee arthroplasty. All tibial preparation according to constrained knee joint and long stem was done first. Another the skin incision over the previous scar which was taken for previous total hip replacement (THR). During the dissection to reach the hip, a lot of fibrosis was observed around the hip joint. We were unable to observe any normal anatomy. With the help of electrocautery and careful dissection, we were able to completely expose the acetabular margin of the femoral component. All muscular and soft tissue attachments of the femur were cleared circumferentially with careful attention to the neurovascular structures. Now, meticulous dissection started from the second incision for the distal femur. All anterior, posterior, medial, and lateral attachments were cleared by subperiosteal dissection with special care to structures around the popliteal fossa. The proximal and distal incision was connected by making a tunnel around femur. The previous THR was constrained and acetabular cup radiologically and intraoperatively seemed to be stable, no loosening of implant was found so only femoral implant along with the head and liner was removed. After stem and distal femur removal, we found that the distal femur bone was only around 10 cm long and the long femoral stem was fixed by bone cement only. The total length of implant was calculated by pre-operative X-rays and again confirmed intraoperatively by comparison with removed bone and implant. Trial was performed by passing the endoprosthesis through a tunnel. Acetabular liner was fixed for the constrained hip. Stability of both joints and length of endoprosthesis were checked. After trial, the tibial component was fixed with cement, the femoral head was reduced, liner ring was impacted for constrained hip, and then, the constrained knee joint with a rotating platform was fixed. Again stability of both joints and stretching of the neurovascular structure was assessed. After pulse lavage, abductor muscular tissue was attached to the hole given in the trochanteric area of the endoprosthesis; then, closure was performed with two drains. Post-operative radiographs showed no immediate complications such as fracture, dislocation, and appropriate alignment. 2 days after surgery, the patient was given in bed exercises with assisted knee bending to 20°-30°. Moreover, 5 days after surgery, the patient was mobilized with long knee brace and walker with the help of nursing staff and physiotherapist. The patient progressed well and was discharged from hospital 9 days after surgery with proper instruction including those of physiotherapy exercises as well as general follow-up advice. 3 months postoperatively, the patient is clinically well and ambulating with the help of a walker.
Discussion
The incidence of TFA is rare, and TFA in cases of purely non-oncologic cases is even rarer. This procedure requires careful pre-operative planning which involves identification of the cause of implant failure, standard infection screening serum blood tests, examination of soft tissues to ensure adequate soft tissue coverage of the prosthesis, as well as evaluation of lower extremity motor strength. Pre-operative imaging of standard and lateral views of the pelvis, hip, femur, and knee lay the foundation for evaluating current implants and amount of remaining bone. Although intraoperative blood loss remains a viable concern, recent technological advancements such as intraoperative blood salvage, bipolar sealing device, and argon beam coagulation may assist with hemostasis [14, 15, 16]. Peri-prosthetic infection has also become a rising cause of concern among surgeons; however, at a 12-month follow-up, this patient showed no signs of any inflammation or infection in blood tests. Morimoto et al. [17] reported a rate of 12% in 100 patients who underwent TFA. Another cause of concern which was not observed in this patient post-operatively is hip instability which causes recurrent dislocations. Another potential complication is limb length discrepancy which may require revision surgery entailing exchange of modular components of the TFA implant to shorten or lengthen it accordingly. Less common complications requiring another revision surgery include mechanical failure of implant, loosening of the acetabular or the tibial component, complications involving the patella, and difficulty with wound healing. None of these was observed in the patient after 12 months of follow-up. In cases not involving malignancy, bone stock and soft tissue preservation, when possible, are of the utmost importance. As this patient underwent surgery multiple times, neither the muscle attachments nor the soft tissue planes were clearly demarcated.
Conclusion
TFA, although complex, remains a viable solution as a salvage procedure in the treatment of infected non-union of fractures. The dual-incision approach to this complicated procedure produced good results in this case. However, this procedure should only be considered after all other treatment modalities have failed. The risk-benefit ratio should be thoroughly evaluated.
Clinical Message
TFA remains a very complex and relatively infrequently indicated surgical procedure with a horde of complications surrounding it intraoperatively as well as post-operatively. It is important for the surgeon as well as the patient to understand the various complications associated with this procedure so that both of them are prepared for whatever post-operative outcome is observed. Keeping in mind the need for meticulous dissection and tissue handling, only experienced surgeons should opt for using this technique.
References
1. Kalra S, Abudu A, Murata H, Grimer RJ, Tillman RM, Carter SR. Total femur replacement: Primary procedure for treatment of malignant tumours of the femur. Eur J Surg Oncol 2010;36(4):378-383.1. Kalra S, Abudu A, Murata H, Grimer RJ, Tillman RM, Carter SR. Total femur replacement: Primary procedure for treatment of malignant tumours of the femur. Eur J Surg Oncol 2010;36(4):378-383.
2. Ahmed AR. Total femur replacement. Arch Orthop Trauma Surg 2010;130(2):171-176.
3. Berend KR, Lombardi AV Jr, Mallory TH, Adams JB, Dodds KL. Total femoral arthroplasty for salvage of end-stage prosthetic disease. Clin Orthop Relat Res 2004;427:162-170.
4. Buchman J. Total femur and knee joint replacement with a vitallium endoprosthesis. Bull Hosp Joint Dis 1965;26:21-34.
5. Steinbrink K, Engelbrecht E, Fenelon GC. The total femoral prosthesis. A preliminary report. J Bone Joint Surg Br 1982;64(3):305-312.
6. Friesecke C, Plutat J, Block A. Revision arthroplasty with use of a total femur prosthesis. J Bone Joint Surg Am 2005;87(12):2693-2701.
7. Lombardi AV Jr, Berend KR. The shattered femur: Radical solution options. J Arthroplasty 2006;21 4 Suppl 1:107-111.
8. Kurtz SM, Ong KL, Lau E, Bozic KJ. Impact of the economic downturn on total joint replacement demand in the United States: Updated projections to 2021. J Bone Joint Surg Am 2014;96(8):624-630.
9. Fountain JR, Dalby-Ball J, Carroll FA, Stockley I. The use of total femoral arthroplasty as a limb salvage procedure: The Sheffield experience. J Arthroplasty 2007;22(5):663-669.
10. Clement ND, MacDonald D, Ahmed I, Patton JT, Howie CR. Total femoral replacement for salvage of periprosthetic fractures. Orthopedics 2014;37(9):e789-e795.
11. Amanatullah DF, Trousdale RT, Hanssen AD, Lewallen DG, Taunton MJ. Non-oncologic total femoral arthroplasty: Retrospective review. J Arthroplasty 2014;29(10):2013-2015.
12. Davis N, Curry A, Gambhir AK, Panigrahi H, Walker CR, Wilkins EG, et al. Intraoperative bacterial contamination in operations for joint replacement. J Bone Joint Surg Br 1999;81(5):886-889.
13. Binkley JM, Stratford PW, Lott SA, Riddle DL. The Lower Extremity Functional Scale (LEFS): Scale development, measurement properties, and clinical application. North American Orthopaedic Rehabilitation Research Network. Phys Ther 1999;79(4):371-383.
14. Ashworth A, Klein AA. Cell salvage as part of a blood conservation strategy in anaesthesia. Br J Anaesth 2010;105(4):401-416.
15. Kaibori M, Matsui K, Ishizaki M, Sakaguchi T, Matsushima H, Matsui Y, et al. A prospective randomized controlled trial of hemostasis with a bipolar sealer during hepatic transection for liver resection. Surgery 2013;154(5):1046-1052.
16. Go PM, Goodman GR, Bruhn EW, Hunter JG. The argon beam coagulator provides rapid hemostasis of experimental hepatic and splenic hemorrhage in anticoagulated dogs. J Trauma 1991;31(9):1294-1300.
17. Morimoto S, Futani H, Ogura H, Okayama A, Maruo S. Successful reimplantation of total femoral prosthesis after deep infection. J Arthroplasty 2003;18(2):216-220.
 |
 |
 |
 |
 |
| Dr. Aniruddh Agrawal | Dr. Vinod Agrawal |
Dr. Sandeep Kumar Yadav | Dr. Sushil Soni | Dr. Sawan Kumar Pawar |
| How to Cite This Article: Agrawal A, Agrawal V, Yadav S, Soni SK, Pawar SK. A Case Report of Dual Incision Technique for Total Femur Arthroplasty as a Salvage Procedure in Infected Non-Unions. Journal of Orthopaedic Case Reports 2017 Jul-Aug;7(4):44-47 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


